Dr. Seema Bhosale, Dr. Sudha
Setharam, Dr. Vijay Shetty, Dr. Suhas Haldipurkar
FINANCIAL DISCLOSURE- None of the authors have any financial or proprietary interest in any products mentioned in this study
Introduction –
Keratoconus is an ocular condition characterized by the progressive non-inflammatory thinning and protrusion of the cornea, accompanied by the decentration of the resulting cone, corneal distortion, increased irregular astigmatism and myopia1 . The most frequent location of this corneal focal curvature is the mid-periphery region, both in the inferior-nasal and inferior-temporal quadrants, wherein, the paracentral region comprises about 72 % of cases, and approximately 25 % of those cases are included in the central region.2,3
Elevation based Scheimpflug imaging is used for the diagnostic characterization of the front and back corneal surface, along with the pachymetric mapping4. The Tangential maps are considered highly sensitive in detecting sudden changes in the corneal curvature as compared to Sagittal maps5,6
Purpose –
To evaluate the change in magnitude at different predetermined locations on the anterior and posterior location, on the Sagittal and Tangential map in patients of different grades of keratoconus.
Aim of the study – To evaluate the change in magnitude at different predetermined locations at 3mm, 5mm and7mm, on the anterior and posterior location, on the Sagittal and Tangential map in patients of different grades of keratoconus. To evaluate for any correlation in the change in the magnitude between the anterior and posterior surface and for Sagittal and Tangential maps.
Materials and Methods – A Secondary data analyses done at a Tertiary eye institute in Western Maharashtra conducted between February 2012 – April 2016 including 80 eyes of 42 patients of Keratoconus, 30 eyes of 15 normals. All Patients diagnosed of Keratoconus in the study period were included. Patients of Keratoconus who had undergone treatment elsewhere and patients who had any other additional corneal pathology were excluded. All patients underwent ophthalmic examination (Keratometry, Manifest Refraction, Slit lamp biomicroscopy) and Pentacam measurements of the first visit. The patients were divided into grades according to Amsler-Krumeich classification (Grade1-29, Grade 2- 27, Grade 