Dr. Sanjana, Dr. Sri Ganesh, Dr. Sheetal Brar
INTRODUCTION
Various treatment options available for management of low myopia , in the current scenario are – LASIK , PRK, Intacs and the latest all femtosecond, flapless procedure, ReLEx SMILE
Photorefractive keratectomy (PRK) has been used since a long time for treatment of myopia. It has been shown to correct myopia ranging from -1 to -12 D. Due to significant postoperative pain, relatively slow visual recovery and haze development, especially when treating high myopia, (1-3) the intrastromal LASIK procedure was invented (4). LASIK virtually eliminated the previously mentioned drawbacks, but instead flap-related complications developed, as well as a higher risk of corneal ectasia. Surface ablation of the cornea is therefore, by some, considered the overall safest procedure for treatment of low to moderate myopia.(5-8) Outcomes from eyes with low myopia were generally superior to outcomes from eyes with high myopia. Treatment of higher degrees of myopia with standard PRK should only be done today under special circumstances, due to low refractive predictability, and high risk of corneal haze. The introduction of mitomycin C and modern surface ablation techniques has also increased the range of treatment and lowered the risk of haze and regression after PRK. (9-13)
Laser in-situ keratomileusis (LASIK) is the current laser refractive procedure of choice to treat myopia. The advantages of LASIK include early postoperative improvement and stabilization of visual acuity, minimal postoperative patient discomfort, and the possibility of enhancement in the future [14]. However, side effects such as dry eyes, reduced vision in low lighting conditions, and visual distortions such as glare and haloes can still occur in up to 1% to 2% of cases; while flap-related complications, inflammation, or infection, though rare, can have serious consequences [15,16].
Due to these potential complications of LASIK and its application in thin corneas, PRK is again gaining popularity due to its safety in treatment of low degrees of myopia.
ReLEx SMILE has recently evolved as a new technique for correction of myopia upto -10 D SEQ, and astigmatism upto 5 D. It is an all femtosecond, minimally invasive, technique which involves creation of a refractive lenticule followed by its extraction through a 2 mm incision. (17,18) It has advantages over LASIK, in terms of better biomechanical stability (19), no flap related complications, less induction of dry eyes and aberrations, (20,21) and faster post operative recovery. It has been proposed that this technique may be better and more stable for treating higher powers compared to LASIK, as the biomechanical strength after SMILE is not compromised much due to intactness of Bowmans membrane and conservation of strong anterior corneal lamellae. Also, the residual stromal bed thickness is stated to be more compared to LASIK, as the cap also contributes to the residual bed thickness.
Hence, this study has been undertaken with the aim of comparing the safety and efficacy of ReLEx SMILE and PRK as both of them are flapless procedures for the correction of low myopia and study their long term results.
MATERIALS AND METHODS
This prospective, non randomised, comparative, interventional trial included eligible patients of both gender, who underwent PRK and ReLEx SMILE for correction of low myopia and myopic astigmatism at our centre (Myopia with SEQ < – 4 D with cylinder upto – 2 D); and included patients between 21 to 40 years of age, stable corneal conditions within the last 12 months, stable refraction since past 12 months (<0.5D change within past 12 months), healthy ocular surface with stable tear film, discontinuation of soft contact lenses 1 week, and rigid contact lenses 3 weeks prior to surgery.
Patients who had thin corneas (corneal pachymetry <480µ), any ectatic condition of the cornea including keratoconus, Pellucid marginal degeneration, corneal scars, severe dry eye, patients with any other ocular morbidity leading to loss of vision were excluded from the study.
PREOPERATIVE, POSTOPERATIVE MEASUREMENTS
A written,informed consent was obtained from all patients in accordance with the tenets of the Declaration of Helsinki. Preoperative and postoperative measurements at 15 days and 3 months included uncorrected (UDVA) and corrected (CDVA) distant visual acuity, manifest and cycloplegic refraction, intraocular pressure measurement by Goldmann applanation tonometry, slit lamp biomicroscopy examination, dilated fundus examination, dry eye assessment (Schirmer’s I and II), topography [Orbscan (Bausch & Lomb-Technolas, Munchen, Germany) and Pentacam (Oculus Inc, Arlington, WA, USA)], contrast sensitivity assessment (FACT, Stereo Optical Co., Inc., Chicago, Ilinois, USA) and aberrometry (iTrace; Tracey Technologies, Houston, TX).
SURGICAL TECHNIQUE
All surgeries were performed by a single experienced surgeon (Dr.SG) under topical anaesthesia.
