Eliza Anthony, Chanchal Poddar, Jyotirmay Biswas
Abstract
Objective:To describe the diagnostic criteria,treatment and long term visual outcomes in ocular sarcoidosis.
Methods: Retrospective study
Results:150 eyes of 82 patients with sarcoid uveitis, mean age 40.59 ± 14.08years,were followed up for 32.96 months.Commonest symptom was diminution of vision(55.36%) and commonest signs were vitreous opacities(17.3%). Bilateralitywas seen in 26.4%.Vision improved in 38%,worsened in 32%,and maintained in 30% of eyes.Thirty eightpatients had recurrence.Most of the patients were diagnosed based on elevated ACE level(72 patients), mantoux test(19 patients) and HRCT chest(17 patients).Mean ACE level was 69.98±29.86.Diagnosis was definitive in 7 patients(8.54%), presumed in 18(21.95%),probable in 1(1.22%) and possible in none and 56 patients(68.29%) didn’t belong to any of these categories.Oral steroids(30.36%) and immunosuppressive(17.41%) were most common treatment modalities.
Conclusion:Both clinical suspicion and laboratory evidence are crucial in diagnosing sarcoid uveitis.
Full text
Introduction
Introduction
Sarcoidosis is a multisystem chronic granulomatous inflammatory disorder which was first described by Jonathan Hutchinson in 1878. Schumacher first described the ocular involvement in a patient with nodular iritis.1Ocular involvement can occur in more than 25-60% of sarcoidosis patients. But sometimes the involvement can be as high as 90%.2Sarcoiduveitis has been described as the presenting sign in 10-20% of patients.In 2/3rd of the patients, it is the most common intraocular manifestation.3Most characteristically it presents as bilateral granulomatous uveitis. Early diagnosis of sarcoid uveitis and ruling out other infective etiologies is very important especially in a tuberculosis (TB) endemic country like India.
