Dr. Harshal Rathi,
R15159
A rare case of late-onset fluid filled Descemet membrane detachment following cataract surgery and its management.
Harshal Rathi, DNB, FICO; Anitha Venugopal
Aravind Eye Hospital and Post graduate Institute of Ophthalmology, Tirunelveli,
INDIA.
Introduction:
Descemet membrane detachment (DMD) is a known complication after cataract surgery. However it is usually noticed intra-operatively or in the early post-operative period. Late onset DMD after cataract surgery is seldom reported.1-3 Here we report a rare case of late onset spontaneous DMD with fluid filled in the space created by the separation, along with its anterior segment optical coherence tomography (AS-OCT) documentation and treatment.
Case Report:
A 77 years old male patient came with the complaints of white coloured opacity in the left eye noticed since 1 week. He had undergone phacoemulsification surgery in his left eye 19 months back. His best corrected vision was 6/6 in the right eye and 6/9 in the left eye. On slit-lamp examination, an area of localized bullous DMD of about 4 mm in diameter was noted. It was present in the inferior half of the cornea, with the upper limit of the detachment bisecting the pupil (Figure 1). The space between the stroma and the descemet membrane (DM) was filled with whitish turbid fluid. The fluid was more opaque in the inferior three-fourth of the space with relatively transparent fluid filling up the remaining upper part, thus resembling a hypopyon. AS- OCT confirmed the DMD with fluid filled in the space (Figure 2). There were no signs suggestive of inflammation. A posterior chamber intra-ocular lens was present in both the eyes. The rest slit-lamp examination of the right eye was normal. The fundus examination was normal.
His surgery records revealed an uneventful phacoemulsification surgery for a white mature cataract. Striate keratopathy was noted in the immediate post-operative period. AS-OCT showed small DMD at the site of the incision, no DMD was noted elsewhere (Figure 3). The striate keratopathy had resolved completely over a period of 4 weeks with the best corrected vision of 6/6.
As the patient was not willing for an operating theatre based procedure, Nd: YAG (Neodymium doped Yttrium Aluminium Garnet) laser was used to make openings into the DM (Descemetotomy) in an attempt to drain the fluid into the anterior chamber in an attempt to resolve the DMD and improve the vision. The risks and the benefits of the procedure were explained to the patient beforehand. A low energy laser beam (0.8 mJ/ pulse) was focussed on the detached DM above the inferior edge of the DMD. Two openings were made. 2 weeks after the procedure, the fluid was almost completely drained with resolution of DMD (Figure 4) and improvement of vision to 6/6. No inflammation was noted after the procedure. Minimal DM scarring was noted in the DMD area where the laser was applied. AS-OCT revealed (Figure 5) complete resolution of the DMD with slightly irregular DM near the areas where laser was applied.
Discussion:
Late-onset DMD with fluid filled space following cataract surgery has been reported only twice in the literature as per our knowledge.2-3 The clinical features of our patient were similar to these reported cases, with the only exception being absence of fine capillaries near the edges of DMD in our case. The source of the fluid remains unknown. In the reported cases, the aspiration of fluid had revealed necrotic and few viable squamous epithelial cells in one case while other case had calcium oxalate crystals with cellular debris.2,3 The fluid could not be obtained for analysis in our patient due to the non-invasive nature of the procedure.
Nd: YAG laser has been used with success to make openings in the retained DM following penetrating keratoplasty surgeries.4,5 However, there are no reports on application of laser in fluid-filled DMDs. As per our knowledge, this is the first such reported case of fluid-filled DMD treated by draining the fluid into the anterior chamber via openings made in the DM with the help of Nd: YAG laser along with its AS-OCT documentation.
However, the safety of Nd: YAG descemetotomy procedure needs to be evaluated before conclusively advising the procedure to the cases of fluid-filled DMDs
Bibliography:
- Morrison LK, Talley TW, Waltman SR. Spontaneous Detachment of Descemet’s Membrane. Cornea. 1989; 8:303-5.
- Singh D. Localized bullous separation of Descemet’s membrane after previous cataract surgery. J Cataract Refract Surg. 1996; 22:147-9.
- Singh D, Singh M. Bullous separation of the Descemet’s membrane Indian J Ophthalmol. 1978; 25:47
- Steinemann TL, Henry K, Brown MF. Nd: YAG laser treatment of retained Descemet’s membrane after penetrating keratoplasty. Ophthalmic Surg. 1994; 26:80-1.
- Arenas AE, Ramirez CM, Mieth AA. Double Descemet’s membrane in penetrating keratoplasty. Refract Corneal Surg. 1992; 9:65 Figure 1: Slit-lamp photo of the fluid-filled DMD.
Figure 1: Slit-lamp photo of the fluid-filled DMD.
