Dr. Gazal Patnaik, P18593, Dr. Sumita Mohapatra, Dr. Nanda Prasanta Kumar, Dr. Rath Indrani Dr. Gazal Patnaik, Dr. Sumita Mohapatra, Dr. P.K. Nanda, Dr. I. Rath
Making an early diagnosis of AS was difficult, because
disease onset is insidious and sacroiliitis is not evident on plain X-ray until the disease is at an advanced stage. The major functional losses occur during the first 10 years of disease.
Since a prolonged delay in diagnosis is common
among SpA patients, and occurrence of uveitis may be the reason for their first interaction with medical care, a novel evidence-based algorithm, named DUET, has been proposed to guide ophthalmologists to refer appropriate IAU patients to rheumatologists
Ocular inflammation is common in many rheumatologic diseases but with variable prevalence.
This review limits itself to the idiopathic anterior uveitis (IAU) seen in association with inflammatory rheumatic diseases grouped under the term spondyloarthropathies or spondyloarthritis (SpA) that encompasses ankylosing spondylitis (AS),psoriatic arthritis (PsA), reactive arthritis(ReA) and undifferentiated SpAUnraveling the mystery of their association could help us better understand the pathoetiology of SpA.
MATERIALS AND METHODS
A Prospective study was conducted in Regional Institute of Ophthalmology,S. C. B. Medical College and Hospital, Odisha over a period of 6 months from November 2015 to December 2016 with due clearance from instituitional ethical committee.
INCLUSION CRITERIA-
All patients with Idiopathic Anterior Uveitis
EXCLUSION CRITERIA-
All diagnosed cases of any form of spondyloarthropathy
Anterior uveitis due to any other apparent cause
(like traumatic uveitis,post operative uveitis ) Other forms of uveitis(intermediate, posterior or pan uveitis)
108 patients of idiopathic anterior uveitis were thoroughly examined including slit lamp biomicroscopy. Then further investigation were carried out in consonance with a novel algorithm,DUET algorithm.
STATISTICAL ANALYSIS-SPSS Software was used for all the stastistical analysis of the data obtained and interpreted in the form of tables,graphs and charts.
RESULTS :
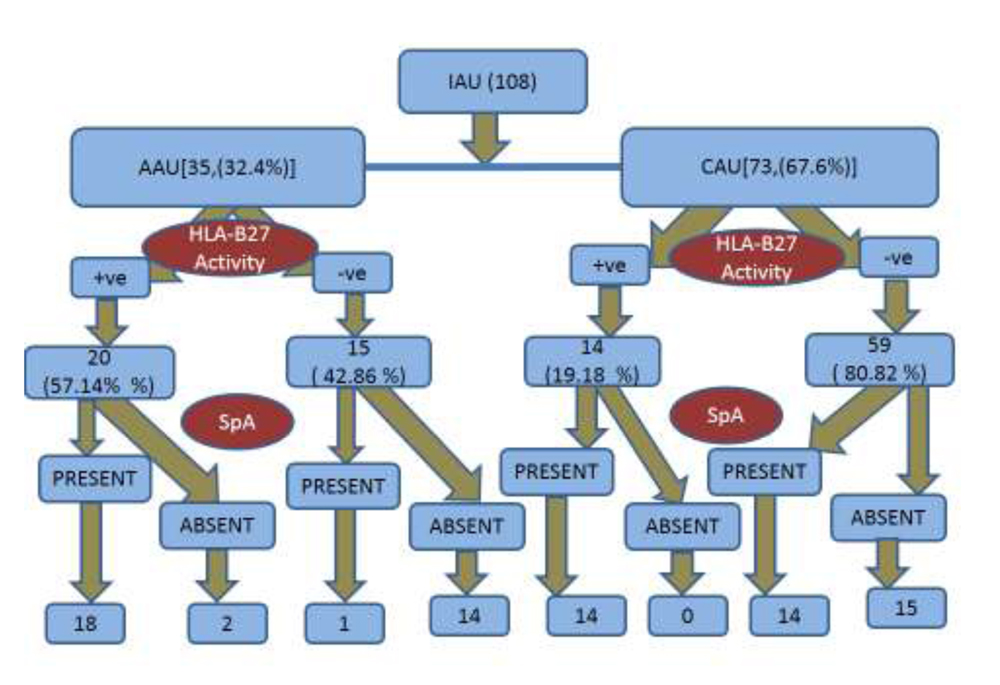
Amongst 108 patients of IAU, 35(32.40%) were found to have acute anterior uveitis(AAU) & 73(67.60%) had Chronic anterior uveitis(CAU). M:F with AAU was 1.7:1 and with CAU was 0.78:1. 47pts(43.52%) of whom had some form of SpA.(19 had AAU & 28 had CAU)
34 pts (72.34%) of those undiagnosed SpA were found to be HLA-B27 positive, of whom 20(58.82%) had AAU & 14(41.18%) had CAU.