We reviewed the electronic database of all consecutive patients diagnosed with sarcoid uveitis, seen by a single consultant at uveitis clinic of Sankara Nethralaya , Chennai, which is a tertiary care centre, between January 2011 and January 2016 .
Sarcoid uveitis was diagnosed as per International Workshop of Ocular Sarcoidosis, 20064 are listed in Table 1.
| Table 1: International Workshop of Ocular Sarcoidosis, 20064 | ||
| 1 | Biopsy supported diagnosis with compatible uveitis | Definitive ocular sarcoidosis |
| 2 | Biopsy not done, bilateral hilar lymphadenopathy with compatible uveitis | Presumed ocular sarcoidosis |
| 3 | Biopsy not done; chest radiograph normal; 3 suggestive signs out of 7* and 2 positive investigations** | Probable ocular sarcoidosis |
| 4 | Biopsy negative; 4 suggestive ocular signs* and 2 positive investigations** | Possible ocular sarcoidosis |
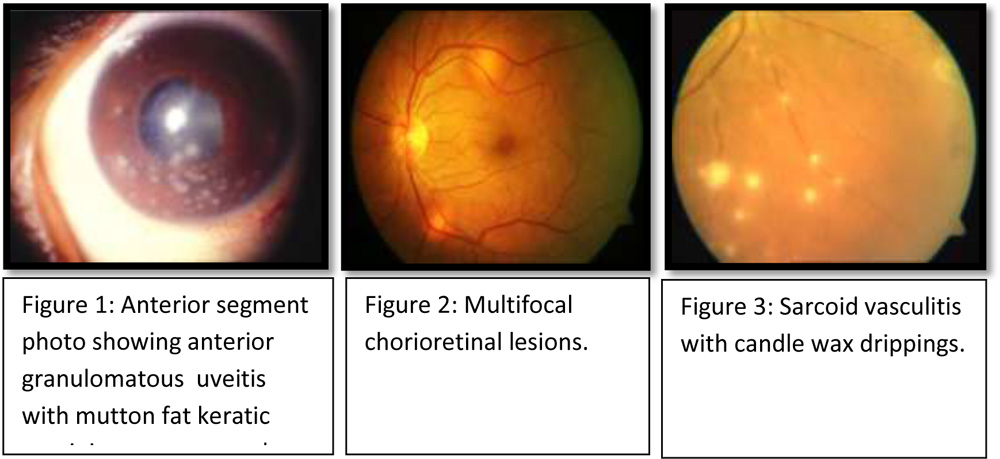
Following are the clinical signs* considered to make diagnosis of sarcoid uveitis:
| 1. Mutton fat keratic precipitates (Figure-1) and/or iris nodules at pupillary margin or on stroma. |
| 2. Trabecular meshwork nodules and/or tent-shaped peripheral anterior synechiae. |
| 3. Snowballs/string of pearls in vitreous or vitreous opacities. |
| 4. Multifocal peripheral chorioretinal lesions- active (figure-2) or atrophic. |
| 5. Nodular and/or segmental periphlebitis with or without candle wax exudates (Figure- 3) and/or macroaneurysms
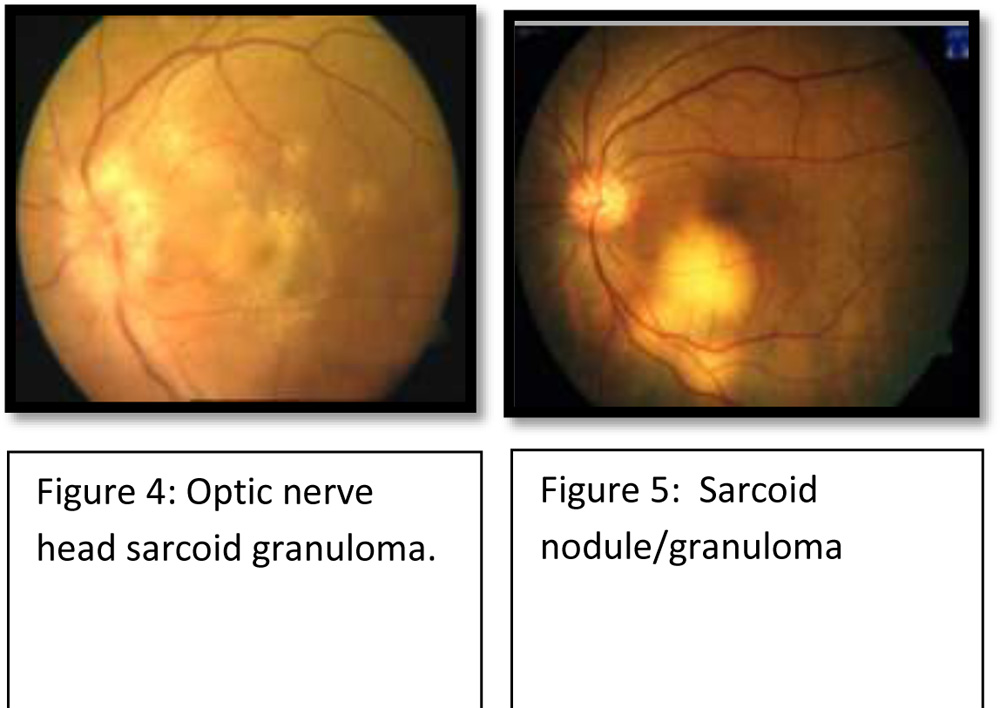
6.Optic disk nodule( Figure- 4 )/granuloma and /or solitary choroidal nodule(Figure- 5) 7.Bilateral inflammation (evident on clinical examination or investigational imaging ) |
The laboratory investigations** that were included were
1.Negative tuberculin skin test in a BCG-vaccinated patient or in a patient having had a positive tuberculin skin test previously.
2.Elevated serum angiotensin converting enzyme (ACE) levels and/or elevated serum lysozyme.
