Dr. Tanya
Jain, Dr. Alok Sen, Dr. Shubhi Tripathi
Dr. Tanya Jain
1st year DNB Resident
SadguruNetraChikitsalaya
Jankikund, Chitrakoot
AIOS Registration No.: T19190
Co-Authors- Dr. AlokSen, Dr. ShubhiTripathi
Introduction
The term coloboma is derived from the Greek termkoloboma, meaning mutilated or curtailed. The malformation refers to a notch, gap, hole or fissure in any of the ocular structures. (1)
Colobomata(plural)results from a failure of the fetal or choroidal fissure to close during the 5th to 7th week of fetal life, at the 7-14 mm stage. This is the period between the invagination of the optic vesicle and the closure of the fetal fissure. Almost any ocular structure may be involved, including the cornea, iris, ciliary body, lens, choroid, retina, optic disc and/or optic nerve. (1)
Typical coloboma is involves the infero-nasal quadrant, caused by defective closure of the fetal fissure. It is more frequent and may affect any part of the globe traversed by the fissure from the iris to the optical nerve. (1)
Certain conditions have been implicated to be associated with coloboma like micropthalmia, strabismus, nystagmus, some more than the others. Microcorneafor example is so commonly associated with coloboma that in a study conducted in UK the incidence of microcornea was 0.22 per 1000 and coloboma was 0.26 per 1000. Along with these patients might also develop complications like retinal detachment, giant retinal tears, cataracts, lens subluxation, amblyopia, sensory strabismus, anisometropia and secondary glaucoma. Eyelid colobomata may be associated with exposure keratopathyand even corneal ulcers. Most common among these are idiopathic retinal detachment and cataracts. (1)
A variety of cataracts have been known to be associated with coloboma, including isolated pigment clumping on the lens capsule at the equator, sub-capsular and cortical opacification, anterior and posterior polar cataracts and total opacification(1). Various studies have concluded that cataracts in coloboma present at an earlier age than senile cataracts. (1,3) Also a cataract surgery in colobamtous eyes could be challenging given the abnormal development of the sclera, uvea and the zonules as the structural integrity of the globe is compromised(8). This is also associated with poor pupillary dilatation(7).There factors lead to an increased risk of a posterior capsular rupture, poor visualization leading to capsulorhexis related complications and increased vitreous loss during surgery.
Initially, studies were conducted in order to compare the various methods of cataract surgery and finding which type of cataract surgery would be the most suitable for patients with coloboma. It was concluded that phacoemulsification is the safest and most suitable surgical procedure with least complications. Outcomes of phacoemulsification have also been studied. But retrospective nature, paucity of sample size and inadequate follow-up have remained a constraint. The outcomes of phacoemulsification in different types of coloboma have not been studied. The pre-operative difficulties like axial length and hence the IOL power calculation still remains a challenge. Hence, this study determines the visual outcomes of phacoemulsification in a considerable number of patients along with description of the associated anomalies, pre-operative assessment including type and extent of coloboma and intra-operative and post-operative complications.
Materials and methods
We conducted a Retrospective, Observational and Non-ComparativeStudyof51 eyes with congenital coloboma with cataract who had cataract surgery by Phacoemulsification, presenting to the Outpatient department and retina clinic of a tertiary eye care center in central India, SadguruNetraChikitsalaya, Jankikund, Chitrakoot between march 2014 and march 2016. Inclusion criteria included a diagnosis of coloboma and cataract, cataract surgery by the phacoemulsification technique, and minimum follow-up of 6 weeks.
Case report files of patients were reviewed for age, gender, preoperative and postoperative bestcorrected visual acuity (BCVA) (Snellen converted to LogMAR for analysis), anterior segment bio-microscopy, extent of disease, Non contact tonometry, nuclear sclerosis grade (LOCS 3), type of cataract, presence of other ocular co-morbities and coloboma grading (Ida Mann Classification) . Preoperative assessment including axial length and IOL power were also noted in order to document refractive surprises. Also, type of anaesthesia, incision, type of IOL,post-operative visual acuity (Snellen converted to Log MAR for analysis) intraoperative and postoperative complications were noted. On the follow-up visit at 6 weeks visual acuity and refraction were noted along with any other complication. The 6 week postoperative criterion was selected as this is a reasonable time to expect resolution of postoperative inflammation and healing.
