Dr. Dhaval Patel, Dr.Dipankar Das, Dr. Diva Kant Misra
Chief and presenting author- Dhaval Patel
Co-authors: Dipankar Das (D08987), DivakantMisra (M15899)
Synopsis
Gnathostomiasis is a rare parasitic infestation of humans who become incidental hosts after intake of undercooked or raw meat of the definitive host .We describe 3 cases of intraocular Gnathostomiasis with detailed documentation. The parasites were fixed in a neutral buffered solution of 1% glutaraldehyde and 4% formaldehyde and sent for pathological examination. This is the first report where electron microscopy and Energy-dispersive X-ray spectroscopy was done for detailed examination of parasite. EDX spectroscopy of spine of Gnathostomiasis was done which showed positive spikes for sulphur, copper and calcium. Eventually the parasite was surgically removed in all the cases which was documented meticulously. Based on our experience with intraocular parasites we propose and describe a novel algorithm for rapid diagnosis of intraocular parasitic infections.
Introduction
Gnathostomiasis is a rare parasitic infestation of humans who become incidental hosts after intake of raw or undercooked meat of the definitive host (dogs, cats and wild animals), second intermediate host (frogs, freshwater fish, snilas and chicken), or paratenic host (birds).After ingestion, the larvae penetrate the gastric or intestinal wall and migrate haphazardly throughout the body.1Clinical manifestation of the disease occurs due to mechanical damage of the host tissue caused by migration of the parasitic larvae and host response to gnathostoma toxins resembling those to protease, hyaluronidase, acetylcholine, and hemolysin.1 The most common parasitic manifestation in humans is cutaneous in the form of larvae migrans, but visceral involvement in the lungs, gastrointestinal tract, genitourinary tract, ear, central nervous system and eye have been reported.1Of the forms of visceral gnathostomiasis, central nervous system infestation is the commonest, whereas ocular involvement is rare. We report a case of intravitrealgnathostomiasis where clinical presentation, surgical management, and scanning electron microscopic features and newer rapid diagnostic method of the retrieved larva.
Case Report 1
40 year old male presented to our outpatient department with chief complain of severe lacrimation, photophobia, pain and redness in the right eye since 1 week. His medical history was not significant. He was non vegetarian with fish as staplediet. On examination his best corrected visual acuity was 6/12 in the right eye and 6/6 in the left eye. Slit- lamp examination of the anterior segment of the left eye was unremarkable. In the right eye therewas lid edema and conjunctival congestion.Cornea was clear. On anterior chamber examination a 3-4mm free floating wormwas present at around 6 o’clock position.(Fig.1)Extra ocular movements were normal. Pupillary reflex was normal. The lens and the ocular media were clear, and there were no signs of cellular reaction. Fundus examination was within normal limits. Intraocular pressure was normal. Findings of neurologic and dermatologic evaluations were not remarkable.
Results of laboratory investigations including determination of complete blood cell count and routine stool and urine examinations were within normal limits. The condition and treatment explained to the patient in detail. He underwent surgical removal of parasite. Under aspetic and antiseptic precaution anterior chamber entry was done with 150 side port at 11 o’clock. Viscoelastic substance injected into anterior chamber and viscodelivery of parasite was done. Post operatively patient was advised topical atropine, steroid and antibiotic eye drops, as well as oral steroids.
Case Report 2
49 year old male presented with chief complain of pain, redness, photophobia in the right eye and headache since 2 days. His medical history was not significant. On examination his best corrected visual acuity was 6/9 in the right eye and 6/6 in the left eye. Results of slit- lamp examination of the anterior segment of the left eye were unremarkable. In the right eye the findings noted were lid edema, conjunctival congestion and aclear cornea . On anterior chamber examination there was no cellular reaction and live worm was lodged into the iris stroma around 10 o’clock position.(Fig.2) Extra ocular movements were normal. Pupillary reflex was sluggish. The lens and the ocular media were clear, and there were no signs of cellular reaction. Fundus examination was within normal limit. Intraocular pressure was normal. Findings of neurologic and dermatologic evaluations was not remarkable.
Results of laboratory investigations including determination of complete blood cell count and routine stool and urine examinations were within normal limits. The condition and treatment explained to the patient in detail. He underwent surgical removal of parasite. Under aspetic and antiseptic precaution,Infusion cannula (AC maintainer) was inserted to maintain the anterior chamber and IntracameralLignocaine injected.3 sideportswere made with MVR blade. Iris repositor was inserted and worm freed from surrounding stroma.Then Flute needle wasinserted and the parasite removed. Post operatively,patient was advised topical atropine, steroid and antibiotic eye drops, as well as oral steroids.