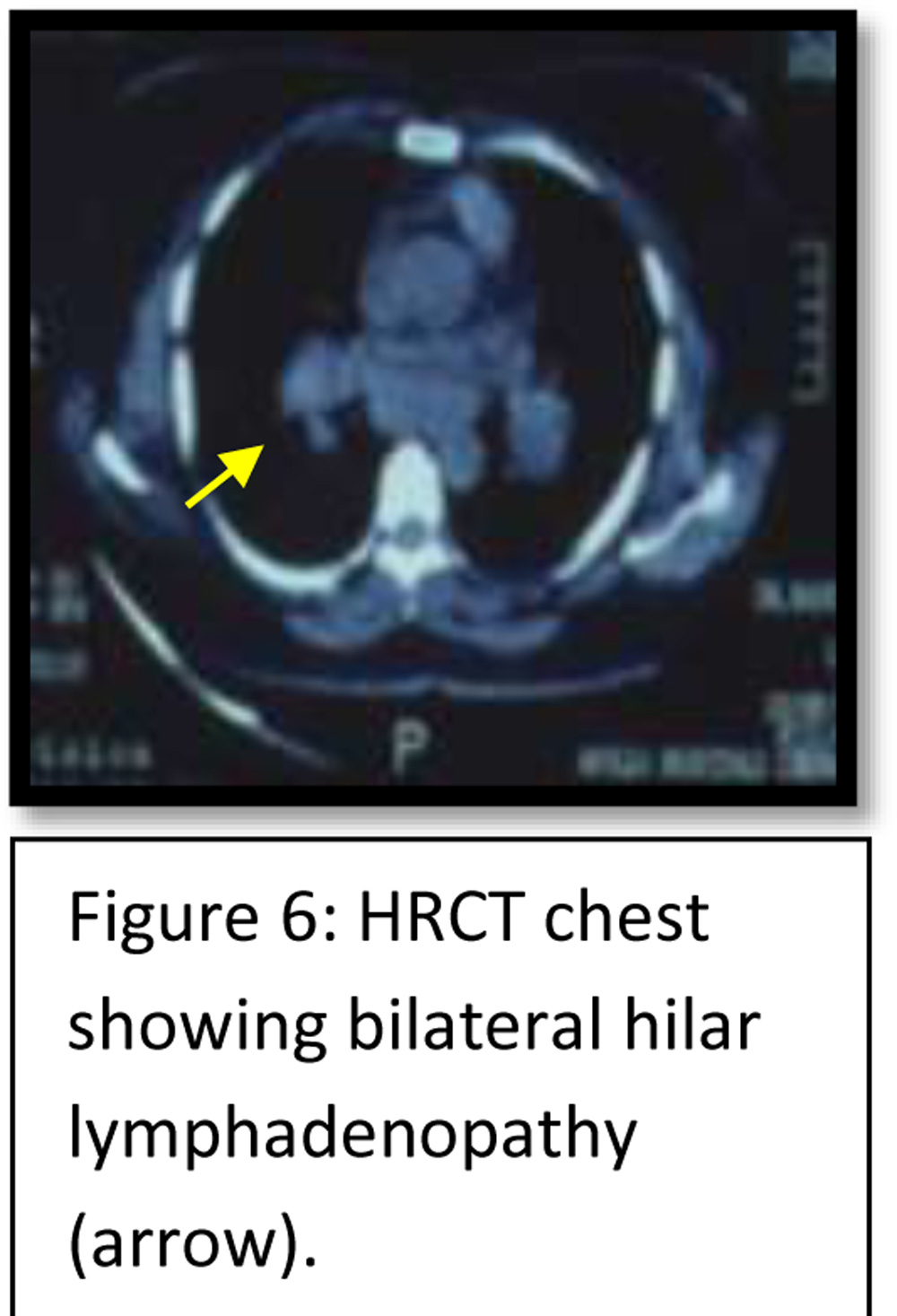
3.Chest radigraphy revealing bilateral hilar lymphadenopathy (BHL).
4.Abnormal liver enzyme tests
5.HRCT chest ( Figure 6) in patients with a negative chest x-ray result.
Patient with at least one positive investigation with ocular signs suggestive of sarcoid uveitis were included in a separate self prepared 5th category, which was not included in the international criteria. Patients with follow-up <3 months, infective etiology and inadequate documentation were excluded from the study. Institute Ethics Committee approval was obtained. The study adhered to the tenets of the Declaration of Helsinki. The data, including sex, age, clinical presentation, ocular involvement, associated systemic findings if any, current treatment at presentation, treatment given , duration of treatment , duration of follow up , number of recurrences, treatment of recurrences, visual outcome, complication, categorization based on above criteria were entered into a computer database. Best corrected visual acuity (BCVA) of eyes recorded and converted to logarithm of the minimal angle of resolution (logMAR) for statistical analysis. Data analysis was done using SPSS 14 version. P value < 0.05 was considered significant.
Results
We studied 150 eyes of 82 patients diagnosed with sarcoid uveitis. Among them,14 patients had unilateral disease and 68 patients had bilateral disease. Mean age of the patients was 40.59 ± 14.08 yrs.
There were 42 males (51.2%) and 40 females(48.8%).At presentation 136 eyes (90.6%) out of 150 eyes had bilateral disease. At presentation 29patients(35.37%) had recurrent disease and rest 53 patients(64.63%) were new cases.Among the 29 patients who had recurrent disease at presentation, 25 patients (86.21%)had bilateral disease and 4 patients(13.79%) had unilateral disease. Mean duration of symptoms was 438.26days+801 days. Blurring of vision was seen in 83 eyes (55%)followed by floaters in 29 eyes (19.3%), pain in 9 eyes (6 %) and redness in 11 eyes (7.3%).