The statistical correlation between pre-operative and 6-week postoperative visual acuity was established using a Wilcoxon signed rank test.
Results
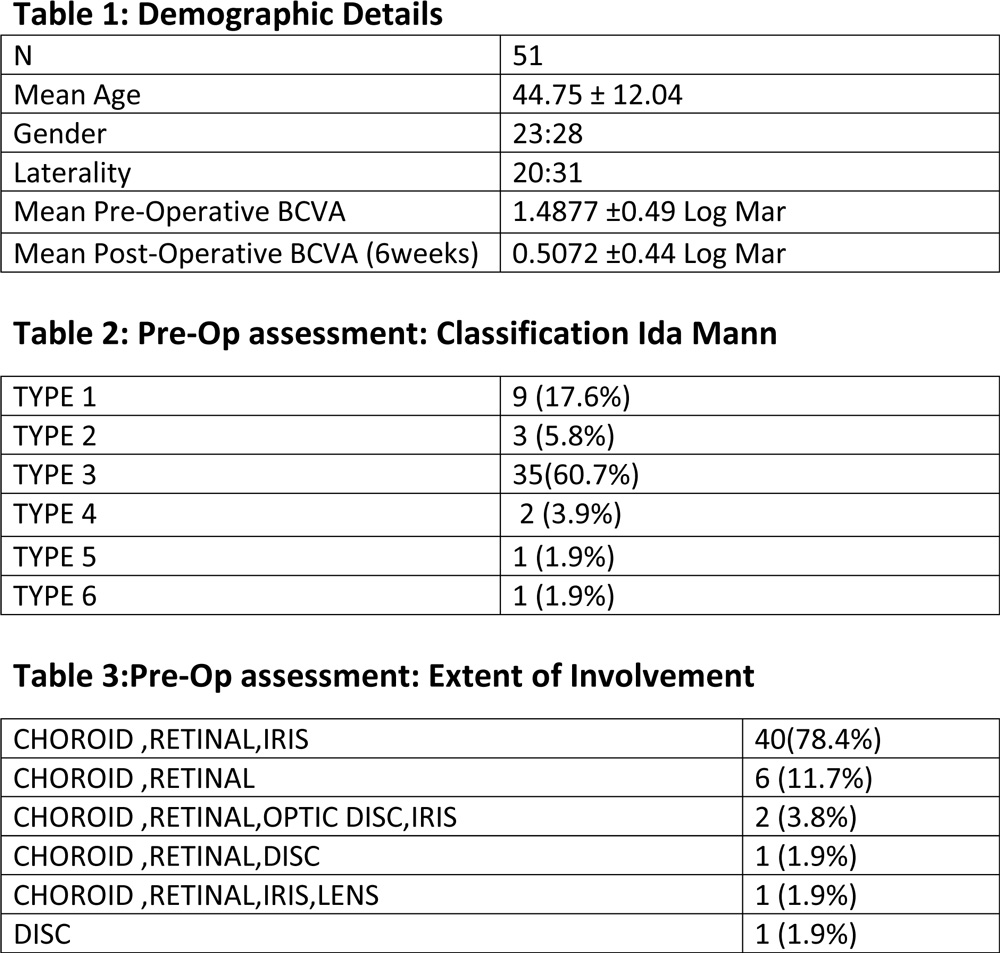
On retrospective case reports evaluation 51 eyes were identified with congenital coloboma and cataracts that underwent cataract extraction by phacoemulsification. Mean age at time of surgery was 44.75 years with 12.104(SD). The male : female ratio was 23:28. 20 eyes had a bilateral coloboma while the rest 31 eyes had a unilateral presentation. The mean visual acuity at the time of presentation was 1.4877 (SD =.49320) Log MAR values. 9 eyes had a type 1 coloboma, 6 eye had a type 2 coloboma, 35 eyes had a type 3 coloboma ;the most common type, 2 eyes had a type 4 coloboma and 1 patient each had type 5 and type 6 coloboma. 40 eyes presented with coloboma of the choroid , retina and the iris, 6 eyes had chorio-retinal coloboma, 2 eyes had coloboma of the iris, optic disc, choroid and retina while 1 eye had coloboma of the iris, lens, choroid and retina. Also, 1 patient had only optic disc coloboma.
