Dr. Amrita Sawhney, S17593, Dr.Shaloo Bageja, Dr. Ashok Kumar Grover, Dr. Harsh Rathod
Dr. Amrita Sawhney, Dr. A.K. Grover, Dr. Shaloo Bageja, Dr.Harsh
Purpose :
a)To show the wide spectrum of clinical manifestations in nine cases of orbital IgG4 –related disease (IgG4-RD) along with their epidemiological, radiological, laboratory and histological data. b) To evaluate the clinical outcomes of the disease with the targeted therapies like immunosuppressants and rituximab.
Immunoglobulin G4-related disease is a relatively newly defined emerging entity which is characterized by mass forming lesion, lymphoplasmacytic infiltration rich in IgG4 positive plasma cells and raised IgG4 levels in 60-70 % cases.1 It was first identified in a group of patients with autoimmune pancreatitis with raised serum IgG4 levels2 and was recognized as a systemic condition in 2003.3
IgG4 –RD can involve several organs of the body including the orbit, lymph nodes, skin, lungs, salivary glands, thyroid, aorta, biliary tract, breast, kidneys, retroperitoneum, and CNS. The orbit is the most common extrapancreatic site to be involved by this disease entity.4 The most frequently involved site in IgG4 –related orbital disease is the lacrimal gland (IgG4 –related dacryoadenitis). Other sites in the orbit that can be involved are the extraocular muscles (IgG4 –related orbital myositis), the orbital soft tissue (IgG4 related orbital inflammation), the eyelids and the orbital nerves. Orbital IgG4 –related disease is predominantly seen in adults with no gender predilection.5
Microscopic features which are characteristic of IgG4–RD are lymphoplasmacytic infiltrate (predominantly T-lymphocytes), a storiform/cartwheel pattern of fibrosis and obliterative phlebitis. However, in lacrimal gland involvement both storiform fibrosis and obliterative phlebitis may not be present.
Diagnostic criteria include : 1)Clinical presentation – diffuse or localized mass in single or multiple organs, 2) Serum IgG4 concentration >135mg/dl and 3) Histopathological features consisting of – a) fibrosis and lymphoplasmacytic infiltration b) IgG4/ IgG ratio >40 % and > 10 IgG4 cells/HPF . According to these criteria IgG4-RD can be labeled as – Definite disease : 1+2+3, possible disease : 1+2, probable disease : 1+3.
Long term followup is required as there is a risk of recurrence and development of lymphoma.
Materials and method
Nine patients were diagnosed from 2012-2016 on the basis of published diagnostic criteria for IgG4 related disease. Their epidemiological profile (including age and sex), presenting complaints, laboratory results(CRP, ESR and serum IgG4), orbital imaging and histopathological findings were recorded.
All the patients were started on oral steroids to begin with. Azathioprine was used as a steroid sparing agent. Two patients with resistant disease were given rituximab.
Results
We diagnosed nine cases of IgG4 related orbital disease from 2012-2016.
The average age at presentation in our study was 50 years (20-68years) with a male:female ratio of 1.2:1 (5 males and 4 females).
Clinical presentations included swelling of upper lid due to dacryoadenitis in 5/9 cases (Figure 1)(unilateral-3, bilateral-2), proptosis with extraocular muscles or intraconal fat involvement in 2/9 cases (Figure 2), proptosis with lid swelling due to both lacrimal gland and extraocular muscle involvement in 2/9cases (Figure 3).
Serum IgG4 level was raised in 7 /9 cases.
The histopathological diagnosis was based on IgG4 positive plasma cells with fibrosis. (Figure 4)
Systemic involvement including mediastinal lymphadenopathy and hepatosplenomegaly was seen in 1/ 9 cases.
The number of cases diagnosed as definite, probable and possible IgG4 related orbital disease were 3,2 and 4 respectively.
In our study, 7/9 patients had good and stable clinical outcomes with steroids and azathioprine. However, 2/9 patients were given rituximab (1gm iv to be repeated after 15 days, total two doses) as there was resistance to steroids. Both the patients had better clinical outcomes after rituximab therapy.