Associated systemic diseases were hypertension in 12 patients(14.63%), diabetes mellitus in 10 patients (12.19%), dyslipidemia in 2 patients (2.43%), hypothyroidism in 2 patients(2.43%), chronic renal disease in 1 patient (1.22%), deafness and vertigo in 1 patient (1.22%), rheumatoid arthritis in 1 patient (1.22%),lymph node enlargement in 1 patient(1.22%), and 66.67% were systemically unremarkable. None of the patients had history of tuberculosis exposure. Only one patient had past history of tuberculosis (1.22%). History of joint pain was noted in 9 cases ( 10.97%), backache in 1 patient (1.22%), genital ulcers in 1 patient (1.22%) , deafness in 1 patient (1.22%)and atopic dermatitis in 1 patient (1.22%).
Fifteen patients (18.29%)were on oral steroids and topical steroids, 5 patients(6.09%) were on immunossuppressives, 2 patients(2.43%) had received posterior subtenons injection( PST ), 1 patient(1.22%) had received intravenous methylprednisolone, one patient(1.22%) was on anti tuberculous treatment (ATT) and 51 patients (62.19%) were not on any kind of treatment at presentation.
Mantoux test was done for 51 patients and it was positive in 19 patients (23.17%) and negative in 32 patients (39.02%). HRCT chest was done in 30 patients (36.59%) and was normal in 13 patients (15.85%). Chest radiography was done for 54 patients(65.85%) and was inconclusive in 6 patients (7.32%) and normal in 40 patients(48.78%). Bilateral hilarlympadenopathy was seen on HRCT chest in 17 patients (20.73%) and on chest radiography in 8 patients(9.76%). Polymerase chain reaction on vitreous sample was done in 5 patients(6.09%) and was negativein all. Biopsy was done in 7 patients (8.54%) and all were positive. Serum ACE levels were analyzed in 79 patients. Itwas found to be elevated in 72 patients (87.8%) and was within normal range in 7 patients (8.54%). Average ACE level was 69.98±29.86 IU. Serum lysozyme levels were analyzed in 43 patients(52.44%). They were elevated in 7 patients (8.54%) and within normal range 36 patients (43.9%). Liver function test were done in 31 patients(37.8%) and was abnormal in 8 patients (9.76%).QuantiFERON TB Gold test was done in 8 patients (9.76%), positive in 6 patients (7.32%)and negative in 2 patients (2.44%).
Most common treatment was oral steroids in 75 patients (91.46%) , immunossuppressives in 43 patients (52.44%), topical steroids in 39 patients(47.56%), posterior subtenons injection in 30 patients(36.58%), ATT in 8 patients (9.76%), IVMP in 7 patients (8.54%) , hydroxycholoroquine in 2 patients(2.4%) and no treatment was given in one case (1.22%).Oral steroids alone was used in 25 patients (30 %) and immunosuppressive alone in 14 patients (17 %) .Mean total time of treatment was 15.99±23.06 months. Mean time of treatment with steroids was 8.35 ±11.75 months, immunossuppresives was 4.90±7.30 months.
Mean total follow up time was 32.96±38.92 months. During the course of treatment 38 patients (46.34%) had recurrence .Mean number of recurrences were (n=38) 2.08±1.44. Among the 38 patients who had recurrences, 35 patients had bilateral involvement at presentation and had bilateral recurrence also. Rest 3 patients who had initially unilateral disease at presentation, also developed unilateral recurrence. Only in one patient fellow eye got involved. Recurrences were treated with systemic steroids in 30 patients (78.94%), PST in 3 patients (7.89%).