Associated ocular anomalies included microcornea in 35 eyes, esotropia in 10 eyes, nystagmus in 6 eyes and posterior staphyloma in 3 eyes.Cataract grading have been shown in table 5.
On pre-operative assessment for IOL power calculation the standard immersion technique was used and the mean axial length was 24.13mm and the mean IOL power was 17.40D. 6 eyes had an axial length more than 25mm.
For the surgery peribulbar anaesthesia was given to all patients. A temporal clear corneal incision was made. Iris hooks were used in 2 eyes with inadequate mydriasis. Intraoperative complications included a zonular dialysis in 10 eyes,a posterior capsular rupture in 4 eyes and vitreous prolapse in 2 eyes.
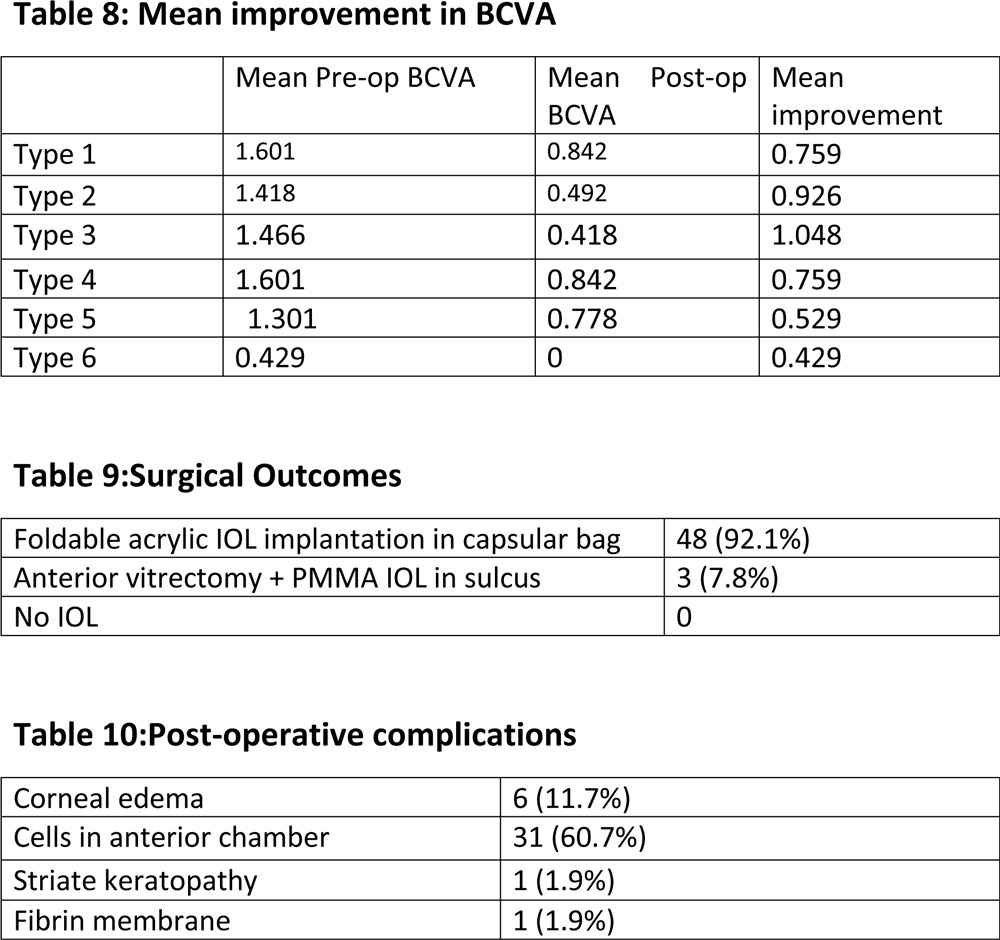
Post operative visual acuity improved to 0.5072(SD =0.44536) Log MAR values.The visual acuity improved in 48 eyes while remained the same in 3 eyes.The mean visual acuity improvement in different types of coloboma have been shown in table 4. Maximum improvement was seen in Post-operative complications includedcorneal oedema in 6 eyes, anterior chamber cells >or= 2+ in 31 eyes, fibrin membrane and striate keratopathy in 1 eye each. No significant complaints were reported 6 weeks post-operatively.
