Dr. Joseph John, J14619, Dr. Elizabeth Joseph
ABSTRACT
AIM :
To assess the effectiveness of Botulinum Toxin(BT) in isolated acquired lateral rectus palsy
MATERIALS AND METHODS:
Prospective interventional controlled trial; we gave BT to ipsilateral medial rectus under topical anaesthesia without electromyographic guide. We enrolled age matched controls. We gave systemic steroids to both groups and followed them 10, 30, 60, 120, 180 days after initiating treatment. We recorded head posture, primary deviation in primary position, limitation of abduction, and diplopia chart on all visits.
RESULTS:
10 cases and 10 age matched controls were enrolled in the study. After 10 days of injection, 100% cases had primary deviation less than 10 prism diopters and no diplopia in primary position. After 30 days, 80% cases had partial recovery of abduction.
CONCLUSION:
Botulinum Toxin is effective in achieving early subsidence of diplopia in primary position and early recovery of abduction in patients presenting with isolated lateral rectus palsy.
Introduction
Botulinum toxin Type A is one of the seven serotypes produced by the anaerobic bacteria Clostridium botulinum1,2. The toxin interferes with acetylcholine release from nerve endings by antagonization of serotonin-mediated calcium ion release. Botulinum toxin, injected into the ipsilateral medial rectus muscle, has been advocated in the management of acute sixth nerve palsy or paresis.
In conservatively managed cases, contracture of the medial rectus muscle may prevent complete resolution of diplopia despite complete recovery of lateral rectus muscle function. Botulinum toxin reduces contracture of the medial rectus muscle and allows for more complete restoration of ductions3.
Aim
To assess the effectiveness of Botulinum toxin in patients presenting with isolated lateral rectus palsy.
Materials and Methods
This study was approved by the Institutional Review Board, Clinical Research Ethics Committee before performing this study. After explaining to the patients the purpose of the study and the possible outcomes, informed consent was obtained from all patients. The procedures conformed to the tenets of the Declaration of Helsinki. This is a prospective, interventional, controlled trial done from March 2012 to March 2015.
The inclusion criteria were: acquired lateral rectus palsy, no other neurological defects, normal Magnetic Resonance Imaging scan and age >30 years. After explaining to the patient about the two modes of intervention they were allowed to choose one mode. The cases were treated with 15 units of Botulinum toxin. All the patients, that is, the cases and controls were given intravenous betamethasone for 3 days changed to oral steroids on tapering doses. All patients were advised part time occlusion of the fellow eye and were followed up 10, 30, 60, 120, 180 days after initiating treatment.
Head posture, primary deviation in primary position, limitation of abduction and presence of diplopia in primary position were noted at baseline and at each follow up visit. Head posture was measured with the help of protractor while the patient is fixing at a distance of 6 metres. The angle of deviation was measured in prism dioptres by simultaneous prism and cover test in the primary position at a distance of 6 metres.
