Dr. Ajay Aurora, A03243
AUTHORS
Dr Ajay Aurora
AIOS Membership Number A 03243
Prof Neetu Singh, MsVartikaDhyani
Centre for Biomedical Engineering, IIT Delhi
Dr Arjun Aurora
Intern, Maulana Azad Medical College
Address For Correspondence
Dr Ajay Aurora
Vision Plus Eye Centre
Kisan Tower
Golf Course Road
Sector51
NOIDA 201301
auroraajay@hotmail.com
ABSTRACT
Purpose
Puncturing rubber stopper of Avastin vial with 26/30 Gauge needle may cause coring and produce rubber slivers, which may get aspirated with Avastin and injected into eye. Our study assessif coring are produced by puncturing rubber stoppers and presents a safe Avastin Puncture Assist Device (APAD) that may help in reducing this risk.
Methods
The new APAD assists in methodically puncturing the Avastin vial without repeat entry through same track. This allows safe removal of drug through pre-numbered laser cut holes with 30G needle
Different Avastin Bottle Rubber stoppers were punctured 16 times each with 26 /30 & 23 gauge needles without APAD and with APAD. These were analysed by Scanning Electron Microscopy (EM) for the size of particles generated.An Energy Dispersive X-ray Microanalysis (EDX) was also carried out.
Results
There was a greater chance of having a sliver in the aspirate with 26G needle and without APAD.
Conclusion
Multiple puncturing of the Avastin rubber stopper is safer with 30G needle and with the use of new APAD.
Introduction
On insertion of a needle through the stopper of a medication vial, a small piece of the stopper is some times sheared off (known as coring). If air/fluid is injected into the vial the “cored sliver” could be pushed into the vial and may be noticed floating in the liquid medication. Because of its small size, personnel are not on the lookout for this, or if a label, a matching background, or colored vial blocks visualization, the coring may go unnoticed. If no fluid is injected into the vial this coring may get aspirated into the syringe with aspiration of the medication. This small foreign body may then get injected into the patient. The unintended presence of extraneous, mobile and undissolved particles in a parenteral solution or medication is called Particulate contamination. These particles can be of various sizes, defining them as detectable by visual inspection (in general ≥ 50 μm) or as sub-visible with a range of 2-50 μm in size in general. For many years the particulate contamination has been recognized as a potential health hazard but limited interventions have been introduced by the industry worldwide to reduce it and probably no effort has been made in India in this regard. In fact most Medical practioners questioned by the author were unaware of the problem.
The rate of coring reported in studies has varied widely, ranging from 3.1% to 97%. This high variance in prevalence is at least partially due to the detection method used. Studies that used microscopy detect coring particles at higher rates (1,2)than studies that did not use microscopy. Other variables have also been reported to potentially affect the rate of coring including the angle at which the needle is inserted into the vial, the use of sharp or blunt tip needles, the use of multiple or single use vials, and the type of stopper (3). It has also been suggested that rubber stoppers with larger surface core more often (4). In addition, a particular concern is that coring rates may be greater with low-quality stoppers (5).
In ophthalmic practice small-bore needles are used and after piercing the stopper, fluid from the vial (antiVEGF, antibiotics, steroidsetc.) are aspirated into the syringe and injected into the eye.
The purpose of this study was to see if the commonly used needles,26 and 30 gauges create coring in a laboratory situation? And if by altering the methodology of puncturing the rubber stopper, the incidence of coring can be reduced. This study has numerous unique features to its credit:
- There is no reported literature testing the chances of coring with the use of 26 and 30 Gauge needles on ophthalmic use solution.
- Introduces a new device APAD (Avastin Puncture Assist Device) that may help in reducing the incidence of coring of rubber stoppers and enable safe delivery of Avastin.
- The first study to our knowledge to report the analysis of coring by Scanning Electron Microscopy (SEM) and
- First study to understand the application of SEM/EDX (Scanning Electron Microscopy (SEM) used in tandem with Energy Dispersive X-ray Microanalysis (EDX) for understanding the chemical structure of rubber stopper coring.
Scanning Electron Microscopy (SEM) used in tandem with Energy Dispersive X-ray Microanalysis (EDX) is a combination of instrumentation, which is capable of providing detailed information on the nature, origin and transformations of environmental samples at the individual particle level. The strength of SEM/EDX analysis is its ability to gather data on the size, morphology and composition of the particles in a time efficient manner.
Methods
- All Rubber stoppers tested were from recently used Avastin Bottles that were maintained at 4-8 C.
- All the bottles were cleaned extensively with filtered deionized (DI) water by injecting the water into the bottles and aspirating the residual drug with a 26 Gauge needle with a single puncture.