Case Report 3
A 48-year-old woman presented with complaints of decreased vision and a floater in the left eye of 6 days’ duration. The onset of symptoms was sudden .It was first noticed when getting up from bed in the morning. Her medical history was otherwise unremarkable except for bouts of an agonizing, left-sided headache and eye ache unexplained by neurologic and computed tomography evaluations of the brain. She was a non vegetarian,fish being the staple diet and gavehistory of occasional intake of smoked fish. On examination , her best corrected visual acuity was 6/6 in the right eye and 6/9 in the left eye. She was orthophoric with full range of ocular movements. Pupillary reflexes were normal. Results of slit- lamp examination of the anterior segment of the right eye were unremarkable. In the left eye, there was sludging of blood circulation in the conjunctival and episcleral blood vessels. The lens and the ocular media were clear. Fundus examination of right eye was within normal limit and in the left eye, an actively moving parasite was detected overlying the disk and the macula. (Fig.3) There was hemorrhage mostly on the superior, temporal, and nasal aspect of the disk that obscured some of the major vessels and the optic disk. The optic nerve head was edematous, and its margin was blurred. Intraocular pressure was normal. Findings of neurologic and dermatologic evaluations was not remarkable.
Results of laboratory investigations including determination of complete blood cell count and routine stool and urine examinations were within normal limits. The condition and treatment explained to the patient in detail. Standard three-port pars planavitrectomy was performed, and posterior vitreous detachment was induced. The intra- vitreal blood surrounding the parasite was aspirated. A 19-gauge cannula fitted with a flute needle was introduced into the vitreous cavity, and the parasite was gently aspirated into the cannula from its caudal end. Post operatively patient was advised topical atropine, steroid and antibiotic eye drops, as well as oral steroids.
Parasitologic Evaluation
Examination of a wet mount of the freshly removed parasite showed an advanced third-stage larva of G. spinigerum(aL3). Light microscopy revealed that the larva was constituted longitudinally into three regions (i.e., lips, head bulb, and body). (Fig.4)The parasite was fixed in a neutral buffered solution of 1% glutaraldehyde and 4% formaldehyde. The head bulb appeared globular and was easily distinguishable from the body. At the center of the head bulb, the mouth was located. The head bulb had four transverse rows of well developed single pointed hooklets or spine. (Fig.5)The body turned into encircle by 250 transverse rows of cuticles with minute body spines. The caudal end of the larva was blunt and round, with the anus opening subterminally. EDX spectroscopy of spine of Gnathostomiasis was done which showed positive spikes for sulphur, copper and calcium.
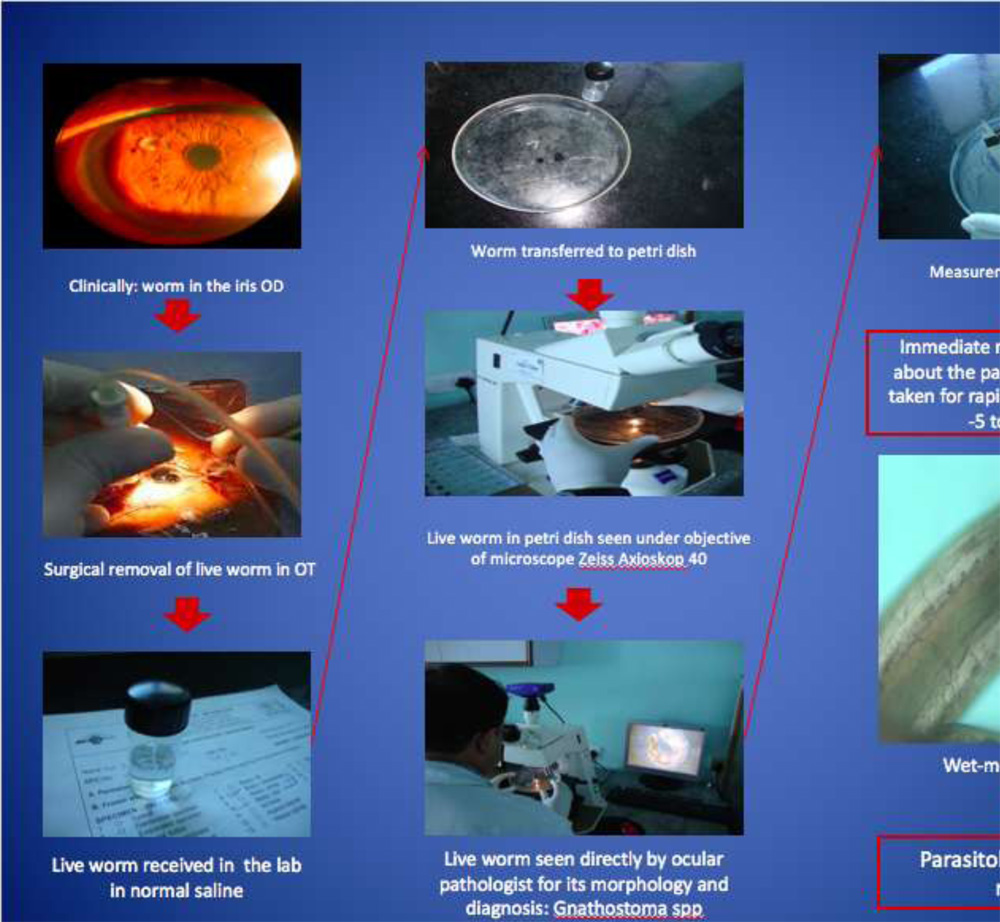
Novel rapid diagnosis algorithm for any intraocular parasite is as follows (Fig.6): Surgical removal of live worm, transfer of live worm in normal saline to laboratory, live worm in petri dish seen under objective microscope for its morphology and diagnosis, Immediate report to the surgeon about the parasite diagnosis. Time taken for rapid exercise- average 5 to 10 minutes.