Mean visual acuity before treatment was 0.316±0.42 logMARunits and after treatment was 0.34±0.64 logmar units. Due to loss of follow up, final visual acuity was available only for 133 eyes. Out of theses 133 eyes in 51 eyes vision improved , in 42eyes vision worsened , and in 40 eyes vision maintained.
| Vision improved (n=51 eyes) | Vision worsened(n= 42 eyes) | Vision maintained (n=40 eyes) | ||
| Presenting visual acuity | 0.504±0.45 | 0.167±0.235 | 0.165±0.386 | P<0.001 |
| Final visual acuity | 0.147±0.23 | 0.726±0.94 | 0.16±0.39 | P<0.001 |
| Duration of symptoms | 349.8±704.01 | 559.63±823.63 | 450.34±891.49 | p=0.43 |
Clinically only 74 eyes (49.33%) had chorioretinal lesions. 4 eyes (6%) had solitary chorioretinal lesions and 68 eyes (45.33%) had multifocal chorioretinal lesions. In 29 eyes (19.33%) lesions were in form of choroidal nodule and in 48 eyes (32%) they were punctate chorioretinal lesions. Chorioretinal lesions were located at macula in 13 eyes (8.7%), extrafoveal in 59 eyes (39.3%), peripapillary in 6 eyes ( 4%) and foveal in 2 eyes (1.33%).
Out of 150 eyes, 110 eyes (73%) eyes had complications. 22 eyes (14.67%) had complicated cataract and in 17 eyes (11.33%) cataract surgery was performed. 12 eyes (8%) had cystoid macular edema which was treated with intravitreal triamcinalone injection in one eye (0.67%) and ozurdex injection in 3 eyes (2%). 10 eyes (6.67%) developed secondary glaucoma. In 9 eyes (6%) topical antiglaucoma medications were used, 4 eyes(2.67%) underwent trabeculectomy procedure and one eye cyclophotocoagulation in order to control the intraocular pressure.6 eyes(4%) had macular scaring. Four eyes (2.67%) had developed choroidal neovascular membrane(CNVM) which was managed by intravitreal vascular endothelial growth factor (anti VEGF) injections in 3 eyes, photodyanamic therapy(PDT) in 1 eye (0.67%). Optic atrophy was also present in 4 eyes (2.67%). Epiretinal membrane was present in 3 eyes (2%) and was surgically removed in 1 eye (0.67%). Retinal detachment occurred in 2 eyes (1.33%) and choroidal detachment in 1 eye (0.67%) and all three eyes were managed surgically. RPE alterations were present at macula in 1 eye (0.67%).
Based on diagnostic criteria, patients were classified into 5 categories – definitive sarcoidosis in 7 patients (8.54%), presumed sarcoidosis in 18 patients (21.95%), probable sarcoidosis in 1 patient (1.22%) and possible sarcoidosis in none . Fifty six patients (68.29%) had at least one positive investigation with ocular signs suggestive of sarcoid uveitis and they were included in a separate self prepared 5th category, which was not included in the original international criteria.
Discussion
Sarcoid uveitis is typically present a bilateral granulomatous uveitis5. In our study also at presentation 90.6% patients had bilateral presentation. Most of the patients, who developed recurrence, had bilateral disease at presentation as well as at the recurrence. Ocular sarcoidosis has been described to have predilection for female gender3 but in our study there was no gender predilection. Highest incidence was described between 20-40 years age group.5 Commonest ocular presentation in our study was blurring of vision followed by floaters. Ocular sarcoidosis has bimodal pattern of incidence, initially it can present at 20-30 years of age and later at 50-60 years of age.3 In our study mean age of patients was 40.59 ± 14.08 years. Although mean duration of symptoms was quiet long 51.29% of the patients were not on any kind of treatment at presentation. This fact highlights the lack of awareness among the people. Most common systemic disease associated was hypertension, although not significantly. Although mantoux test has been described negative in ocular sarcoidosis due to cutaneous anergy, but in our study 23.17% of patient had positive mantoux test. Cutaneous anergy is seen with other antigens also.6 Although chest radiography was done more frequently, hilar lyphadenopathy was diagnosed in 20.73% cases by HRCT chest as compared to 9.76% using chest radiography. Other studies have also described HRCT more sensitive than chest radiography in detecting hilar lymphadenopathy.7 In India where tuberculosis is an endemic disease, positive mantoux test might not be a very reliable to exclude the diagnosis of ocular sarcoidosis. It is reported that serum ACE levels are not very specific in diagnosing ocular sarcoidodsis . Serum ACE levels above 50units/liter are reported to be 84% sensitive and 95% specific.8 But in our study most common investigation done was analysis of serum ACE levels. They were elevated in 87.8% of patients. Serum lysozyme was not very helpful in diagnosing as it was elevated only in 8.54% of patients. However assessing its level is useful