ReLEx SMILE surgical technique
Each SMILE procedure was performed on the VisuMax femtosecond laser (Carl Zeiss Meditec AG) using an established, described technique [22]. After application of topical anesthesia, standard sterile draping, and insertion of the speculum, the patient’s eye was centered and docked with the curved interface cone before application of suction fixation. The laser was then activated for photo-dissection in the following sequence: first the posterior surface of the refractive lenticule (spiral in), then the lenticule border was created. The anterior surface of the refractive lenticule (spiral out) was then formed which extended beyond the posterior lenticule diameter by 0.5 mm followed by a 2mm access incision at 12 o’clock. The following FS laser parameters were used: 100 μm cap thickness, 7.5 mm cap diameter, 6 – 7 mm optical zone of lenticule, 145 nj of power with side cut angles at 90°. Following creation of lenticule, the incision was opened to identify the two planes of lenticule. A thin blunt spatula was used to dissect the superficial and deep planes of the lenticule and to break the remaining tissue bridges thus separating the lenticule from the surrounding stroma. This lenticule was grasped with a pair of forceps and extracted through the 2mm incision. The corneal interface was then flushed with balanced salt solution.
Alcohol assisted PRK surgical technique
Under topical anaesthesia, a 9mm optical zone marker was applied firmly to the corneal surface, centered on the visual axis, and filled with 20% ethanol in balanced salt solution. After 30 seconds, the ethanol was absorbed with a sponge, with care taken to avoid spillage on the areas not being treated; the cornea washed with Balanced Salt Solution (BSS). The loose epithelium was then removed as a sheet by lifting the edge of the loosened epithelium with sharp Beaver blade.
Eximer laser ablation was then carried out using the MEL 90 (Carl Zeiss Meditec AG). After the ablation procedure, Mitomycin- C 0.02% was applied to the ablated surface for 20 seconds, and washed with copious BSS and bandage contact lens applied, which was removed after 4 days of surgery.
Ethics approval was obtained from our Institutional Ethics Committee (IEC Ref No: 2014/26) and this trial was registered (Clinical Trials Registry- India CTRI/2014/10/005084).
Adverse events
All subjects were monitored for adverse events. All adverse events or serious adverse events were reported to institution ethics committee.
STASTICAL ANALYSIS
Microsoft Excel 2010 (Microsoft Corp., Redmond, WA) was used for data entry. Data was entered into Microsoft Excel data sheet and was analyzed using Statistical Package for the Social Sciences software (version 22, SPSS Inc, Chicago, IL, USA). Categorical data was represented in the form of frequencies and proportions. Continuous data was represented as mean and standard deviation. Independent t-test was used as test of significance to identify the mean difference between two groups (PRK and SMILE). Paired t-test was the test of significance for paired data i.e. before and after values. A p value <0.05 was considered as statistically significant.
RESULTS
The study included 120 eyes from 60 patients who satisfied the inclusion criteria.
Patients were divided into 2 groups on the basis of the refractive procedure performed:
- ReLEx SMILE group : 60 eyes of 30 patients
- PRK group : 60 eyes of 30 patients
PRE OPERATIVE DATA
| PRE-OP PARAMETERS | PRK | SMILE | P-VALUE |
| AGE (Yrs) | 25.80 ± 4.697 | 26.8 ± 4.719 | 0.247 |
| FEMALES | 63.33% | 63.33% | |
| MALES | 36.67% | 36.67% | |
| D SPH | -2.08 ± 0.966 | -2.87 ± 1.038 | 0.0001* |
| DCYL | -0.31 ± 0.364 | -0.41 ± 0.475 | 0.180 |
| SEQ (D) | -2.23 ± 0.92 | -3.08 ± 1.031 | 0.0001* |
| BCVA (Log MAR) | 0.00 ± 0.00 | 0.003 ± 0.018 | 0.156 |
| SCHIRMERS 1 (mm) | 31.60 ± 3.227 | 30.82 ± 5.78 | 0.362 |
| SCHIRMERS 2 (mm) | 23.47 ± 5.74 | 23.73 ± 8.39 | 0.849 |
| PUPIL SIZE (mm) | 4.59 ± 0.525 | 4.358 ± 0.683 | 0.040* |
| CCT (µm) | 546.86 ± 40.23 | 545.13 ± 37.4 | 0.808 |
| HOA (Rms) | 0.124 ± 0.055 | 0.113 ± 0.052 | 0.288 |
| MEAN-K (D) | 44.05 ± 1.44 | 43.84 ± 1.17 | 0.401 |
In this study mean spherical power (DSPH) in PRK group was -2.08 ± 0.966 and in SMILE group was -2.87 ± 1.038. The difference was statistically different between two groups. The mean cylindrical power (DCYL) in PRK group was -0.31 ± 0.364 and in SMILE group was -0.41 ± 0.475. There was no significant difference in mean between two groups. The mean Spherical Equivalent (SEQ) was higher in the SMILE group compared to the PRK group and was statistically significant. BCVA was 0.00 logmar in PRK group , as against 0.003 in SMILE group. The difference was not statistically signifiant. Schirmers 1 and 2 in PRK group was 31.60 ± 3.227 mm and 23.47 ± 5.74mm respectively in PRK group , while it was 30.82 ± 5.78 mm and 23.73 ± 8.39 mm respectively . The difference between the 2 groups was not statistically significant. CCT was 546.86 ± 40.23µ in PRK group and 545.13 ± 37.4µ in SMILE group. HOA were 0.124 ± 0.055µ in PRK group and 0.113 ± 0.052µ in SMILE group.