Out of 19 AAU pts with undiagnosed SpA , 12 had Ankylosing Spondylitis(AS), 3 had Reactive A. (ReA), 2 had Psoariatic A. (PsA) & rest 2 had other form of SpA.
Out of 28 CAU pts with undiagnosed SpA, 17 had AS, 3 had ReA, 5 had PsA, 3 had other form of SpA.
DISCUSSION-
The association between the presence of HLAB27+
Tissue type, ankylosing spondylitis (AS), and acute anterior uveitis (AAU) was first described in 1973.

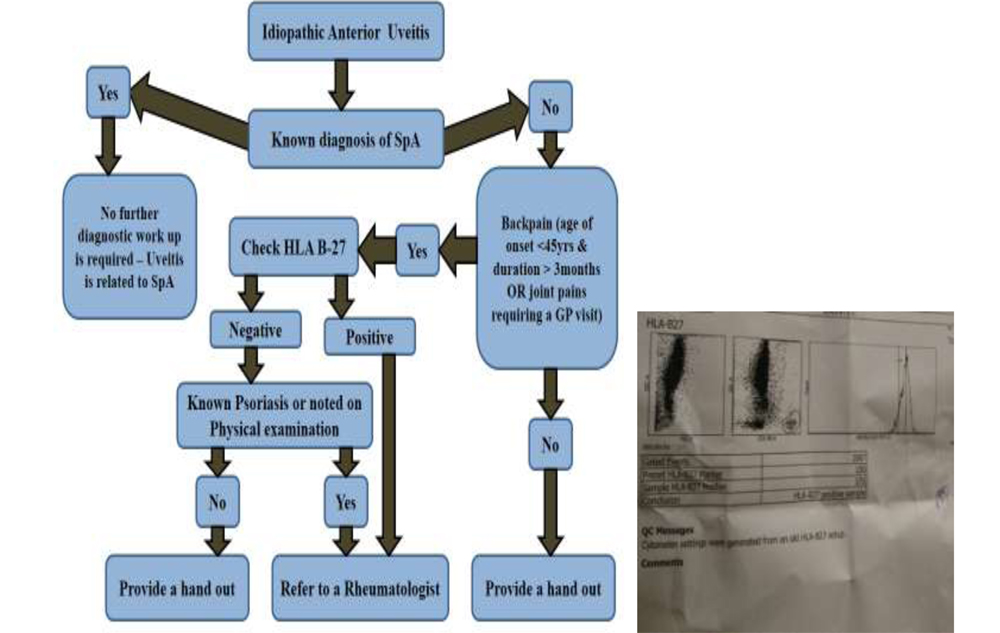
Dublin Uveitis Evaluation Tool (DUET)
| Spa | Mean | Std. Deviation | P-value | |
| AGE | Present (47) | 51.5 | 7.9533 | 0.029 |
| Absent (61) | 55.1 | 6.4454 |
Mean age of presentation with respect to presence of undiagnosed SpA
| Variety of IAU | Mean | Std. Deviation | P-value | |
| AGE | AAU (35) | 49.486 | 6.31698 | 0.528 |
| CAU (73) | 55.466 | 7.01008 |
Mean age of presentation in different varieties of IAU
| Sex | Mean | Std. Deviation | P-value | |
| AGE | Male (22) | 47.6364 | 5.96454 | 0.98 |
| Female (13) | 52.6154 | 5.82435 |
Mean age of both the sexes with AAU having hidden SpA
| Sex | Mean | Std. Deviation | P-value | |
| AGE | Male (32) | 54.0938 | 7.81793 | 0.016 |
| Female (41) | 56.5366 | 6.19717 |