3-7, Grade 4- 17). The magnitude of curvature on the anterior and posterior corneal surface was noted at 30, 90, 150, 210, 270, 330 orientation on the sagittal and tangential maps at 3mm, 5mm and 7mm on the pentacam. The means of the superior (30,90,150) and inferior (210,270,330) magnitudes were assessed for all grades of Keratoconus. The Data was analyzed using STATA version 13.
Discussion –
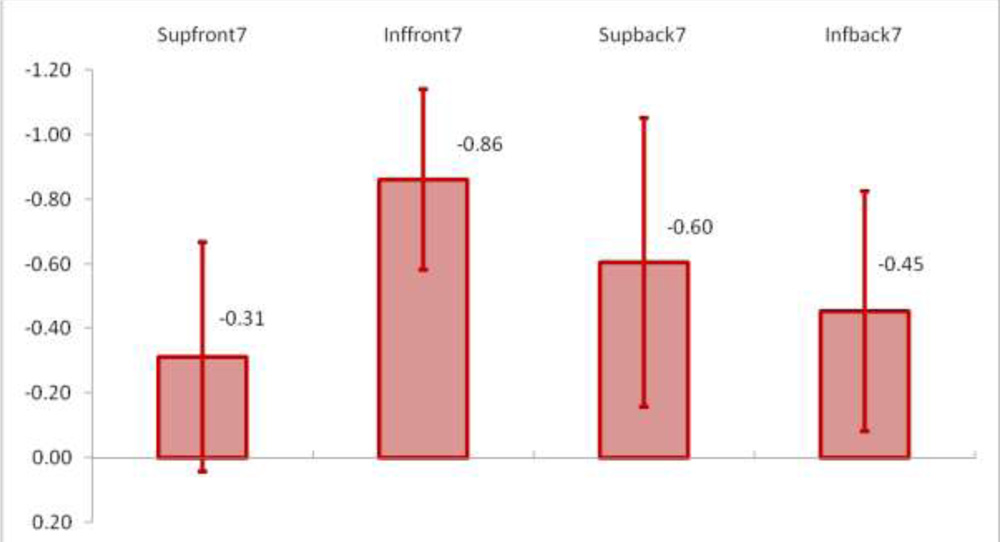
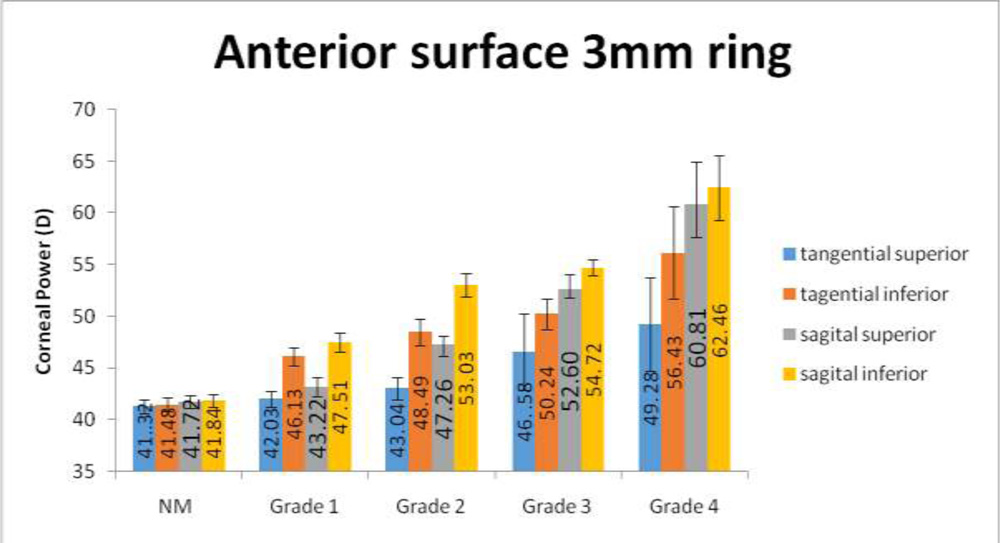
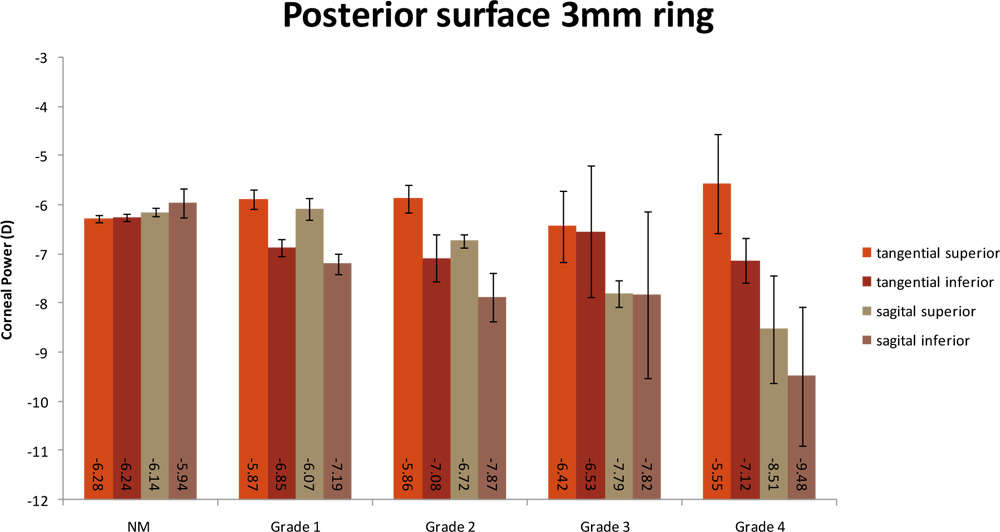
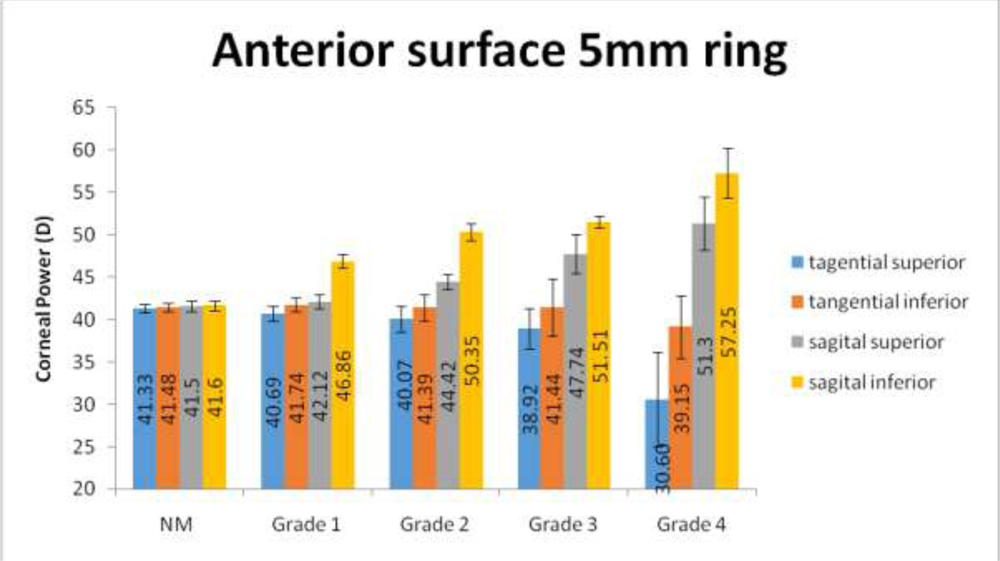
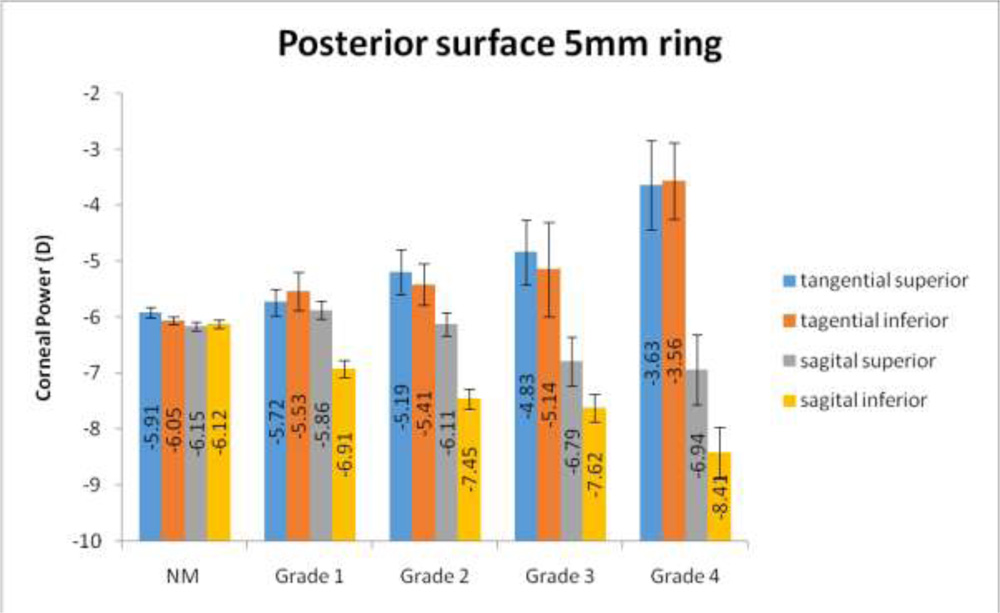
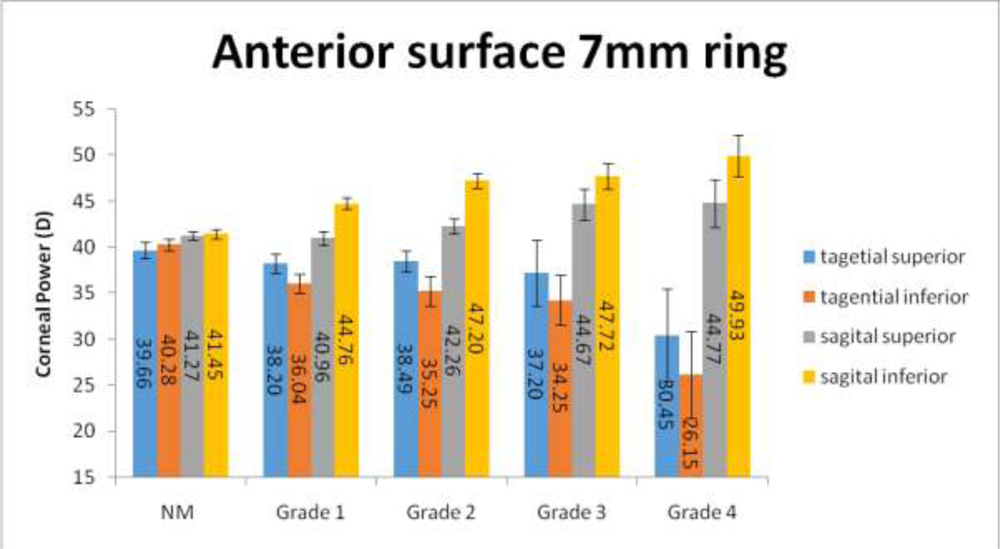
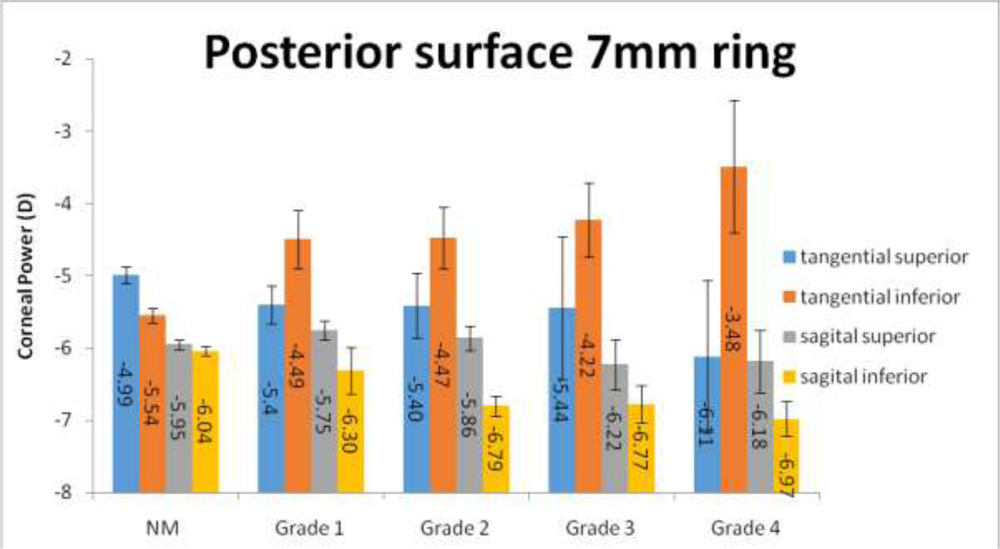
The mean magnitudes at the superior and inferior locations at 3mm,5mm and 7 mm showed an increasing trend for all grades on anterior and posterior surface on the sagittal maps. The same trend was noted for both the superior and inferior surface on the tangential map at 3mm, for superior surface at 5mm but this was not noted on the posterior surface at 5mm and for both surfaces at 7mm on the tangential map. A unit change in the magnitude on the Sagittal map showed a statistically significant positive change with the Tangential map at 3mm and a negative change at 7mm. Tummanpalli et al. noted a steeper tangential apex curvature as compared to the axial curvature in detecting subclinical Keratoconus7. A small sample size and retrospective study are limitations of the study.
Conclusion –
The magnitudes at the inferior locations at 3mm and 5mm were higher than that noted superiorly, comparable to the higher occurrence of paracentral cones in all grades of Keratoconus. The sagittal map showed better correlation as compared to the tangential maps.
References –
1)Rabinowitz YS. Keratoconus. Surv Ophthalmol. 1998;42:297–319
2) Wilson SE, Lin DT, Klyce SD. Corneal topography of keratoconus. Cornea. 1991;10(1):2–8.
3) Prisant O, Legeais JM, Renard G. Superior keratoconus. Cornea.1997;16(6): 693–4.
4) Ucakhan OO, Cetinkor V, Ozkan M, Kanpolat A. Evaluation of Scheimpflug imaging parameters in subclinical keratoconus, keratoconus, and normal eyes. J Cataract Refract Surg. 2011;37(6):1116–1124
5) Rabinowitz YS. Tangential vs Sagittal videokeratographs in the early detection of keratoconus. Am J Ophthalmol.1996; 122:887-889.