CUMULATIVE SNELLENS VISUAL ACUITY 20/20 OR BETTER 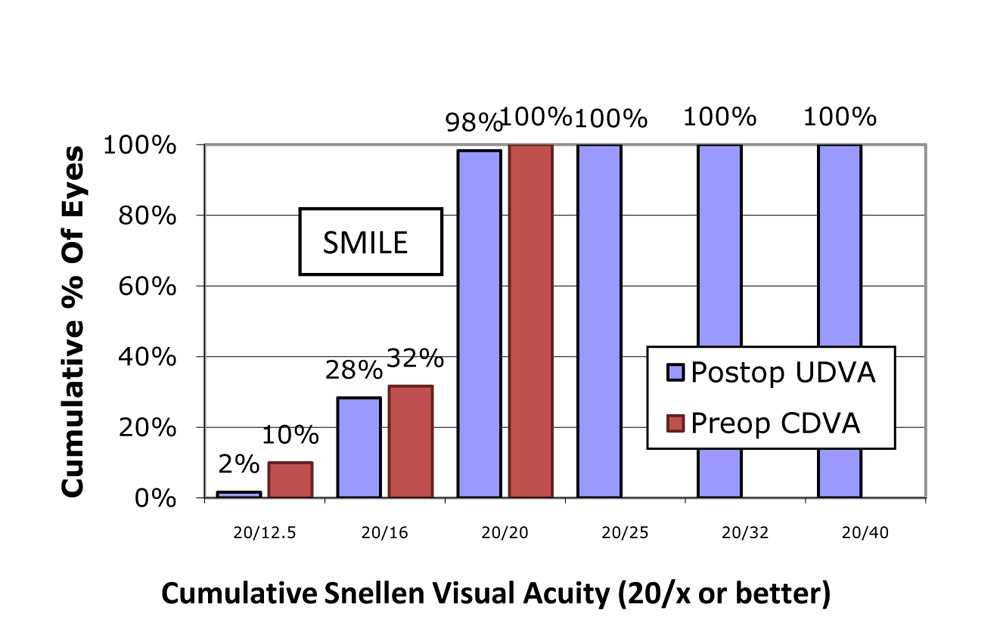 In the SMILE group,100% of eyes had post op Cumulative snellens UCVA of 20/20 , and 30% had better than 20/20
In the SMILE group,100% of eyes had post op Cumulative snellens UCVA of 20/20 , and 30% had better than 20/20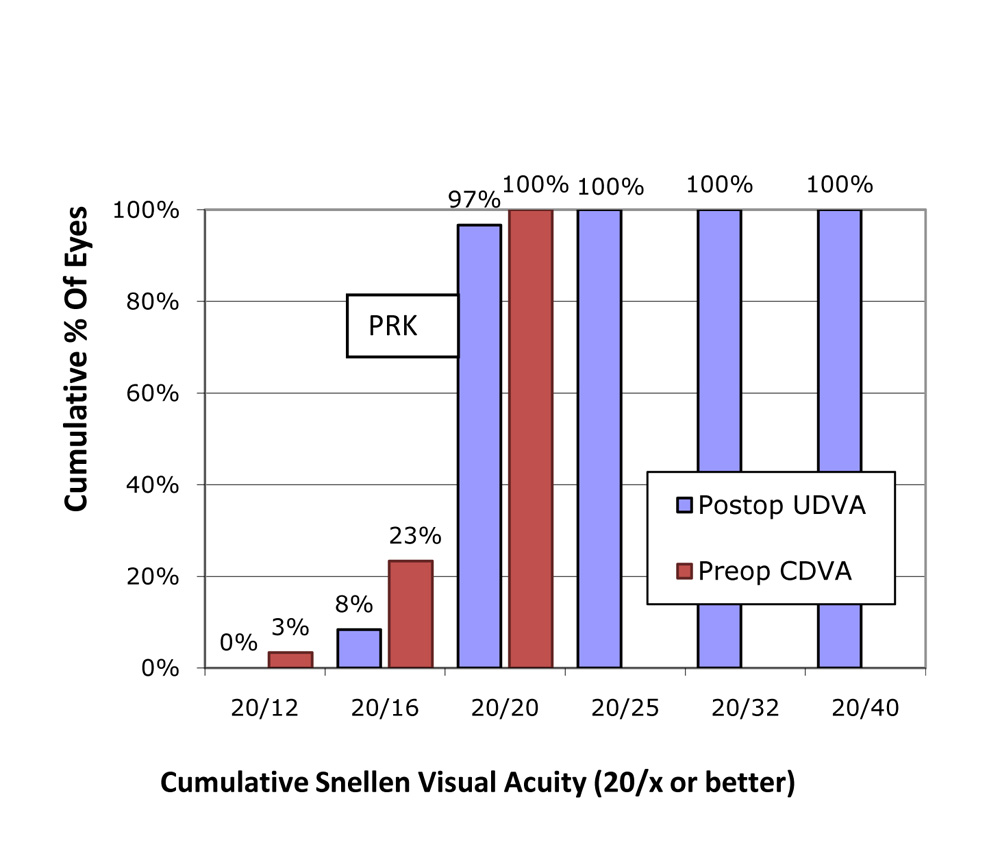 In the PRK group, 97% of eyes had post op Cumulative snellens UCVA of 20/20 , and 8% had better than 20/20.