Mean age of both the sexes with CAU having hidden SpA
| as | Total | ||||
| positive | negative | ||||
| hlab27 | positive | Count | 11 | 3 | 14 |
| % within hlab27 | 78.6% | 21.4% | 100.0% | ||
| negative | Count | 4 | 55 | 59 | |
| % within hlab27 | 6.8% | 93.2% | 100.0% | ||
| Total | Count | 15 | 58 | 73 | |
| % within hlab27 | 20.5% | 79.5% | 100.0% | ||
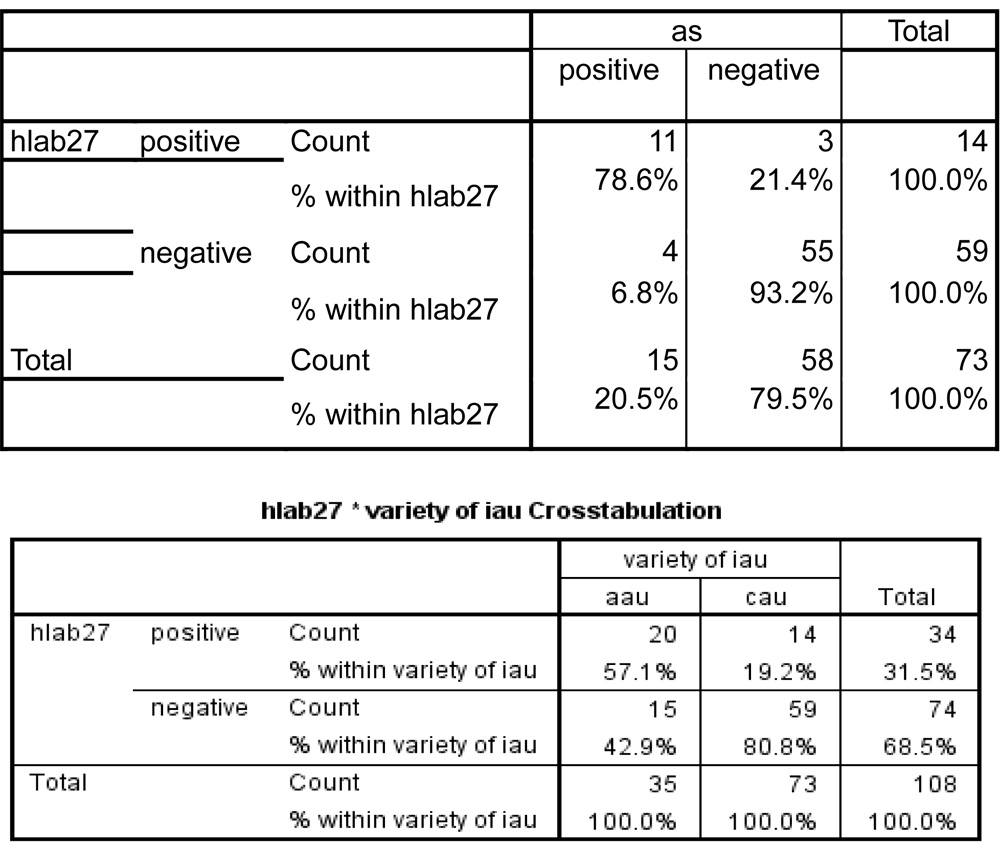
Approximately half of the acute anterior uveítis cases are associated with the presence of the HLA-B27 antigen.
It can bethe first manifestation of an undiagnosed rheumatic disease, usually having a good prognosis and appropriate response totreatment.
Beckingsale et al.
have reported an appreciable incidence of asymptomatic AS in AAU. On the other hand patients with psoriasis-associated AS are not uncommonly asymptomatic.
Brewerton et al.,
who give a value of 43% HLA-B27+ in AAU.’ Others’ have shown nearer 60% of their uveitis patients to have HLA-B27+ tissue type.
CONCLUSION-
In our study ,we found 43.52% of IAU patients to have undiagnosed SpA of which 61.70% had AS(63.18% of AAU & 60.71% of CAU).More complicated forms & recurrence of IAU were found in those with HLA-B27 positivity.