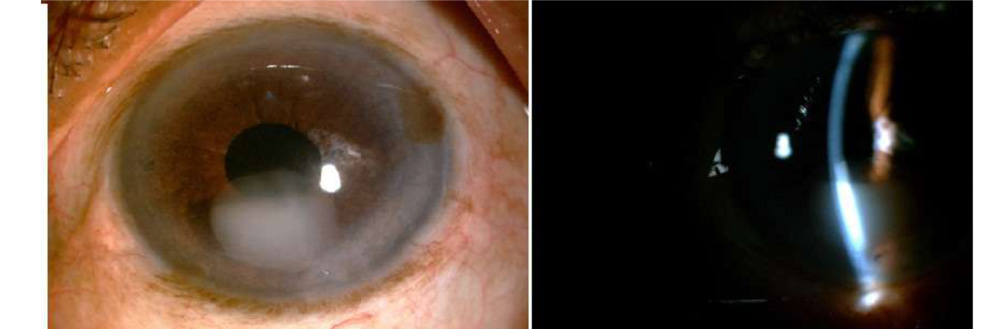
Figure 2: AS-OCT image showing DMD with fluid filled space.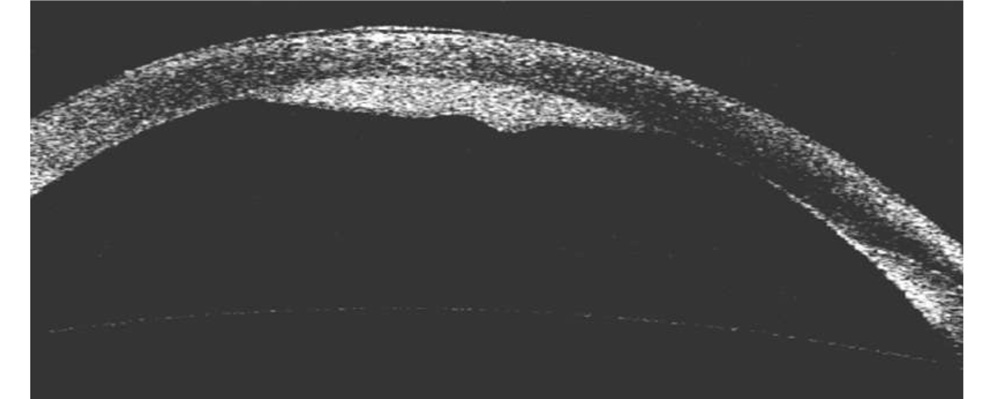
Figure 3: Day 1 post-operative AS-OCT image showing increase in corneal thickness, irregular DM and small DMD at the incision site.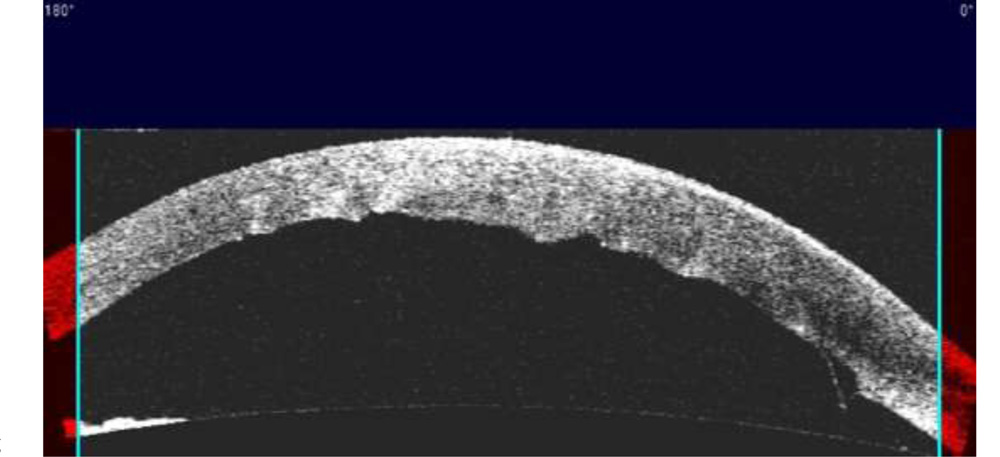 Figure 4: Complete resolution of DMD with minimal DM scarring
Figure 4: Complete resolution of DMD with minimal DM scarring
DM can be seen corresponding to the scarred area (Arrow).
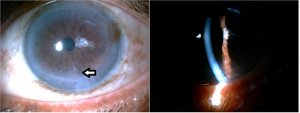 Figure 5: AS-OCT image confirming the resolution of DMD. Irregular
Figure 5: AS-OCT image confirming the resolution of DMD. Irregular
DM can be seen corresponding to the scarred area (Arrow).