In the PRK group, 97% of eyes had post op Cumulative snellens UCVA of 20/20 , and 8% had better than 20/20.
PERCENTAGE WITHIN ATTEMPTED – EFFICACY 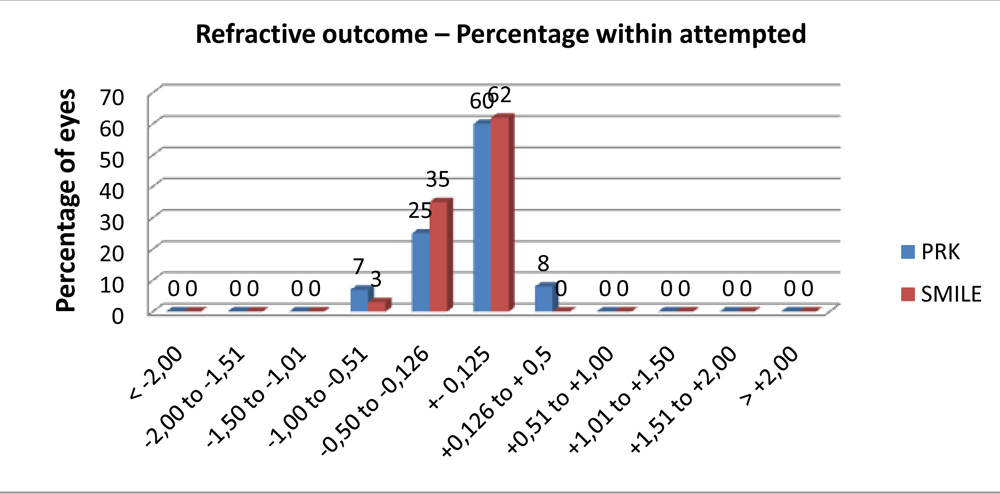 97 % of eyes had refraction within ±0.5D in SMILE group , while 85% had within ±0.5D in PRK group
97 % of eyes had refraction within ±0.5D in SMILE group , while 85% had within ±0.5D in PRK group
PERCENTAGE SAFETY
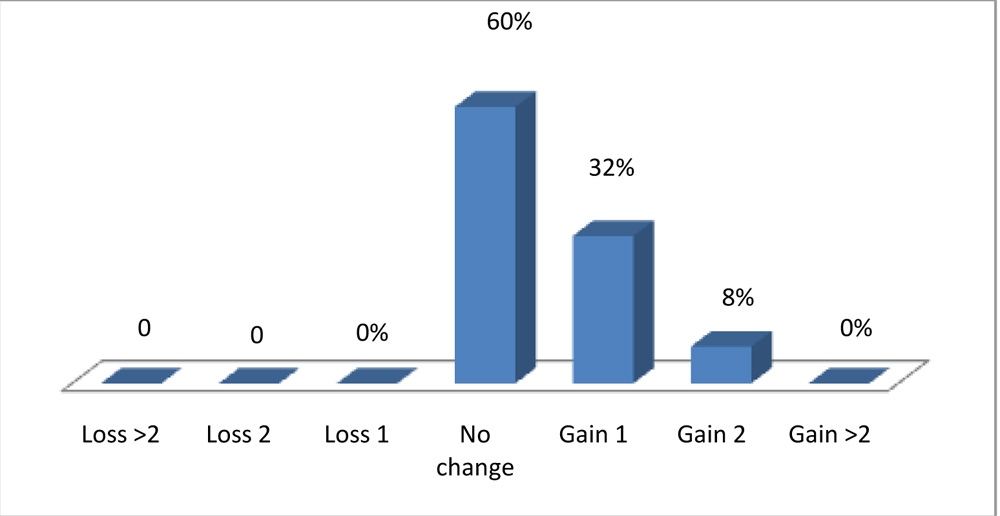 In SMILE group, 60 % of eyes had no change in visual acuity, 32 % gad gain in 1 line and 8% had gain in 2 lines , while no eyes had loss of lines.
In SMILE group, 60 % of eyes had no change in visual acuity, 32 % gad gain in 1 line and 8% had gain in 2 lines , while no eyes had loss of lines.