especially in patients on ACE inhibitors. Oral corticosteroids are mainstay of treatment for ocular sarcoidosis. In case of optic nerve and macular involvement intravenous corticosteroids are used.3, 6 In our study also, most common treatment was oral steroids followed by immunossuppressives. We had a long follow up period during which 46.34 % of patients had recurrence mostly in previously affected eyes. These recurrences were managed with oral corticosteroids. Although the group in which vision improved had a worse presenting visual acuity but had a shorter duration of symptoms compared to group in which vision maintained or worsened. Most common types of lesions were multifocal, extrafoveal punctuate lesions. Various ocular complications that have been described in sarcoid uveitis are cystoids macular edema, complicated cataract, secondary glaucoma, retinal ischemia, optic disk edema, vascular occlusions, retinal and optic disk neovascularization, vitreous hemorrhage and retinal detachment. Inflammatory neovascular membranes have also been reported in few studies. Band-shaped keratopathy is observed in chronic cases. 3, 5 In our study the most common complication was complicated cataract and cystoids macular edema. Cataract surgery was done for significant complicated cataract. Mainstay of management for uveitic macular edema was oral corticosteroids. Only in few cases intravitreal triamcinalone and ozurdex injection was given. Throughout the follow up intraocular pressures were monitored and secondary glaucoma was an infrequent complication, present only in 10 eyes. In a previously reported case of inflammatory CNVM associated with sarcoidosis, patient was treated only with oral corticosteroids thereby avoiding anti VEGFs, as steroids not only suppress inflammation but also downregulates vascular endothelial growth factor9. But in our study as patients were already on oral steroids, inflammatory CNVM in 4 eyes, were managed with intravitreal anti VEGF injection in 3 eyes and PDT in one eye. Thus it is very important to manage the inflammation as well as the complications, which finally determines the visual outcome.
Conclusion
Both clinical suspicion and laboratory evidence are crucial in diagnosing sarcoid uveitis. Clinical criteria supported by chest imaging and blood test helps in diagnosing sarcoid uveitis although we cannot strictly abide by diagnostic criteria as many eyes inspite of not satisfying international criteria were clinically very much suggestive of sarcoid uveitis. Further research and mutlicentric studies are required to establish diagnostic criteria as sarcoid uveitis can have a variable presentation, along with many genetic and enviromental associations also. Treatment of sarcoid uveitis should be initiated early. Both clinical suspicion and laboratory evidence are crucial in diagnosing sarcoid uveitis. A long follow up with prompt management of complications plays a very crucial role in determining the visual outcome .
References
- Schumacher G. Fall von beiderseitiger Iridocyclitis chronica bei Boeckschem multiplem benignem Sarkoid. Munch Med Wochenschr. 1909;56:2664.
- Babu K, Kini R, Mehta R, Abraham MP, Subbakrishna DK, Murthy KR. Clinical profile of ocular sarcoidosis in a South Indian patient population. Ocular immunology and inflammation. 2010 Oct 1;18(5):362-9.
- Robert Nusenblatt HNS. Posterior uveitis and collagen vascular disease. In: Color atlas and synopsis of clinical ophthalmology wills eye institute. Lipincott Williams and Wilkins; 2012. p. 65–71.
- Herbort CP, Rao NA, Mochizuki M, the members of the Scientific Committee of the First International Workshop on Ocular Sarcoidosis (IWOS). International criteria for the diagnosis of ocular sarcoidosis: results of the first International Workshop On Ocular Sarcoidosis (IWOS). Ocular immunology and inflammation. 2009 Jan 1;17(3):160-9.
- J.Biswas,P.D majumdar BK. Ocular sarcoidosis. In: Uveitis An Update. Springer India; 2016. p. 133–41.
- Foster CS CM. Sarcoidosis. In: Diagnosis andtreatment of uveitis. Jaypee Highlights; 2013. p. 967.
- Chung YM, Lin YC, Liu YT, Chang SC, Liu HN, Hsu WH. Uveitis with biopsy-proven sarcoidosis in Chinese—a study of 60 patients in a uveitis clinic over a period of 20 years. Journal of the Chinese Medical Association. 2007 Nov 30;70(11):492-6.
- Baarsma GS, La Hey E, Glasius E, De Vries J, Kijlstra A. The predictive value of serum angiotensin converting enzyme and lysozyme levels in the diagnosis of ocular sarcoidosis. American journal of ophthalmology. 1987 Sep 30;104(3):211-7.
- Shoughy SS, Jaroudi MO, Tabbara KF. Regression of peripapillary choroidal neovascular membrane in a patient with sarcoidosis after oral steroid therapy. Saudi Journal of Ophthalmology. 2014 Jun 30;28(2):160-2.