- Next we injected 200µL water with each puncture (16 punctures were made randomly in each bottles).
- The punctures were made with a 23/ 26/30 gauge needle with and without using Avastin Puncture Assist Device (APAD) (Fig1,2&3)
- Next the sealed bottles were opened and the fluid from the bottles stored in a 24 well plate until further usage.
- The well plate was examined under microscope to check for slivers produced during multiple punctures.
- To analyze the morphologies of slivers, we drop casted the samples on a glass coverslip and coated the glass with gold with sputtering technique.
- For EDX, samples were tested against Control taken directly from the rubber stopper and mounted on an aluminum tape before testing.
APAD (Avastin Puncture Assist Device)
APAD is made of titanium and has been devised to directly puncture the Avastin bottle in a systematic manner in the operation theater and aspirate the aliquot of Avastin for Intravitreal administration.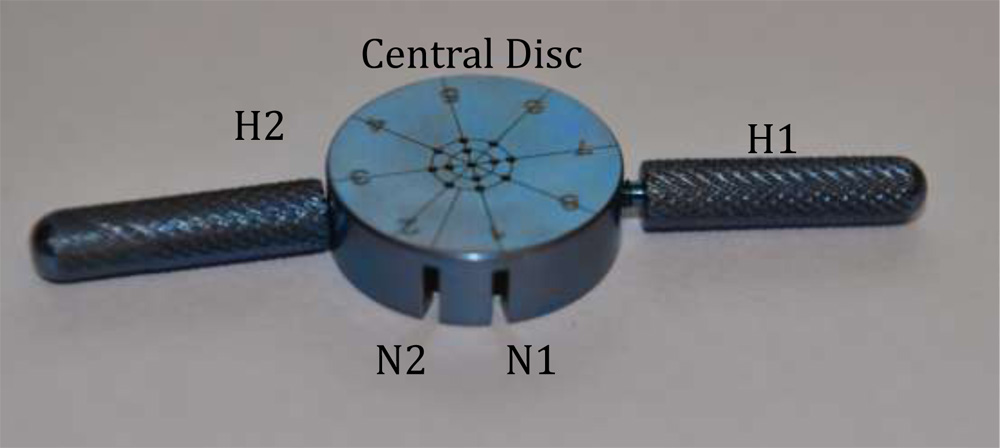
Figure 1 Avastin Puncture Assist Device (D: Central Disc of APAD; H1 & H2 Screwable Disc Handles: N1 Notch 1 on Axis 1: N2 Notch 2 (between Axis 1&2)
Central Disc: Has markings from 1 to 8; there are two circles drawn. The outer circle has a hole on each axis (8 holes) and inner circles that has a hole on alternate axis (Four holes). In addition there is a central hole.
Screwable Disc Handles (H1 & H2): These help to fix the APAD on the Avastin bottle and hold the Avastin Bottle for drug aspiration
Notch 1 & 2 (N1 & N2)Helps orient APAD to the mark on the Avastin Bottle

Figure 2: Avastin Bottle: The Red Line is used as the orientation linefor APAD
APAD allows puncturing of the Avastin bottle rubber stopper ina sequential manner without going through the same hole again. This is achieved by making N1 correspond to a fixed line on the Avastin Bottle (Red line on the label). After completing the puncturing of Avastin bottle once (8+4+1= 13 punctures); one can make the second notch N2 correspond to the same fixed red line on the Avastin Bottle. Now a new set of 12 punctures can be made on the Avastin bottle through the outer and inner circle of APAD. The Central hole is avoided on the second round. This way Avastin Bottle can be punctured 23 times without going through the same hole again. This allows a systematic Direct From the Vial aspiration of Avastin.