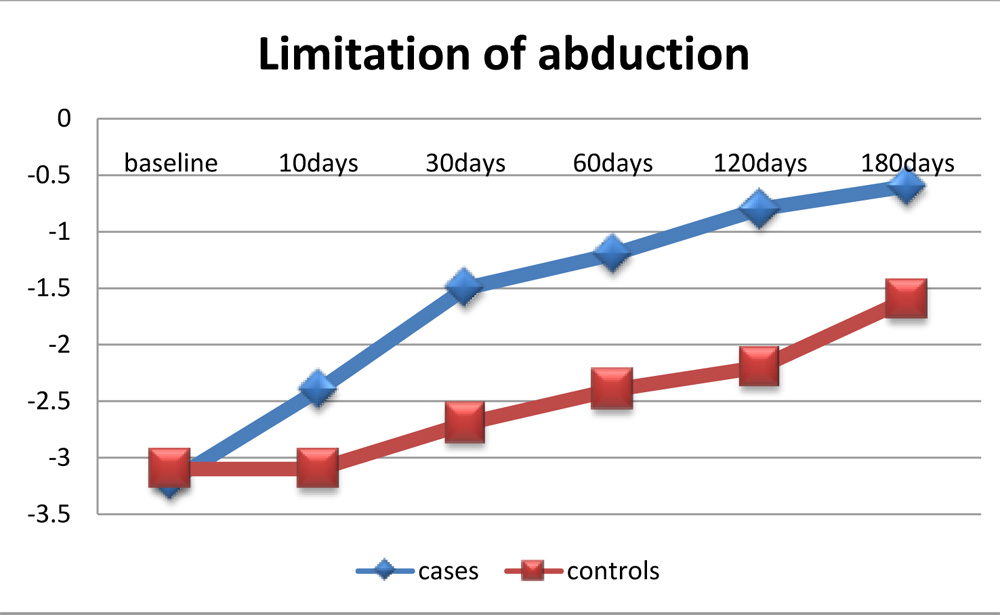
Abduction deficit was recorded on the scale described by Scott and Kraft4: zero (normal), –1 (to 75% full rotation), –2 (to 50% full rotation), –3 (to 25% full rotation), –4 (to midline), and –5 (inability to abduct to the midline). Diplopia chart was recorded using red –green goggles and yellow streak and presence of diplopia in primary position was recorded.
Method of reconstitution of Botulinum toxin, Botox (Allergan, Irvine, CA)
Each vial of Botox contains 50 units of Botulinum toxin which is reconstituted with 2ml normal saline so that 0.1 ml contains 2.5 units. It is used within 1 hour2.
Method of administration of Botulinum toxin
The surgical field was prepared, the medial rectus insertion grasped firmly with forceps and the eye rotated to the primary position. Botulinum toxin was injected 5 mm from the medial rectus insertion, inside the bulk of muscle through a 27 gauge needle with tuberculin syringe (without electromyography guide) under topical anaesthesia. No peritomy was done.
Statistical analysis
Wilcoxon signed-rank test was used for paired samples; Mann-Whitney U test for independent samples; p value < 0.05 was taken as statistically significant.
Results:
10 cases (6 females) were enrolled in the study. 10 age matched controls (6 females) were also enrolled. All except one case had diabetes mellitus. The baseline characteristics of cases and controls (Table 1) were comparable in terms of duration of symptoms (p=0.56), head posture (p=1), primary deviation in primary position (p=0.79) and