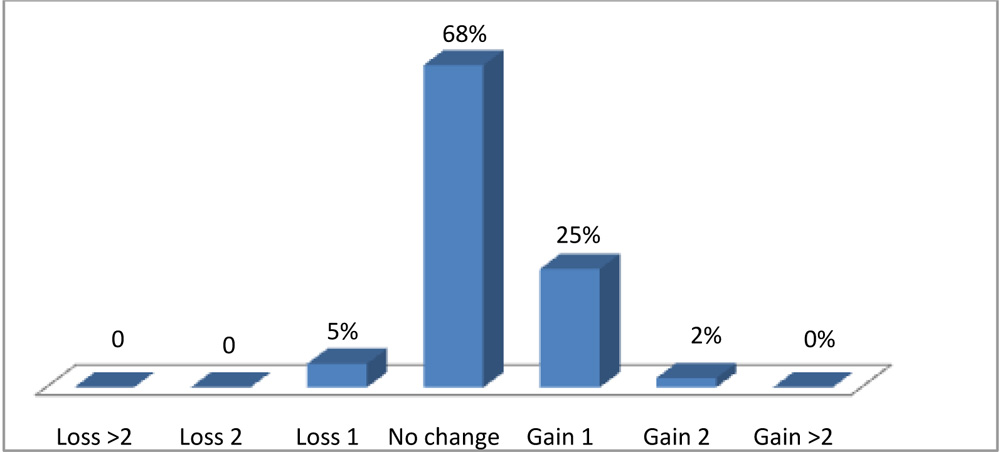 In PRK group, 68 % had no change, 25% had gain in 1 line , 2% of eyes had gain in 2 lines while 5% had loss of 1 line.
In PRK group, 68 % had no change, 25% had gain in 1 line , 2% of eyes had gain in 2 lines while 5% had loss of 1 line.
STABILITY OF SPHERICAL EQUIVALENT REFRACTION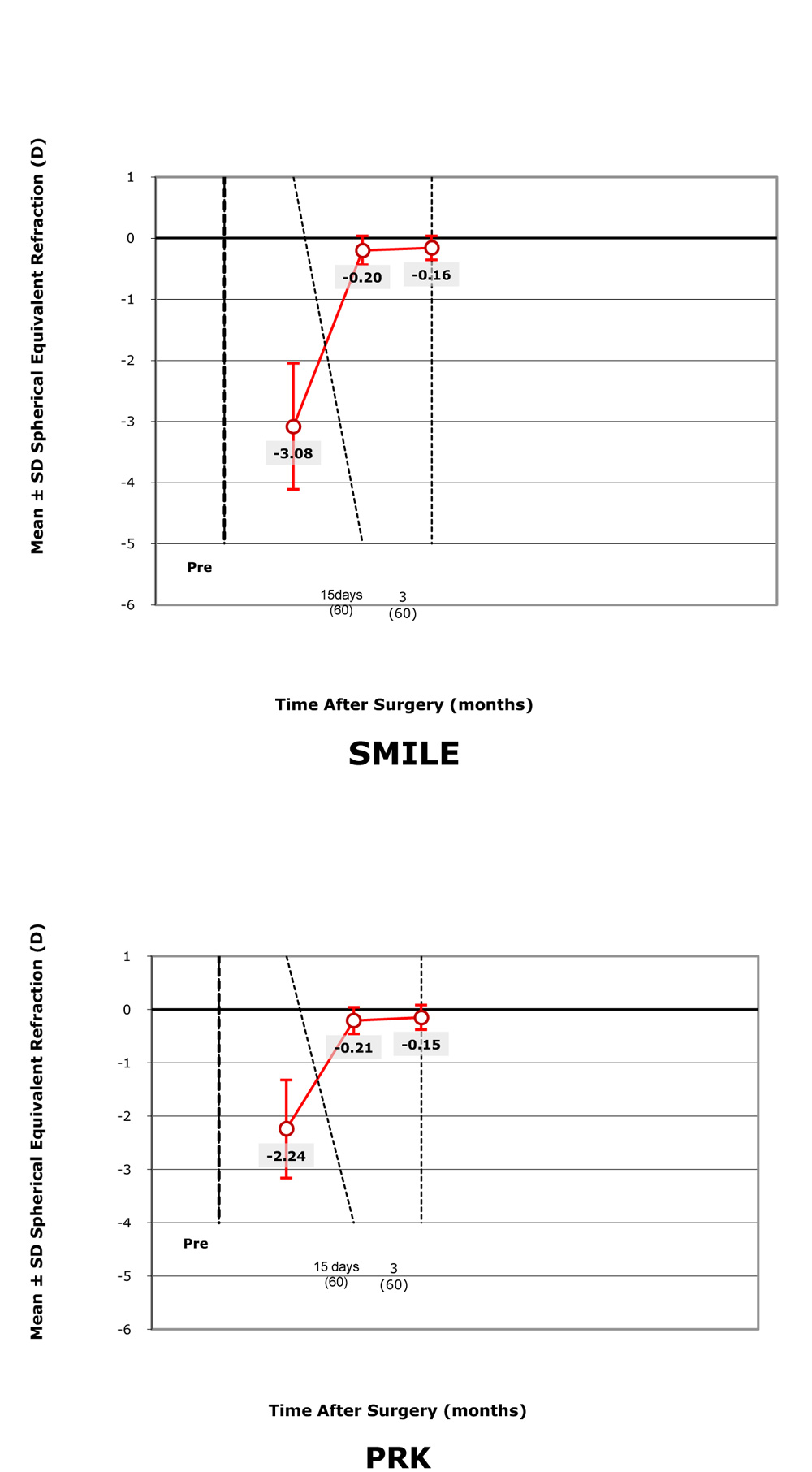 Both SMILE and PRK group shows stable SEQ Refraction at the end of 3 months.
