Dr. Amit Raj, R12161, Dr. Meenakshi Sindhu, Dr. Ravi Kant Bamotra, Dr.Sudesh Kumar Arya
Dr.Amit Raj, Dr. Meenakshi Sindhu,Dr. Ravi Kant Bamotra and Prof. Sudesh Kumar Arya
Introduction
Canalicular lacerations are breaks(interruptions) in normal tear drainage system involving medial part of eyelid. Eyelid injuries occur commonly as a result of blunt or sharp peri-ocular injuries and may involve canalicular lacerations especially when medial canthal region is affected. Canalicular lacerations occur relatively infrequently but their improper management may lead to long term morbidity from epiphora, discharge, ocular irritation and dermatitis.
Herzum and associates reported that lesions of lacrimal drainage system are known to occur in 16% of all eyelid injuries.1 Canalicular injuries is reported to be more common in children and young adults and frequently affects the lower canaliculus.2 Though there is general agreement on the need for bicanalicular injuries,controversy still exists regarding the repair of a single lacerated canliculus.3
A single lacerated canaliculus has been traditionally managed with either an annular stent using the pigtail probe,or with a bicanalicular nasal intubation. The use of pigtail probe was less preferred attributable to the poor results, and risk of injury to the uninvolved canaliculus.1,4 Various surgical treatment techniques and materials have been previously described such as Crawford(bicanlicular),Ritleng(bicanlicular) intubation systems and Mini Monoka stents(unicanalicular). Mini Monoka stent due to its self retaining properties and inert silicone material is now standard procedure for monocanalicular as well as bicanalicular lacerations.
In this study, we describe epidemiology of canalicular lacerations managed at a tertiary eye hospital in northern india and report our experience with Mini Monoka stent in the management of monocanalicular as well as bicanalicular lacerations.
Methods:
Retrospective review of patients reported with canalicular lacerations in whom Mini Monoka stent was used for repair of canalicular lacerations and analyzed during the period of January 2014 and December 2015 . Demographics, involvement of canaliculi, mode of injury,any associated trauma and time of repair since injury was analyzed. Extrusion of stent and probable cause was also analyzed. Mini Monoka stent was used for monocanalicular as well as bicanalicular lacerations. The stent was kept in-situ for 4-6 months. A patent canaliculus on diagnostic probing (Hard stop) was defined as anatomic success whereas absence of epiphora was defined as functional success.
Results
Out of total 12 canalicular lacerations which were repaired with Mini monoka stent,8 had lower canalicular lacerations,1 had upper canalicular laceration while 3 had both upper and lower canaliculus involvement(Fig.1). Mean age of patients was 34.08 years (range 9-58 years) and most of them were males (92%). The most common mode of injury was roadside accidents (75%) followed by assault. The mean time following trauma to repair was 11.75 hours and all cases repaired within 24 hours.2 cases were associated with orbital wall fracture while 1 case was associated with open globe injury. Open globe injury was associated upper canalicular laceration. The stent extrusion was seen in 2 cases within 1 month,out of them in one case wound infection occured. Mean time of removal of Mini Monoka stent(Fig.2) was 4.2 months. The anatomical success was found in 11 cases (91.7%) cases while the functional success was seen in 10 cases (83.3%).