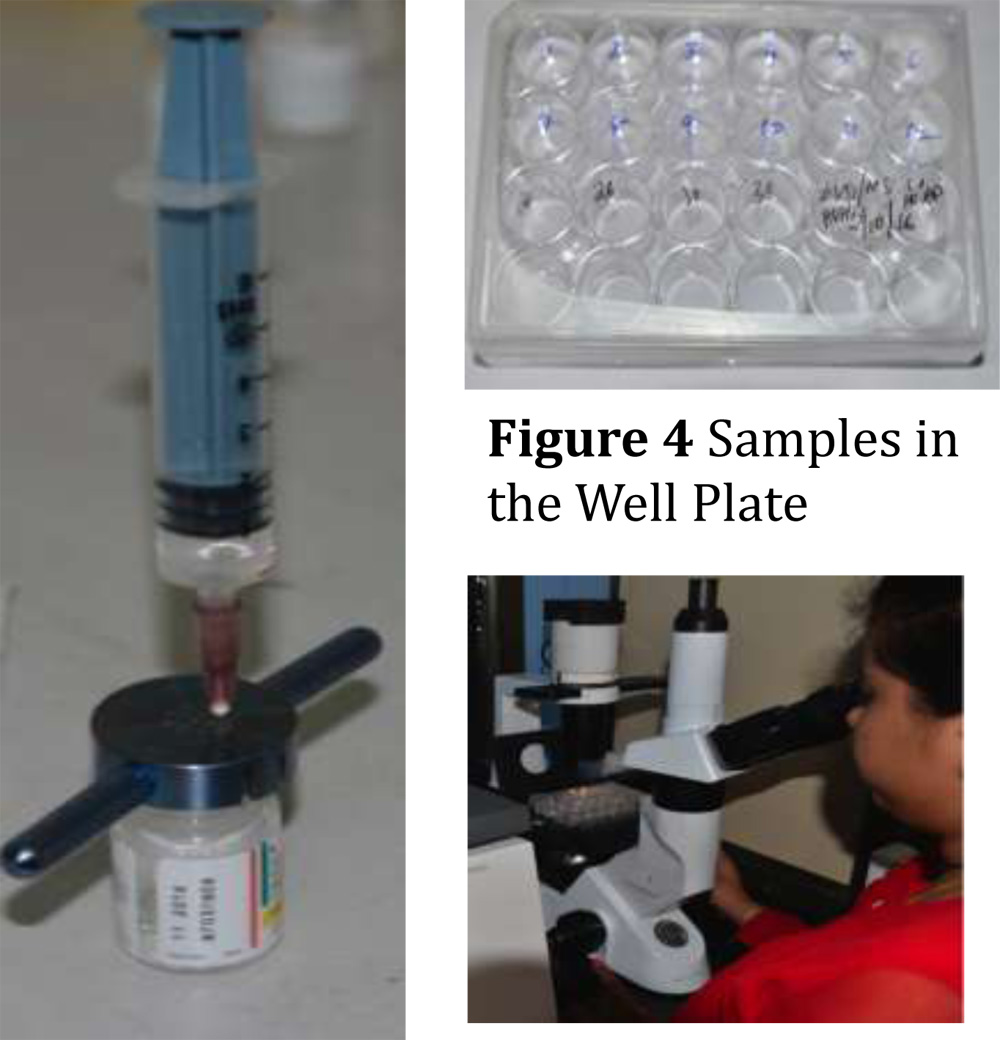
Figure3 APAD N2Oriented to RedLine on AvastinBottle
Figure5 Well Plate being examinedUnder Microscope
Results:
a) Particulate matter of different size and different density was found on examination of the well plate. It was observed that largest particles were in the well plates that consisted of fluid from bottles punctured with 23 Gauge needle. Similarly there was virtually no particulate matter when the rubber stopper was punctured with 30 gauge needle and with the use of APAD (Table1)
b)SEM (Scanning Electron Microscopy): The particles detected ranged from 1-10μ As the bore size increased the sliver particle size also increased. The particles size detected on SEM varied as follows:
| Gauge | Without APAD
Particle in μm |
With APAD
Particle in μm |
| 23 | 8-10 | 5-10 |
| 26 | 2-5 | 2-5 |
| 39 | 1-2 | 1-2 (very few)_ |
- EDX (Energy Dispersive X-ray Microanalysis):The elemental analysis of slivers was done by dispersing a small amount of solid in DI. A small amount of this suspension was then placed on an Aluminum tape and allowed to dry. Analytical data were collected for solids in each sample. The composition of these solids, as measured by EDX, shows the average Carbon and Oxygen contents of the solids spectra for control stopper and produced slivers and appears to have same compositions
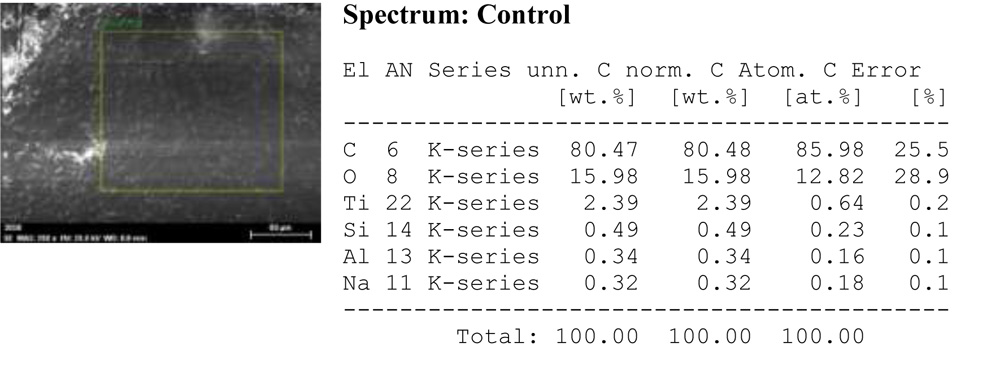
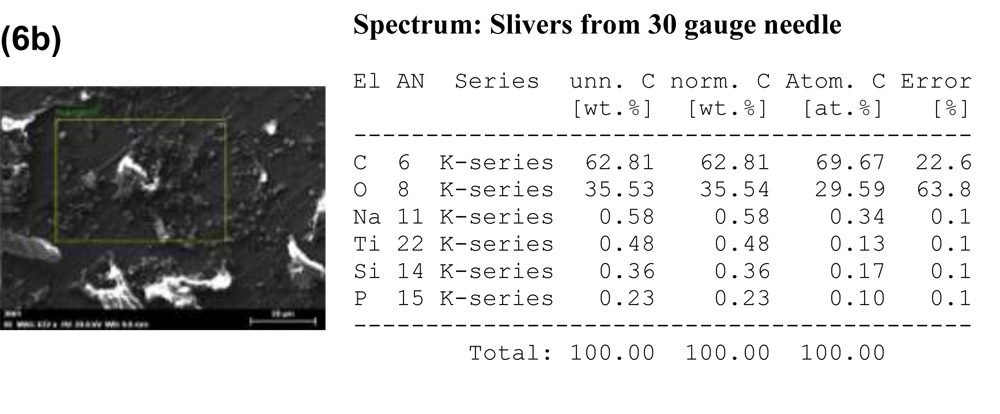
Figure 6: Energy Dispersive X-ray Analysis of (a) Control and (b) Slivers produced by a 30-gauge needle.
Discussion
Particulate contamination describes the unintended presence of extraneous, mobile and undissolved particles in a parenteral solution. These particles can be of various sizes, defining them as detectable by visual inspection (in general ≥ 50 μm) or as sub-visible with a range of 2-50 μm in size in general.
Coring of the stopper has been invoked to explain the cluster of case reports involving insulin. Asakura et al. examined the incidence of microscopic stopper fragmentation with pen type insulin injectors with an intrinsic DNR (Dried Natural Rubber) stopper in the cartridge. They demonstrated a high incidence of micro-scopic rubber fragments in the lumen of the needle prior to injection: 73% with the first puncture and 97% with the second (2). They further reported a high, but not defined, incidence of coring when small-gauge needles used for subcutaneous injection were used to puncture DNR vial stoppers, particularly when the vials had been refrigerated