Both SMILE and PRK group shows stable SEQ Refraction at the end of 3 months.
POST OP PARAMETERS
| 3 month Post-op parameters | PRK | SMILE | p-value |
| UCVA (Log MAR) | -0.061 ± 0.066 | -0.013 ± 0.034 | <0.0001* |
| CDVA (Log MAR) | -0.091 ± 0.064 | -0.046 ± 0.062 | <0.0001* |
| Residual SE (D) | -0.14 ± 0.23 | -0.15 ± 0.19 | 0.722 |
| HOA (RMS) | 0.169 ± 0.062 | 0.144 ± 0.059 | 0.022* |
| CCT (µm) | 495.28 ± 45.85 | 468.31 ± 42.06 | 0.001* |
| Schirmers 1 (mm) | 30.35 ± 3.35 | 29.68 ± 5.5 | 0.081 |
| Schirmers 2 (mm) | 22.1 ± 5.72 | 22.73 ± 7.29 | 0.081 |
| Mean K (D) | 42.06 ± 1.41 | 41.66 ± 1.42 | 0.125 |
At the end of 3 months post op, UCVA (Log MAR) was -0.061 ± 0.066 and -0.013 ± 0.034 , in PRK and SMILE group respectively. CDVA (Log MAR) was -0.091 ± 0.064 in PRK group and -0.046 ± 0.062 in SMILE group. The difference in UCVA and BCVA was statistically significant between the groups . HOA were 0.169 ± 0.062 and 0.144 ± 0.059 in PRK and SMILE group respectively and the difference was statistically different. CCT was 495.28 ± 45.85 in PRK group and 468.31 ± 42.06 in SMILE group. Schirmers 1 (mm) and Schirmers 2 (mm) in PRK group was 30.35 ± 3.35 and 22.1 ± 5.72 respectively while it was 29.68 ± 5.5 and 22.73 ± 7.29 respectively in SMILE group. The difference was not statistically significant .
DISCUSSION
The current study showed that both SMILE and PRK were effective in correction of low myopia, however SMILE scored slightly better in terms of safety, efficacy and lesser inductions of aberrations. This could represent a differential healing response between both procedures23
97 % of eyes had post op refraction within ± 0.5D in SMILE group , while 85% had within ± 0.5D in PRK group. This difference in the post op refraction can be attributable to the differential healing response between the 2 procedures. PRK utilizes ultraviolet light from excimer laser to reshape the corneal curvature through direct photoablation. SMILE uses femtosecond laser in near infrared spectrum to achieve the cutting effect within the cornea through photodisruption. The amount of energy delivered to the cornea is much lower with femtosecond laser compared to excimer laser24. The main advantage of femtosecond laser compared to excimer laser is its high cutting precision with minimal collateral damage and associated cellular and structural changes 23. The response of corneal epithelium may also be different between SMILE and PRK. This is important because epithelial hyperplasia has been observed following treatment after PRK 25,26. Healing of corneal epithelium and stromal remodeling could influence the refractive outcomes.
Also, variation in hydration of the corneal stroma is the most likely cause for underablation or overablation of stromal tissue. 27,28,29 .In PRK, after the removal of epithelium, the stroma is exposed to hydration changes before refractive correction. On the other hand, in SMILE, the refractive lenticule is cut by a femtosecond laser prior to any disturbance of the stroma. It is likely that this difference contributed to greater predictability
No eyes in SMILE group showed loss of lines , while 5% of eyes in PRK group showed loss of 1 line at the end of 3 months post op .It has been known that the corneal wound-healing response after refractive surgical procedures is a complex cascade. 27.Epithelial injury triggers release of inflammatory mediators like cytokines and growth factors,30,31,32.33 which induce keratocyte apoptosis. The surrounding live keratocytes are activated and transformed into fibroblasts or myofibroblasts, and migrate to repopulate the depleted stroma. This possibly explains the formation of stromal haze post operatively in PRK treated eyes and hence the cause of drop in BCVA.