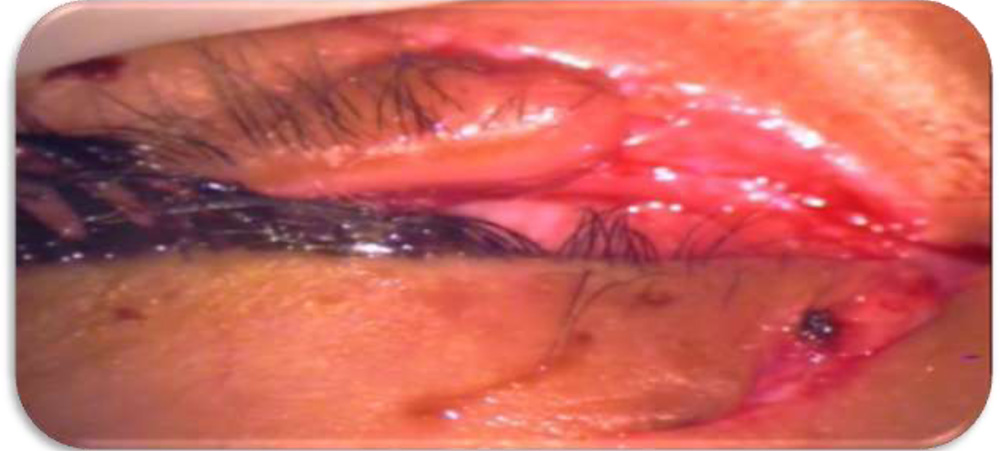
Figure1- Left eye upper and lower lid lacerations with canalicular involvement

Figure 2- one month post canalicular repair with Mini Monoka Stent
Discussion
Canalicular lacerations are usually associated with eyelid lacerations. The literature on epidemiology and management of canalicular lacerations is limited.
Herzum et.al. reported 16% canalicular involvement in a series of 180 patients with eyelid injuries while Naik et.al. reported 36% canalicular involvement in 66 patients with eyelid injuries.1,5 we are sharing 12 patients with canalicular involvement.
Kennedy and associates in a 11 year epidemiologic and clinical study,noted that two thirds of canalicular injuries occurred in children or young adults below 30 years of age2similarly in our series also mean age was 34 years and most of the patients were in younger age group.
Kennedy and associates reported lower eyelid involvement in 66.2% of cases, upper eyelid in 27.5% and bicanalicular involvement in 6.2% cases.2 Similarly,our study showed lower eyelid involvement in 66.6% cases, bicanalicular involvement in 25% cases while upper canaliculus was involved in only 8.3% of cases.
Epiphora is reported to be more common with bicanalicular injuries or when no canalicular stent is placed at the time of surgical repair.2 Immediate repair of laceration with stenting of canaliculus is currently the most preferred treatment approach for bicanalicular injuries.3
There is no consensus regarding the exact duration for which canaliculus should remain stented to achieve long term patency. Various authors have recommended the duration of canalicular stent varying from three to twelve months.6 we maintained stent in our cases for 4-6 months.
The main purpose of treatment is to repair lacerated canaliculus by stenting damaged lacrimal system. Surgical procedures usually aim to perform an anastomosis within the lacerated canaliculus and intubate this canalicular system until the re-epithelialisation of canalicula occurs.
We suggest that Mini Monoka monocanalicular stent is a simple, minimally invasive tool for reconstruction of traumatic monocanalicular as well as bicanalicular lacerations.
Conclusion
Canalicular injuries if repaired within 48 hours lead to higher success anatomically as well as functionally.MiniMonokabeing a monocanalicular stent prevents undue manipulation/trauma to the other uninvolved canaliculus which is manipulated in standard bicanalicular silicone stents.
References:
- HerzumH,HolleyP,Hintschich C. Eyelid injuries : epidemiological aspects Ophthalmologe 2001;98:1079-1082
- Kennedy RH, May J,Dailey J, Flanagan JC. Canalicular laceration. An 11 year epidemiologic and clinical study. OphthalPlastReconstrSurg 1990;6:46-53.
- Reifler DM. Management of canalicular laceration. Surv Ophthalmol 1991;36:113-132
- Saunders DH, Shannon GM,Flanagan JC. The effectiveness of pigtail probe method of repairing canalicular lacerations. Ophthalmic Surg. 1978;9:33-40.
- Naik MN, Kelapure A, Rath S, Honavar SG. Management of canalicular lacerations: Epidemiological aspects and experience with Mini Monoka monocanalicular stents. Am J Ophthalmol 2008;145 no.2: 375-e2.
- Kersten RC, Kulwin DR. “one stitch” canalicular repair.A simplified approach for repair of canalicular laceration. Ophthalmology 1996;103:785-789