Discussion
The prevalence of congenital coloboma is estimated to be 4.89 per 100 000 newborns(1). Given the infrequent occurrence of this disease the data on the surgical outcomes of coloboma with cataract is limited.
In most reported cases, the cataract surgeries were delayed, and the age at the time of surgery tended to be younger than in eyes with typical visually significant age-related cataract. (2,3,9) In our study also the age at presentation was younger than in eyes with typical visually significant age related cataract. Type 3 was found to be the most common type of coloboma according to the Ida-Mann classification.
Pre-operative assessment has two important considerations. First is the assessment of associated anomalies; mainly microcornea. There is a clear association between microcornea and coloboma with several genetic and multi-system syndromes.(4,9)
Chromosomal and genetic disorders associated with severe microphthalmia with coloboma include trisomy 13; cat-eye, Wolf-Hirschhorn, Lenz’s microphthalmia, Meckel-Gruber, Warburg’s, and Aicardi’s syndromes; and Goltz’sfocal dermal hypoplasia (9). Even though these conditions will present in pediatric age group , a look out for these conditions must be kept in mind.
Another important aspect would be the IOL power calculation in patients with coloboma. The problems in eyes with coloboma are multiple . These include those affecting axial length calculation like coloboma involving the macula, poor fixation, nystagmus and posterior staphyloma and those involving the keratometry like poor fixation and microcornea; thus leading to erroneous IOL power calculation and post-operative refractive surprises. In our study, we found that mean axial length was 24.13mm which was on the higher side and 6 patients had an axial length exceeding 25mm . 3 of these eyeshad a posterior staphyloma which is well known to be associated with coloboma. The axial length of the eyes with posterior staphyloma was calculated using the USG B scan while the conventional immersion technique was used to calculate for the rest of the patients. We found a refractive surprise of more than 3 D in 6 eyes. This shows that IOL power calculation is troublesome in patients with coloboma and refractive surprises need to be looked out for.
Chaurasia et al. compared the outcomes of different types of cataract surgeries in 25 patients of coloboma with cataract. They performed phacoemulsification in 16 eyes with soft to moderate-density cataracts while the others underwent SICS, ECCE or ICCE. 6 out of 25 patients had a posterior capsular rent.Hence,theyconcluded better outcomes with phacoemulsification (10).Norlund et al studiedphacoemulsification in 7 colobomatous eyes with cataract and concluded that even though coloboma can present with pre-operative and technical difficulties but visual acuity improved in all cases. In all cases IOL was implanted and hence they confirmed phacoemulsification to be a safe method to remove cataract in eyes with coloboma and cataract.(2)But the pilot study done by Norlund at al had a small sample size,hence required more scientific evidence.Norlund et al also reported one case with monocular diplopia caused by the edge of optic bisecting the ectopic pupil. Proper centration overcomes this.