In the current study, significant differences were not found in refraction diopters between the SMILE and PRK groups postoperatively. In general, both procedures were effective, but a longer follow-up period is essential to further verify the stability of the results.
Schirmers 1 and 2 values were comparable in both SMILE and PRK treated eyes and there was no significant dry eyes in either of the groups .
We found total HOAs were significantly lower in the SMILE group compared to the PRK group at end of 3 months. The aspheric smart ablation profile was used in SMILE and PRK groups in our study, so corneal curvature was not an explanation for the significant differences in HOA. Development of epithelial haze and irregular epithelial healing might have been the important reason for the induction of more HOAs in PRK group.
The ablation efficiency reduction caused by the excimer laser and the healing process associated with corneal remodeling are also the reasons for the increased HOAs. 34 There is less wound healing response and inflammatory infiltration after SMILE in comparison with PRK, suggesting that SMILE may result in fewer topographic changes and less HOA induction, which may favorably affect visual results. 35
Also other important factors which influenced better results in SMILE in low myopic correction were: Fixation was along the line of sight, Peripheral thickness of the lenticule was increased, Lesser distortion of the superficial layer, No intraop complications- cap tear/ lenticule retention and were done under the hands of a well experienced surgeon
CONCLUSION
Both SMILE and PRK are efficaceous for correction of low myopia, HoweverSMILE has few added advantages like:
- Better safety than PRK (No loss of lines in SMILE group)
- Lesser post operative discomfort
- Faster recovery
- Use of medications for a shorter duration.
REFERENCES
- Ehlers N, Hjortdal JO: Excimer laser refractive keratectomy for high myopia. 6-month follow-up of patients treated bilaterally. Acta Ophthalmol (Copenh) 1992, 70:578–586
- Gartry DS, Kerr Muir MG, Marshall J : Excimer laser photorefractive keratectomy: 18-month follow-up. Ophthalmology 1992, 99: 1209–1219
- Rosman M, Alio JL, Ortiz D, Perez-Santonja JJ : Comparison of LASIK and photorefractive keratectomy for myopia from -10.00 to -18.00 diopters 10 years after surgery. J Refract Surg 2010, 26: 168–176
- Pallikaris IG, Papatzanaki ME, Stathi EZ, Frenschock O & Georgiadis A (1990): Laser in situ keratomileusis. Lasers Surg Med 1990, 10: 463–468
- Lee JB, Kim JS, Choe C, Seong GJ, Kim EK (2001): Comparison of two procedures: photorefractive keratectomy versus laser in situ keratomileusis for low to moderate myopia. Jpn J Ophthalmol 2001, 45: 487–491
- Rao SK, Srinivasan B, Sitalakshmi G, Padmanabhan P : Photorefractive keratectomy versus laser in situ keratomileusis to prevent keratectasia after corneal ablation. J Cataract Refract Surg 2004, 30: 2623-2628
- Ghadhfan F, Al-Rajhi A, Wagoner MD : Laser in situ keratomileusis versus surface ablation: visual outcomes and complications. J Cataract Refract Surg 2007, 33: 2041-2048
- Hodge C, Lawless M, Sutton G : Keratectasia following LASIK in a patient with uncomplicated PRK in the fellow eye. J Cataract Refract Surg 2011, 37: 603–607
- Carones F, Vigo L, Scandola E, Vacchini L : Evaluation of the prophylactic use of mitomycin-C to inhibit haze formation after photorefractive keratectomy. J Cataract Refract Surg 2002, 28: 2088-2095
- Bedei A, Marabotti A, Giannecchini I, Ferretti C, Montagnani M, Martinucci C, Barabesi L : Photorefractive keratectomy in high myopic defects with or without intraoperative mitomycin C: 1-year results. Eur J Ophthalmol 2006, 16: 229-234
- Shalaby A, Kaye GB , Gimbel HV : Mitomycin C in photorefractive keratectomy. J Refract Surg 2009, 25:93-97
- Teus MA, de Benito-Llopis L, Alio JL (2009): Mitomycin C in corneal refractive surgery. Surv Ophthalmol 2009, 54: 487-502
- Hofmeister EM, Bishop FM, Kaupp SE, Schallhorn SC (2013): Randomized dose-response analysis of mitomycin-C to prevent haze after photorefractive keratectomy for high myopia. J Cataract Refract Surg 2013, 39:1358-1365