Discussion
Human gnathostomiasis is usually prevailing in geographical area like Southeast Asia and Latin America,however there has been a progressive shift in its global frequency. Travel patterns, food habits, and fishing is also accountable for this world distribution.2,3 Clinical presentations in humans could be visceral and cutaneous, together with ocular involvement. Ocular gnathostomiasis is a rare clinical entity, and intravitrealgnathostomiasis is an even rarer condition. The anterior segment of the eye is the most common location of the parasite; of 19 reported cases worldwide, only 5 had intravitreal localization.4Ocular gnathostomiasis affects the eyelids, conjunctiva, cornea, anterior chamber, uvea, and vitreous cavity. The commonest ocular clinical manifestation is anterior uveitis.5However, lid edema, conjunctivalchemosis and orbital cellulitis, retinochoroidal and vitreous hemorrhage, and blindness may also be presenting features.
Consumption of smoked fish, a semicooked preparation, may have been the possible cause of infestation in our cases. In two of our patient’s intractable headache, which preceded ocular symptoms, could have been attributed to the intracranial larval migration after its passage through the common carotid, internal carotid, and ophthalmic arteries.
There is no established pharmacologic treatment of ocular gnathostomiasis. Mebendazole has been suggested as a potential therapeutic agent, but it is yet to be approved by the US Food and Drug Administration.6Therapeutic success relies upon early and complete surgical eradication of the parasite in the live form; otherwise, there may be ocular damage due to migration, and the severed parasite can cause serious intraocular inflammation.7,8Funata et al9and other researchers have recommended pars planavitrectomy and aspiration of the parasite out of the eye.
The larva of Gnathostomacan be identified from the number of rows and features of hooklets in the head bulb and can also be distinguished based on the number of nuclei in intestinal epithelial cells of infected larvae.9,10 Scanning electron microscopy improves the ability of distinguishing different species as well as staging.11Although five different species of Gnathostomaare known to cause human disease, G. spinigerumis the commonest species that affects the human eye. In the present case series, the species of the retrieved larva after surgical removal was identified based on light and electron microscopic features. In all the reported cases including ours, the intraocular parasite was in a living state. Our patients were followed up for 2 years. they maintained visual acuity of 6/6 with a normal fundus and was in perfect general health, indicating surgical removal of the parasite in the live form is a safe and effective modality of treatment.
Conclusion
Gnathostomiasis is a rare parasitic infestation of humans after intake of raw or undercooked meat or fish. This rapid diagnosis algorithm can help for early diagnosis and treatment of parasitic infection to prevent complications.
References
- Manson-Bahr PEC, Bell DR. Manson’s Tropical Disease. 19th ed. Appendix II. ELBS: London, Bailliere Tindal; 1987:1348–1350.