Kumar et al studied the outcomes of phacoemulsification in 21 eyes of coloboma with cataract and reported favorable surgical outcomes with phacoemulsification in all densities of cataract with the help of adjuncts like dispersive OVD to protect endothelium and prevent anterior vitreous luxation, sphincterotomy, iris hooks, capsular retractors, Utrata’s forceps, CTR and techniques like stop, chop and stuff for phacoemulsification and bimanual irrigation and aspiration. They did not observe any diplopia or glare.(3)
We after having studied the outcomes of 51 eyes of coloboma with cataract report an improvement in visual acuity in 48 out of 51 eyes(94.1%) while remained unchanged in 3 eyes. 2 out of these4 eyes had optic disc coloboma with foveal involvement (5). 1 was type 4 coloboma. Foveal involvement was also the reason for poor visual outcome in the study conducted by kumar et al.
The mean pre-operative BCVA was 1.487 (SD=.493) which improved to a Mean Post Operative BCVA of 0.507 (SD=0.445) after 6 weeks. This was found to be statistically significant using the Wilcoxon Signed Rank Test with Z value -6.032.The maximum mean improvement was seen in eyes with type 3 coloboma showing the best visual outcome.
An Intraoperative Capsular tension implantation in 19.7% patients clearly indicated weak zonular support and hard cataracts in eyes with coloboma. This was about 40% in a study conducted by kumar et al and 29% in the study by Norlund et al further confirming the weak zonularsupport.Poor pupillary dilatation was also observed in 10 eyes and iris hooks were used in 3.8% of the eyes. Kumar et al reported iris hooks usage in 20% of the eyes. Hence this also is a major intraoperative concern in coloboma patients. Postoperative period was uneventful with no major complications.
Therefore, we report favorable surgical outcomes with phacoemulsification in eyes with coloboma and cataract in all densities of cataract and improved visual acuity in all eyes except those involving the macula. We alsoobserved maximum visual improvement in eyes with type 3 coloboma; the latter being the most common type in our study. There were raised incidence of post capsular rupture and capsular tension ring implantation but IOL placement was nonetheless possible in all cases. We also describe the common associations, extent of coloboma, intra and post operative complications associated with coloboma. We recommend careful evaluation of microcorneaalong with cautious IOL power calculation in these patients as we observed a high incidence of refractive surprises of more than 3D.
Hence, phacoemulsification seems to be a favorable and desirable method for cataract surgery in patients with coloboma and cataract.
References
- Onwochei, Benjamin C et al. “Ocular Colobomata”. Survey of Ophthalmology 45.3 (2000): 175-194. Web.
- Nordlund ML, Sugar A, Moroi SE (2000) Phacoemulsification and intraocular lens placement in eyes with cataract and congenital coloboma: visual acuity and complications. J Cataract Refract Surg 26:1035–1040
- Khokhar, Sudarshan et al. “Outcomes Of Phacoemulsification In Eyes With Congenital Choroidal Coloboma”. Graefes Arch Clin Exp Ophthalmol 251.10 (2013): 2489-2490. Web.
- Bermejo E, Martinez-Frias ML. Congenital eye malformations: clinical–epidemiological analysis of 1,124,654 consecutive births in Spain. Am J Med Genet 1998; 75: 497–504
- Nakamura, Kelly M. “Incidence, Ocular Findings, And Systemic Associations Of Ocular Coloboma”. Archives of Ophthalmology 129.1 (2011): 69. Web.
- Klein BEK, Klein R, Linton KLP. Prevalence of age- related lens opacities in a population; the Beaver Dam Eye Study.Ophthalmol 1992; 99:546 –552
- Duke-Elder WS (1963) System of ophthalmology, vol 3, part 2. Mosby, St Louis, pp 456–487
- Elder MJ. Aetiology of severe visual impairment and blindness in microphthalmos. Br J Ophthalmol 1994; 78:332–334
- Robb RM. Developmental abnormalities of the eye affecting vision in the pediatric years. In: Albert DM, Jakobiec FA, eds, Principles and Practice of Ophthalmology. Philadelphia, PA, WB Saunders, 1994; 2791–2798
- Chaurasia S, Ramappa M, Sangwan VS (2012) Cataract surgery in eyes with congenital iridolenticularchoroidalcoloboma. Br J Ophthalmol 96:138–140