Table 1: Shows epidemiology, presenting complaints and laboratory results .
| S.NO | AGE/SEX | IgG4-RD TYPE | PRESENTING COMPLAINTS | CRP
(mg/l) |
ESR
(mm/hr) |
Serum IgG4 LEVELS |
| 1. | 55/female | Bilateral dacryoadenitis | Bilateral upper eyelid swelling | 15 | 28 | 425
(<135mg/dl normal ) |
| 2. | 20/male | Bilateral dacryoadenitis with mediastinal LAP and hepatosplenomegaly | Bilateral upper eyelid swelling | 14 | 30 | 13 (0.03-2.01) |
| 3. | 30/female | Left dacryoadenitis | Left eye upper lid swelling | 4 | 20 | 2.97( <2.01) |
| 4. | 55/male | Left dacryoadenitis | Left eye upper lid swelling | 11 | 18 | 123(<135mg/dl) |
| 5. | 50/female | Right dacryoadenitis | Right eye upper lid swelling | 19 | 34 | 131(4-86) |
| 6. | 60/male | Left orbital pseudotumour | Left eye proptosis | 8 | 16 | 153.3 (4-86) |
| 7. | 50/male | Right orbital pseudotumour | Right eye proptosis | 5 | 19 | 43.4(4-86) |
| 8. | 60/male | Left orbital pseudotumor+dacryoadenitis | Left eye swelling upper lid+proptosis | 10 | 12 | 4.54( 0.03-2.01) |
| 9. | 68/female | Left orbital pseudotumor+proptosis | Left eye swelling upper lid+proptosis | 5 | 23 | 155(>135mg/dl) |
Table 2: shows radiology and biopsy findings along with final diagnosis
| S.NO. | AGE/SEX | RADIOLOGY | BIOPSY | DIAGNOSIS |
| 1. | 55/F | Bilateral soft tissue swelling in extraconal superotemporal quadrant with enhancement of lacrimal gland area | Fibrosis with IgG4 positive plasma cells
>10perHPF |
Definite IgG4 |
| 2. | 20/M | Bilateral lacrimal gland swelling and mediastinal LAP on CT chest | Lymphoplasmacytic infiltration with 5-8% IgG4 positive cells | Possible IgG4 |
| 3. | 30/F | Left lacrimal gland swelling | Fibrosis with IgG4 positive plasma cells
<10 per HPF |
Possible IgG4 |
| 4. | 55/M | Left lacrimal gland swelling | Fibrosis with IgG4 positive plasma cells
>30 per HPF |
Probable IgG4 |
| 5. | 50/F | Right lacrimal gland swelling | Lymphoplasmacytic infiltration with 30% IgG4 positive cells | Definite IgG4 |
| 6. | 60/M | Left intraconal soft tissue with inferior rectus involvement | Fibrosis with IgG4 positive plasma cells
<10 per HPF |
Possible IgG4 |
| 7. | 50/M | Intraconal+extraconal mass involving medial rectus | Dense fibrosis with IgG4 positive plasma cells and raised eosinophils | probable IgG4 |
| 8. | 60/M | Left orbital soft tissue mass involving lacrimal gland | Fibrocollagenous stroma with lymphoplasmacytic infiltrate 25% positive IgG4 plasma cells. | Definite IgG4 |
| 9. | 68/F | Left orbital soft tissue mass involving lacrimal gland | Fibrosis with few IgG4 positive cells | possible IgG4 |
TABLE 3: Treatment and clinical outcome
| S.NO. | AGE/SEX | TREATMENT | OUTCOME AND FOLLOWUP |
| 1. | 55/F | Steroids and azathioprine | Stable (1year ) |
| 2. | 20/M | Steroids and azathioprine | Stable ( 5months) |
| 3. | 30/F | Steroids and azathioprine | Stable and off steroids since April 2016 |
| 4. | 55/M | Steroids and azathioprine | Stable (2years) |
| 5. | 50/F | Steroids , azathioprine,rituximab
(resistant) |
After rituximab stable
On tapering steroids with azathioprine 25mg/day |
| 6. | 60/M | Steroids, azathioprine for 4 years. On stopping steroids proptosis recurred. On steroids 5mg and azathioprine | Low dose steroids with azathioprine (4
years) |
| 7. | 50/M | Steroids, azathioprine | Steroids tapered off,on azathioprine (3years) |
|
8. |
60/M |
Steroids,azathioprine,rituximab | After rituximab stable
On tapering steroids with azathioprine |
| 9.