- Hunter JH, Rey L, Scott D. Man-made lakes—man-made disease. World Health Forum 1983;4:177–182.
- Kennedy CR, Hartvigsen R, Halvorsen O. The importance of fish, dissemination of parasite through a group of reservoirs.J Fish Biol. 1991;38:541–552.
- Bhattacharjee, H, Das D and Medhi J. Intravitrealgnathostomiasis and review of literature. Retina. 2007;27:67-73.
- Basak SK, Sinha TK, Bhattacharjee D, et al. Intravitreal live Gnathostoma Indian J Ophthalmol. 2004;52:57– 58.
- Drugs for the parasitic infections. Medical Lecture 1990;32:23–32.
- Bathrick ME, Mango CA, Mueller JF. Intraocular gnathostomiasis. Ophthalmol. 1981;88:1293–1295.
- Tudor RC, Blair E. Gnathostomaspinigerum and unusual causes of ocular nematodiasis in the Western hemisphere. Am J Ophthalmol. 1971;72:185–190.
- Funata M, Custis P, dela Cruz Z, et al. Intraocular gnathostomiasis. Retina 1993;13:240–244.
- Nomura Y, Nagakura K, Kagei N, et al. Gnathostomiasis possibly caused by Gnathostoma Tokai J Exp Clin Med. 2000;25:1–6.
- Maleewong W, Sithithaworn P, Tesana S, Morakote N. Scanning electron microscopy of the early third-stage larvae of Gnathostoma Southeast Asian J Trop Med Public Health. 1988;19:643–647.
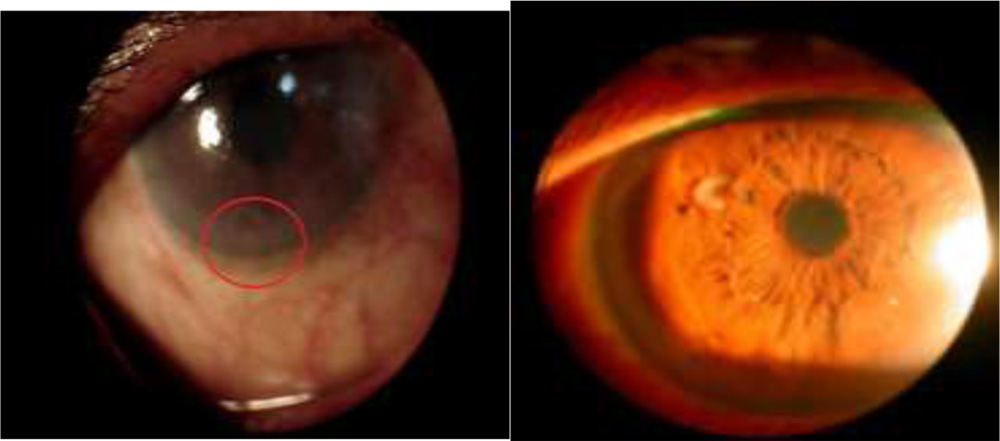
Figure 2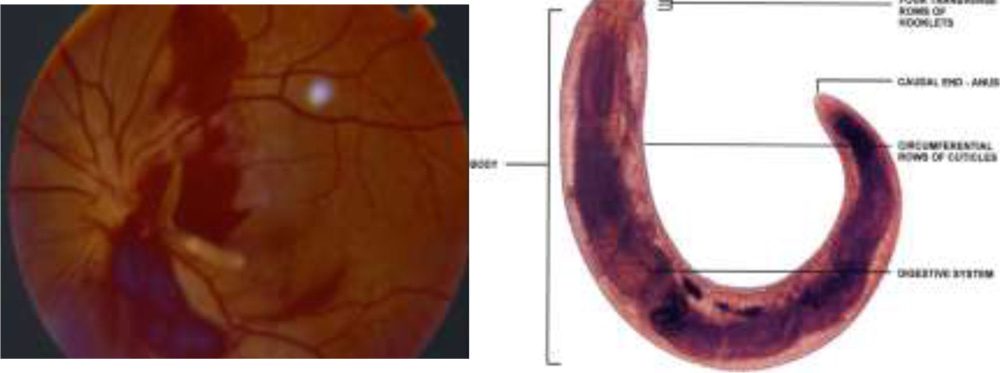 Figure .3 Figure 4
Figure .3 Figure 4 Figure 5
Figure 5