Present study clearly demonstrates that rubber slivers are generated when the Avastin rubber stopper is punctured. The size of the particle is dependent on the size of the needle used as demonstrated by the SEM analysis. The chances of these particles to be present increases with the use of higher gauge needle and without use of APAD. This could be explained from the observation that without APAD we punctured the vial from its central zone as would be done in a clinical situation.This may mean that multiple entry into the vial from the central zone is likely to produce greater number of slivers than if these entries are divided into different zones of the stopper as is done with the assistance of APAD.This study also demonstrates that with a 30 Gauge needle particles as small as 1-2μm can be generated. Hence a filter that blocks particles larger than 1μm should be used. It is conjectural that these particles could be involved in an inflammatory response that occurs in some cases after injecting Bevacizumab or other antiVEGF
Table 1: Slivers seen under High Power field in well-plate
| Sample | 23 Gauge | 23 Gauge with APAD | 26 Gauge | 26Gauge with APAD | 30 Gauge | 30 Gauge with APAD |
| 1 | Present
>10 |
Present
>6 |
3-6 | 0-3 | 0-3 | 0 |
| 2 | Present
>10 |
Present
>6 |
3-6 | 0-3 | 0-3 | 0 |
Slivers per HPF (X100 mag)
References
1.Stein HA, Vu BL. Coring: A potential problem in eye surgery. J Cataract Refract Surg 1994;20:169-171.
2.Asakura T, Seino H, Nozaki S, Abe R. Occurrence of coring in insulin vials and possibility of rubber piece contamination by self- injection. Yakugaku Zasshi 2001;121:459-463.
3.Gragasin FS, van den Heever ZAN. The incidence of propofol vial coring with blunt needle use is reduced with angled puncture compared with perpendicular puncture. Anesth Analg 2015;120: 954-955.
4.Wani T, Wadhwa A, Tobias JD. The incidence of coring with blunt versus sharp needles. J Clin Anesth 2014;26:152-154.
5.Eskander J, Cotte J, Glenn E, Friedman S, Rosinia F. The incidence of coring and fragmentation of medication vial rubber stoppers. J Clin Anesth 2015;27:442-444.