|
68/F
|
Steroids,azathioprine | Steroids,azathioprine( reacted to azathioprine, stable on low dose steroids) 1 year |
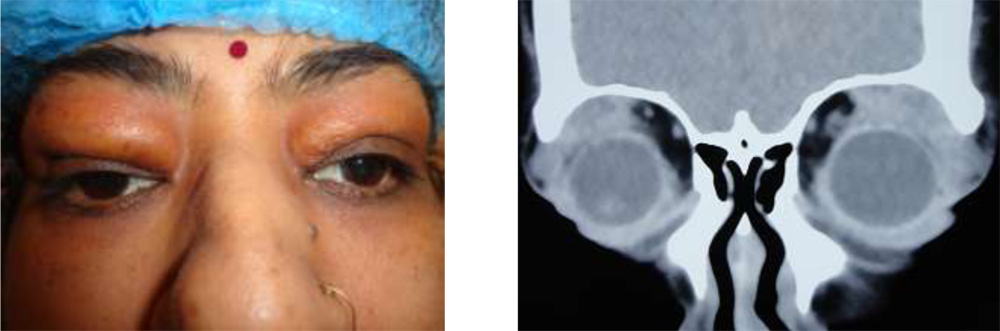 Figure 1: a) 55 year old female presenting with bilateral upper lid swelling (bilateral dacryoadenitis)b) CTscan showing soft tissue swelling in superotemporal quadrants on both sides.
Figure 1: a) 55 year old female presenting with bilateral upper lid swelling (bilateral dacryoadenitis)b) CTscan showing soft tissue swelling in superotemporal quadrants on both sides.
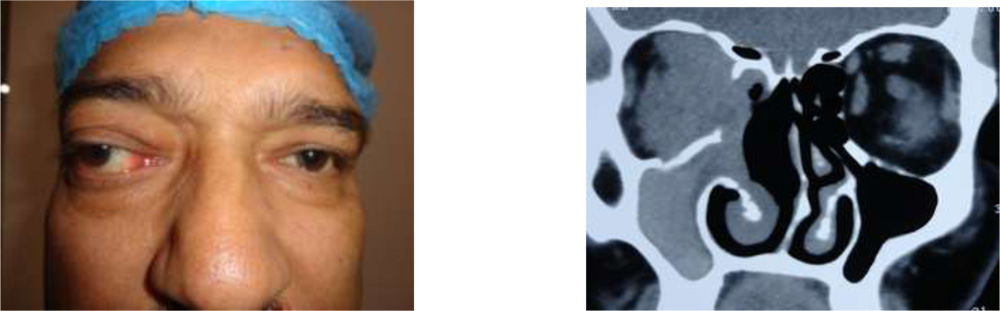 Figure 2: a) 50year old male presenting with right eye non-axial proptosis
Figure 2: a) 50year old male presenting with right eye non-axial proptosis
b) CT scan shows intraconal and extraconal mass involving medial rectus muscle.
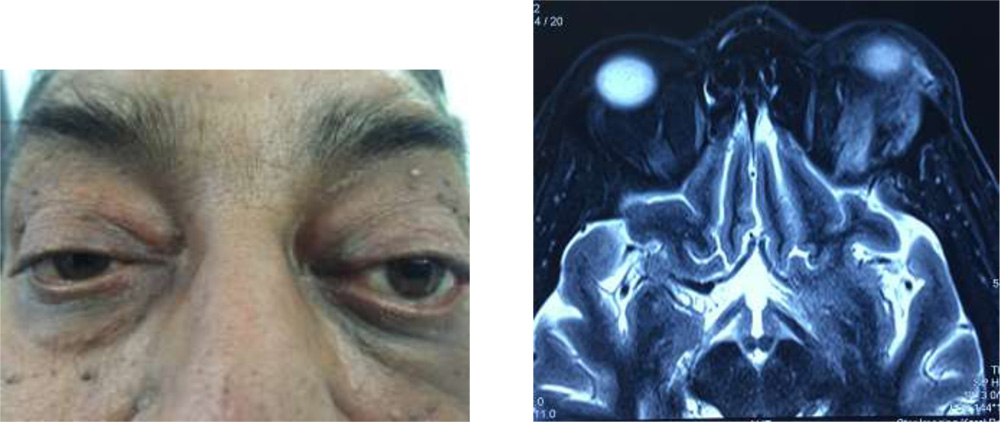
Figure 3: a) 60year old male presenting with left eye proptosis with upper lid swelling
b) MRI shows left orbital soft tissue mass involving lacrimal gland
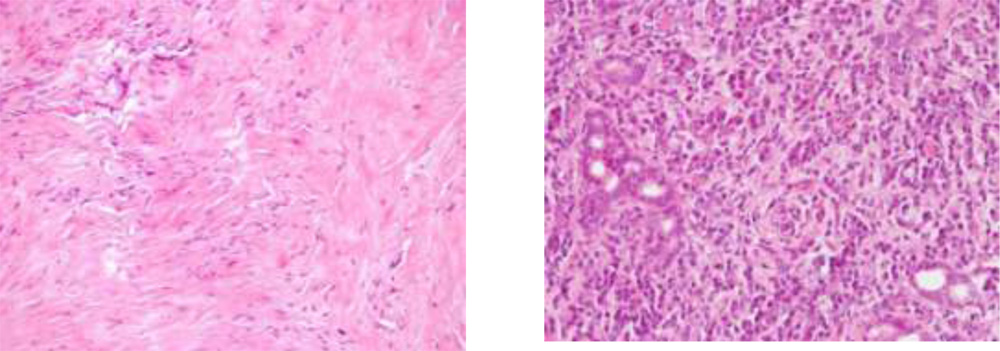
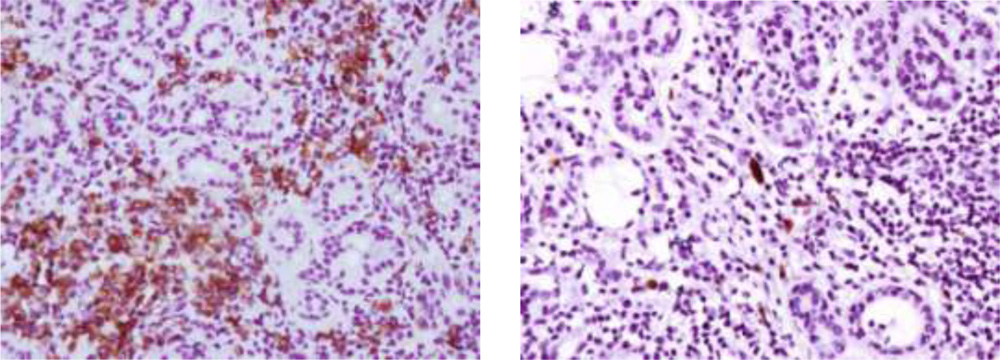
Figure 4: a) H & E staining under 10X showing extensive fibrosis ( storiform pattern)
b) H&E staining under 40X showing plasma cells
c) IHC under 40X showing CD-138 positive plasma cells
d) IHC under 40X showing IgG4 positive plasma cells
Discussion
This study depicts the spectrum of manifestations in orbital IgG4 related disease along with their epidemiological, radiological , laboratory and histological data. Standard treatment for this disease remains oral steroids with immunosuppressants as maintenance therapy. However, in our study 2/9 patients had to be given rituximab due to resistance to steroid therapy and it proved to be beneficial as patients had better clinical outcome.