6) Chan JS, Mandell RB, Burger DS, Fusaro RE. Accuracy of videokeratography for instantaneous radius in keratoconus.Optom Vis Sci.1995;72:793–799
7) Efficacy of axial and tangential corneal topography maps in detecting subclinical Keratoconus. J Catarct Refract Surg.2015;41:2205-2214
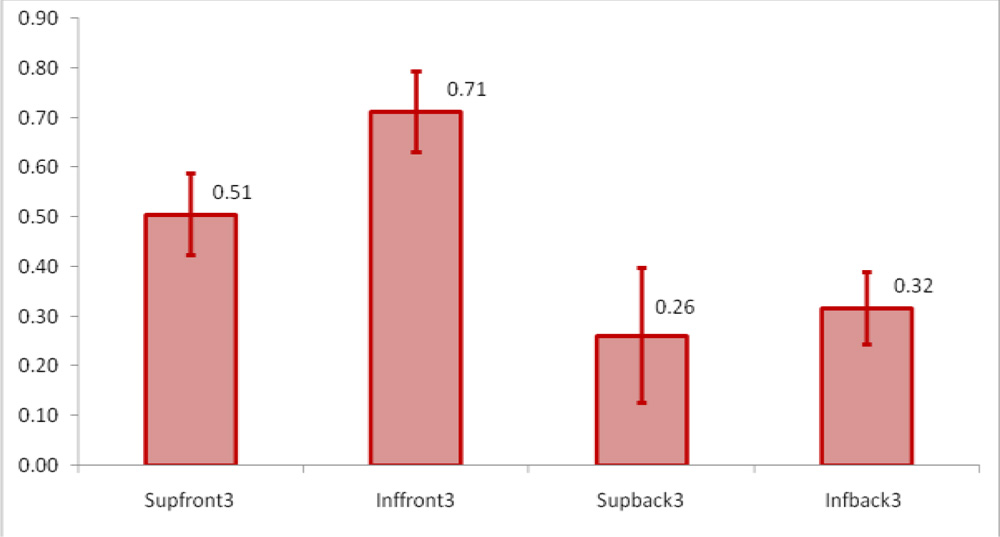
Regression values for unit change -Sagittal and Tangential maps at 3mm
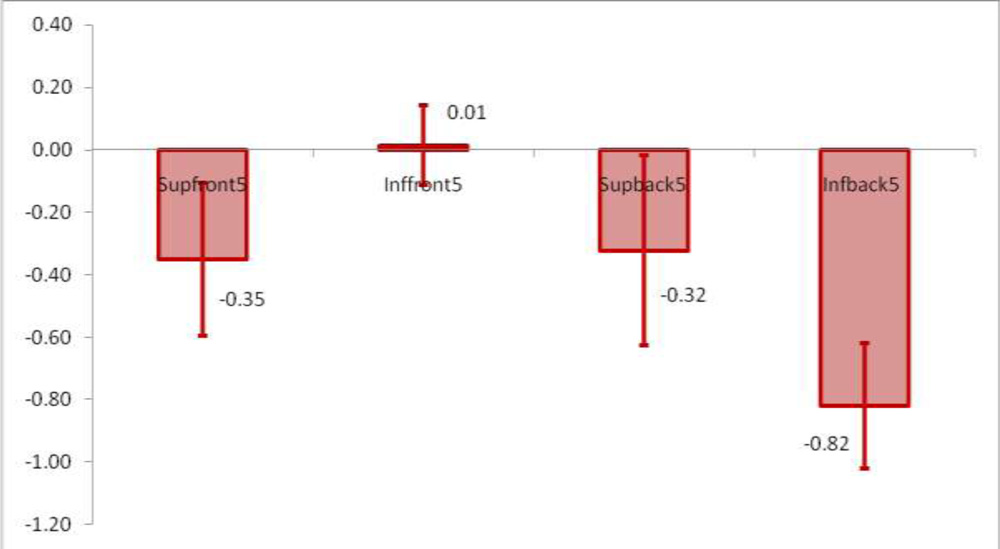
Regression values for unit change- Sagittal and Tangential maps at 5mm
Regression values for unit change- Sagittal and Tangential maps at 7mm