limitation of abduction (p=0.84). One case required a repeat injection of 10 units of Botulinum toxin after ten days. After 10 days of injection 100% cases attained primary deviation less than 10 prism diopters and subsidence of diplopia in primary position and 50% cases showed partial recovery of abduction (Table 2).
Figure 1 showing method of administration of Botulinum toxin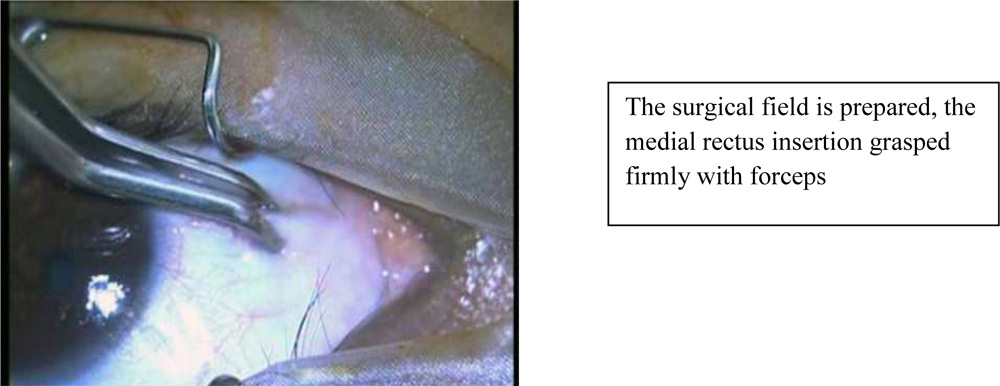
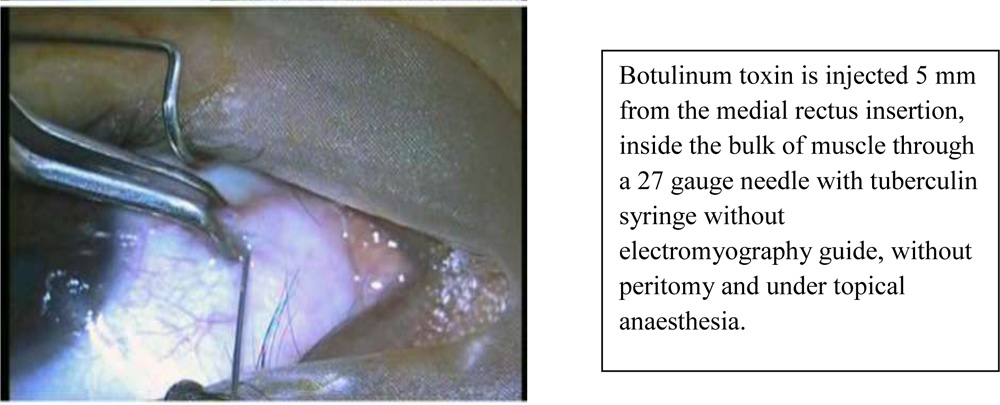
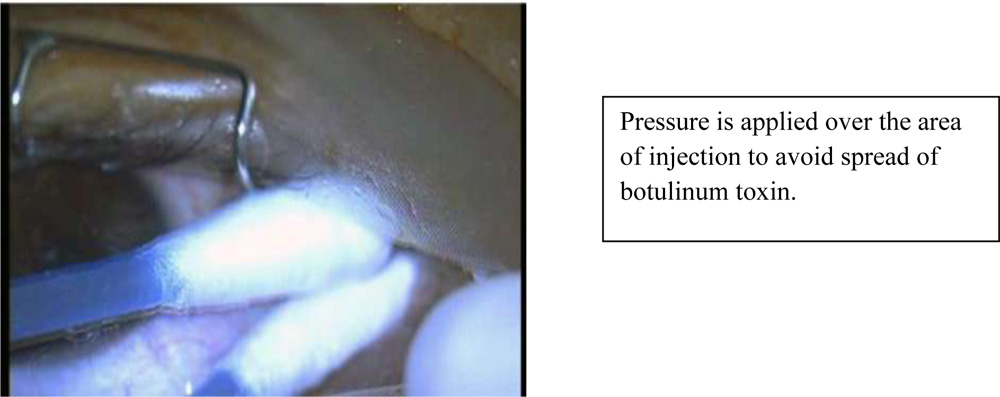
Table 1 :Baseline characteristics of patients
| Cases
N=10 |
Controls
N=10 |
Mann Whitney U test
P value |
|
| Age (years) | 59.1±5.8 | 58.2±6.0 | 0.65 |
| Duration of symptoms(days) | 6.3±2.1 | 6.8±2.1 | 0.56 |
| Head posture (degrees) | 44±11 | 44±11 | 1 |
| Primary deviation (prism diopters) | 37±12 | 39±15 | 0.79 |
| Limitation of abduction | -3.2±0.9 | -3.1±1 | 0.84 |
Table 2 :Improvement in botulinum toxin group
| 10 days | 30 days | |
| Primary deviation at primary position
< 10 prism diopters |
100% | 100% |
| Subsidence of diplopia in primary position | 100% | 100% |
| Recovery of abduction
(partial) |
50% | 80% |
Head posture improved from 44+/-11 degrees at baseline to 21+/-7 degrees after 10 days (p=0.002) and to 18+/-6 degrees (p=0.002) after 30 days. Primary deviation at primary position improved from 37+/-12 prism diopters at baseline to 6+/-2 prism diopters after 10 days (p=0.002). The limitation of abduction decreased from -3.2+/-0.9 at baseline to -2.4+/-1.8 after 10days (p=0.05) and to -0.7+/-1.2 (p=0.002) after 30 days.