The diagnosis of IgG4 related disease,often missed earlier, is critical as it has led to targeted therapies with immunosuppressive agents and rituximab with better clinical outcomes.
Rituximab is a monoclonal antibody which acts against CD-20 positive B lymphocytes. These B lymphocytes differentiate into short acting plasma cells that produce IgG4 antibodies. This therapy has shown promising results in inducing clinical remission and is also associated with fall in serum IgG4 levels, especially in resistant and recurrent cases.6,7
We plan to conduct more studies in future with more number of patients to look into the role of rituximab in management of IgG4 related disease.
References
1.Stone JH, Zen Y, Deshpande V. IgG4-related disease. N Engl J Med. 2012; 366:539-551.
2.Hamano H, Kawa S, Horiuchi A ,et al. High serum IgG concentrations in patients with sclerosing pancreatitis. N Engl J Med. 2001;344:732-738.
3.Stone JH. IgG4- related disease:nomenclature,clinical features, and treatment. Semin Diagn Pathol. 2012;29:177-190.
4.Divatia M, Kim SA, Ro JY. IgG4 –related sclerosing disease, an emerging entity: a review of a multi-system disease. Yonsei Med J. 2012;53:15-34.
5. Kubota T, Moritani S, Katayama M, et al. . Ocular adnexal IgG4-related lymphoplasmacytic infiltrative disorder. Arch Ophthalmol. 2010;128:577-584.
6.Khosroshahi A, Bloch DB, Deshpande V,et al.Rituximab therapy leads to rapid decline of serum IgG4 levels and prompt clinical improvement in IgG4 –related systemic disease. Arthritis Rheum 2010;62:1755-62.
7. Wu A, Andrew NH, Tsirbas A, et al. Rituximab for the treatment of IgG4-related orbital disease:experience from five cases. Eye(Lond) 2015;29:122-8.