In conclusion, for better assessment and treatment of patients with uveitis, ophthalmologists and rheumatologists should work together.
REFERENCES-
- Rosenbaum JT. Uveitis in spondyloarthritis including psoriatic arthritis, ankylosing spondylitis, and inflammatory bowel disease. Clin Rheumatol. 2015; 34(6):999–1002. An up-to-date review article discussing the clinical features of uveitis associated with different forms of spondyoarthritis
- Smith WM. Gender and spondyloarthropathy-associated uveitis. J Ophthalmol. 2013;2013:928264. This is an interesting article describing the differential association of gender and uveitis among patients with Ankylosing Spondylitis and inflammatory bowel disease
- Wendling D, Prati C, Demattei C, Miceli C, Daures JP, Dougados M. Impact of uveitis on the phenotype of patients with recent inflammatory back pain. Data from the DESIR cohort. Arthritis Care Res (Hoboken). 2012. doi:10.1002/acr. 21648. First data about uveitis in this prospective cohort of potential early spondyloarthritis; uveitis was associated in this population with recent infectious episode and inflammatory bowel disease.
- Rosembaum JT. Acute uveitis and spondyloarthropathies. Rheum Dis Clin North Am 1992; 18(1):143–52
- Sampaio-Barros PD. Epidemiology of spondyloarthritis in Brazil. Am J Med Sci 2011; 341(4):287–8
- Jimenez-Balderas FJ, Mintz G. Ankylosing spondylitis: clinical course in women and men. J Rheumatol 1993; 20(12):2069–72.
- McBryde AM, McCollum DE. Ankylosing spondylitis in women. The disease and its prognosis. N C Med J 1973; 34(1):34–71..
- Laval SH, Timms A, Edwards S, Bradbury L, Brophy S, Milicic A. Whole-genome screening in ankylosing spondylitis: evidence of non-MHC genetic-susceptibility loci. Am J Hum Genet 2001; 68(4):918–26
- Gran JT, Husby G. The epidemiology of ankylosing spondylitis. Semin Arthritis Rheum 1993; 22(5):319–34.
- Brewerton DA, Hart FD, Nicholis, Caffrey M, James DC. Ankylosing spondilitis and HLA-27. Lancet 1973; 1(7809):904–7.
- Carvalho MA, Campos WR, Araújo CA, Lacerda RR, Oréfi ce F. Uveítes anteriores não granulomatosas, espondiloartritese HLA-B27. Rev Bras Reumatol 1999; 39:195–202
- McCannel CA, Holland GN, Helm CJ, Cornell PJ, Winston JV, Rimmer TG. Causes of uveitis in the general practice of ophthalmology. Am J Ophthalmol 1996; 121(1):35–46
- Trevisani VF, Mattos KT, Esteves RF, Olialves SM, Andrade LE. Autoantibodies specificity in acute anterior uveitis according to the presence of the HLA-B27 allele. Ocul Immunol Inflamm 2001; 9(4):231–42.
- Beckingsale AB, Guss RB, Rosenthal AR. Acute anterior uveitis associated with HLA B27 positive tissue type: a comparative study in two populations. T’rans Ophthalmol Soc UK 1982; 102: 168-70.
- Jacic 1. Radiological changes in the sacro-iliac joints and spine of patients with psoriatic arthritis and psoriasis. Ann Rheum Dis 1968; 27: 1-6.
- Molin L. Psoriasis. Acta Derm Venereol (Stockh) 1973; 53 (suppl 72): 7-125.
- Brewerton DA, Caffrey M, Nicholls A, Walters D, James DCO. Acute anterior uveitis and HLA 27. Lancet 1974; i: 464.
- Brewerton DA. HLA 27 and acute anterior uveitis. Ann Rheum Dis 1975; 34 (suppl): 33-5.
- Brewerton DA, Caffrey M, Hart FD, James DCO, Nicholls A, Sturrock RD. Ankylosing spondylitis and HL-A27. Lancet 1973; i: 904-7.
- Brewerton DA, Caffrey M, Nicholls A, Walters D, James DCO. Acute anterior uveitis and HL-A27. Lancet 1973; ii: 994-6.