Table 3:Changes during follow-up in cases
| Cases | Baseline | 10days | p | 30days | p |
| Head posture (degrees) | 44±11 | 21±7 | 0.002 | 18±6 | 0.002 |
| Primary deviation at primary position
(prism diopters) |
37±12 | 6±2 | 0.002 | 4±2 | 0.001 |
| Limitation of abduction | -3.2±0.9 | -2.4±1.8 | 0.05 | -0.7±1.2 | 0.002 |
Table 4:Changes during follow-up in controls
| Controls | Baseline | 10days | p | 30days | p |
| Head posture (degrees) | 44±11 | 44±11 | NA | 32±13 | 0.0078 |
| Primary deviation at primary position
(prism diopters) |
39±15 | 36±16 | 0.0625 | 26±10 | 0.002 |
| Limitation of abduction | -3.1±1 | -3.1±1 | NA | -2.7±1.3 | 0.13 |
After 30 days, 80% cases showed partial recovery of abduction. Controls attained primary deviation less than 10 prism diopters and subsidence of diplopia in primary position after 150 days (range 120-180 days). Table 3 and 4 summaris the changes during follow up in cases and controls. Figures 1,2,3 compare changes in various parameters among cases and controls.
Other than mild subconjunctival haemorrhage, there were no adverse events recorded in the study
Figure 2 : Improvement in head posture in cases and controls
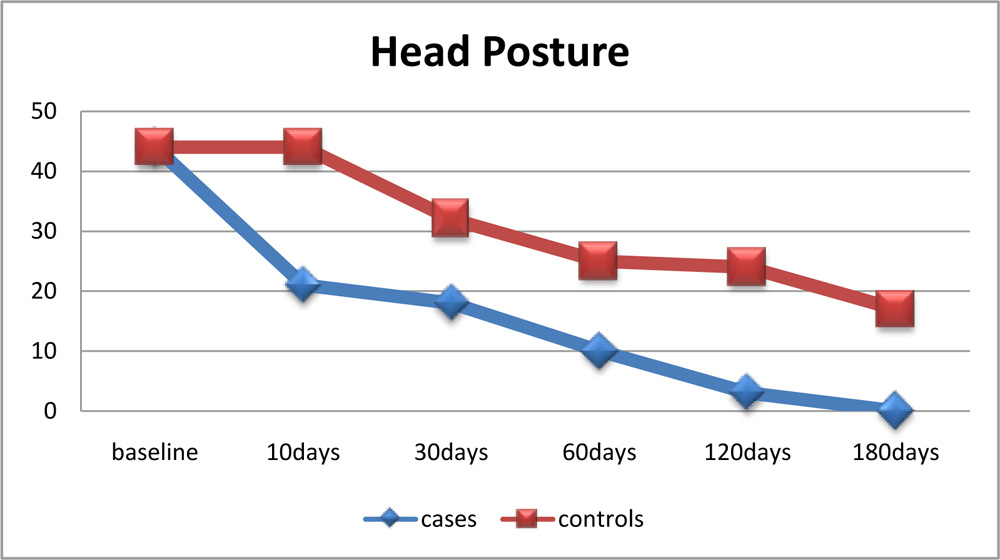
Figure 3: Variation in primary deviation in cases and controls
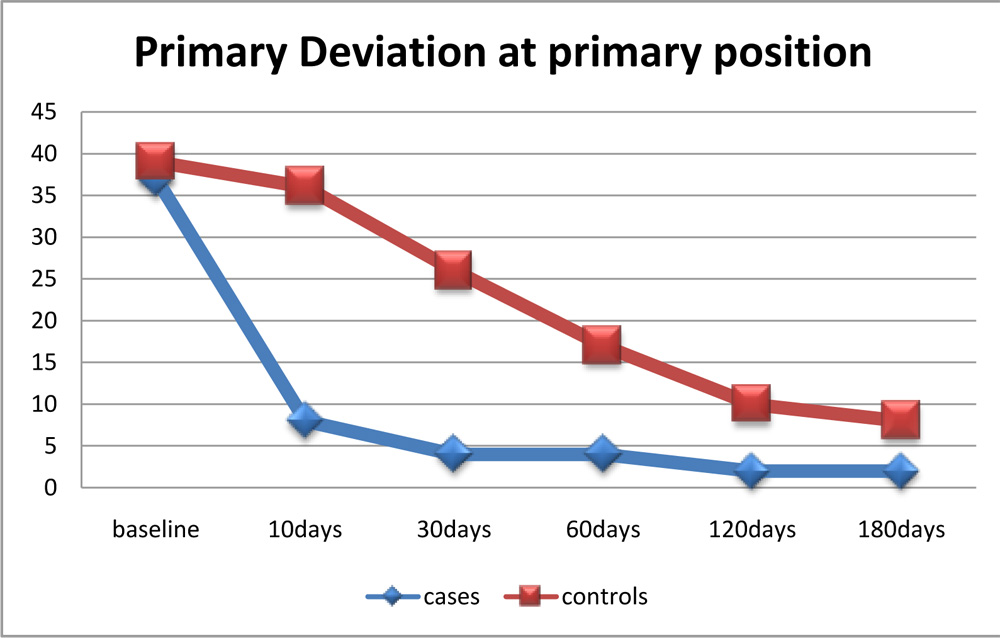
Figure 4: Improvement in abduction in cases and controls
Discussion
In a study conducted by Holmes JM et al and the Pediatric Eye Disease Investigator Group on Botulinum Toxin Treatment Versus Conservative Management in Acute Traumatic Sixth Nerve Palsy or Paresis, the recovery rate was high and similar in patients who received Botulinum toxin within 3 months of injury (73%) and in those who were treated conservatively (71%)4.
In another study on etiology and treatment of pediatric sixth nerve palsy, Merino P et al found out that Botulinum toxin was successful in 70% of cases5.