- Sugar A, Rapuano CJ, Culbertson WW, Huang D, Varley GA, Agapitos PJ, de Luise VP, Koch DD: Laser in situ keratomileusis for myopia and astigmatism: safety and efficacy: a report by the American Academy of Ophthalmology. Ophthalmology 2002, 109:175–187
- Salomao MQ, Wilson SE: Femtosecond laser in laser in situ keratomileusis. J Cataract Refract Surg 2010, 36:1024–1032
- Moshirfar M, Gardiner JP, Schliesser JA, Espandar L, Feiz V, Mifflin MD, Chang JC: Laser in situ keratomileusis flap complications using mechanical microkeratome versus femtosecond laser: retrospective comparison. J Cataract Refract Surg 2010, 36:1925–1933
- Shah R, Shah S, Sengupta S. Results of small incision lenticule extraction: All-in-one femtosecond laser refractive surgery. J Cataract Refract Surg 2011; 37: 127-137
- Wang Y,Wu Z, Tang X, Zhang J, et al. Two millimeter micro incision lenticule extraction surgery with minimal invasion: a preliminary clinical report. Zhonghua Yan Ke Za Zhi. 2014 Sep;50(9):671-80
- Pedersen IB,Bak-Nielsen S, Vestergaard AH, Ivarsen A, Hjortdal J. Corneal biomechanical properties after LASIK, ReLEx flex, and ReLEx smile by Scheimpflug-based dynamic tonometry. Graefes Arch Clin Exp Ophthalmol. 2014 Aug;252(8):1329-35
- Lin F, Xu Y, Yang Y.Comparison of the visual results after SMILE and femtosecond laser-assisted LASIK for myopia. J Refract Surg 2014, 30:248-254
- Xu Y, Yang Y:Dry eye after small incision lenticule extraction and LASIK for myopia. J Refract Surg 2014, 30:186-190
- Sekundo W, Kunert KS, Blum M: Small incision corneal refractive surgery using the small incision lenticule extraction (SMILE) procedure for the correction of myopia and myopic astigmatism: results of a 6 month prospective study. Br J Ophthalmol 2011, 95:335–339
- Wei, S. et al.Ultrastructural Changes and Corneal Wound Healing After SMILE and PRK Procedures. Curr Eye Res, 1–10, doi: 10.3109/02713683.2015.1114653 (2016).
- Riau, A. K.et al. Early corneal wound healing and inflammatory responses after refractive lenticule extraction (ReLEx). Invest Ophthalmol Vis Sci 52, 6213–6221, doi: 10.1167/iovs.11-7439 (2011).
- Ivarsen, A., Fledelius, W. & Hjortdal, J. O. Three-year changes in epithelial and stromal thickness after PRK or LASIK for high myopia. Invest Ophthalmol Vis Sci 50, 2061–2066, doi: 10.1167/iovs.08-2853 (2009)
- Reinstein, D. Z., Ameline, B., Puech, M., Montefiore, G. & Laroche, L. VHF digital ultrasound three-dimensional scanning in the diagnosis of myopic regression after corneal refractive surgery. J Refract Surg 21, 480–484 (2005).
- Sekundo W, Kunert KS, Blum M. Small incision corneal refractive surgery using the small incision lenticule extraction (SMILE) procedure for the correction of myopia and myopic astigmatism: results of a 6 month prospective study. Br J Ophthalmol 2011;95:335–9
- Sekundo W, Kunert K, Russmann C, et al. First efficacy and safety study of femtosecond lenticule extraction for the correction of myopia: six-month results. J Cataract Refract Surg 2008;34:1513–20
- Blum M, Kunert K, Schröder M, et al. Femtosecond lenticule extraction for the correction of myopia: preliminary 6-month results. Graefes Arch Clin Exp Ophthalmol 2010;248:1019–27
- Tuominen IS, Tervo TM, Teppo AM, et al. Human tear fluid PDGF-BB, TNF-alpha and TGF-beta1 vs corneal haze and regeneration of corneal epithelium and subbasal nerve plexus after PRK. Exp Eye Res2001;72:631–41
- Wilson SE, He YG, Weng J, et al. Epithelial injury induces keratocyte apoptosis: hypothesized role for the interleukin-1 system in the modulation of corneal tissue organization and wound healing. Exp Eye Res1996;62:325–7
- Mohan RR, Mohan RR, Kim WJ, et al. Modulation of TNF-alpha induced apoptosis in corneal fibroblasts by transcription factor NF-kb. Invest Ophthalmol Vis Sci 2000;41:1327–34
- Wilson SE, Chen L, Mohan RR, et al. Expression of HGF, KGF, EGF and receptor messenger RNAs following corneal epithelial wounding. Exp Eye Res 1999;68:377–97 [PubMed]
- Kwon Y, Bott S. Postsurgery corneal asphericity and spherical aberration due to ablation efficiency reduction and corneal remodeling in refractive surgeries.Eye (Lond). 2009;23:1845–1850. doi:10.1038/eye.2008.356
- Riau AK, Angunawela RI, Chaurasia SS, Lee WS, Tan DT, Mehta JS. Early corneal wound healing and inflammatory responses after refractive lenticule extraction (ReLEx).Invest Ophthalmol Vis Sci. 2011;52:6213–6221