In our study, the cases attained 100% subsidence of diplopia and primary deviation <10 prism diopters in primary position within 10 days whereas the controls took 120 to 180 days for the same.
In a study on the necessity of electromyographic assistance in Botulinum toxin injection, Sanjari MS et al concluded that the effectiveness of botulinum toxin injection is the same with or without electromyographic assistance in the treatment of abducens nerve palsy6. This is in accordance with our study.
This study has some limitations. The recruitment of patients into cases and controls were not randomised.
Conclusion
Botulinum toxin is effective in achieving early subsidence of diplopia in primary position and early recovery of abduction in patients presenting with isolated lateral rectus palsy.
References
- Dutton JJ, Fowler AM. Major Review- Botulinum Toxin in Ophthalmology. Surv Ophthalmol 2007:52:13-31.
- Diamond GR; Chapter 11.13 – Forms of Nonsurgical Strabismus Management; In: Yanoff M, Duker JS, editors. Yanoff & Duker Ophthalmology, 3rd ed. Philadelphia: Elsevier/Mosby Publishing.
- Rubin SE; Chapter 11.10 – Paralytic Strabismus; In: Yanoff M, Duker JS, editors. Yanoff & Duker Ophthalmology, 3rd ed. Philadelphia: Elsevier/Mosby Publishing.
- Holmes JM, Beck RW, Kip KE, Droste PJ, Leske DA, and the Pediatric Eye Disease Investigator Group (PEDIG). Botulinum Toxin Treatment Versus Conservative Management in Acute Traumatic Sixth Nerve Palsy or Paresis. J AAPOS 2000;4:145-9.
- Merino P, de Liano PG, Villalobo JMC, Franco G, de Liano RG. Etiology and treatment of pediatric sixth nerve palsy. J AAPOS 2010;14:502-505.
- Sanjari MS, Falavarjani KG, Kashkouli MB, Aghai GH, Nojomi M, Rostami H. Botulinum toxin injection with and without electromyographic assistance for treatment of abducens nerve palsy: A pilot study. J AAPOS 2008;12:259-262.