Dr. Madhuri. V. Thallam, M19307, Dr.M Shahid Alam, Dr. Swati Agarwal
Introduction:
Tuberculosis is a chronic granulomatous disease caused by Mycobacterium tuberculosis that can cause disease in many organs, including the eye. Ocular and adnexal tuberculosis can be primary or secondary to systemic involvement. Among ocular manifestations of tuberculosis, primary tuberculosis of eyelid is rather rare1
Various benign, malignant, inflammatory lesions of the eyelid can present clinically as a primary or recurrent chalazion, and pose diagnostic challenge to the clinician2. We report a rare case of eyelid tuberculosis presenting as recurrent chalazion in a female child, diagnosis of which was confirmed by histopathology and polymerase chain reaction.
Case report:
A 5 year old female child presented with a painless swelling of left lower eyelid for the last 5 months. Patient was diagnosed as chalazion elsewhere and was started on conservative treatment without any response. Parents also gave history of some minor surgical procedure done for the swelling details of which were not available. There was no history of ocular trauma or any significant systemic illness. Birth history was unremarkable with vaccination up to date. Her best corrected visual acuity was 20/30 in both eyes. Local Examination revealed single, firm, non-tender swelling in left lower eye lid of roughly 1X1 cm, with rough eczematous skin overlying it. There was mild surrounding erythemawithout any pus discharge or any pus point.
Rest of ocular surface, anterior segment and fundus examination were within normal limits. A clinical diagnosis of non-resolving chalazion was made and parents were advised to continue with conservative management for few more months.
However parents were apprehensive and were interested in surgical removal. Incision and curettage of the lesion was planned under General Anesthesia. A horizontal skin incision was given. The lesion was dissected out from the surrounding structure and underlying tarsus. There was no collection of inspissated material inside as routinely seen in cases of chalazion, instead there was lot of friable granulation tissue. Near complete removal of the lesion was done by carefully dissecting it from the overlying orbicularis and underlying tarsus, and it was sent for histopathology.
Histopathology revealed granulomas composed of epitheloid cells, histiocytes and langhans like giant cells with areas of necrosis and multiple lipid vacuoles surrounded by dense collections of mixed inflammatory cells. Polymerase chain reaction(PCR) targeting MPB64 gene and IS6110 region of Mycobacterium tuberculosis was done, of which MPB64 gene was positive. Patient was referred to an infectious disease specialist who started her on 9 month course of anti-tuberculosis (ATT) therapy, after ruling out any systemic involvement. Patient has completed her course of ATT and was contacted over phone. The patient was doing well without any recurrence. .
Discussion:
Eyelid tuberculosis generally starts as a non-tender eyelid swelling which progresses to become larger and nodular and finally ends up with formation of ulcerative lesions or fistula when the treatment is delayed3Associated features like low grade fever, raised ESR may give a clue to the diagnosis as reported in similar cases earlier4.
Tuberculosis involving the eyelid can mimic a chalazion when it presents as a firm nodular lesion. Study regarding accuracy of clinical diagnosis of chalazion revealed 6.4% clinically misdiagnosed cases which included 2.2% of chronic inflammatory lesions1
It is always challenging to diagnose ocular tuberculosis due to the lack of standard diagnostic criteria. This case report highlights the importance of histopathological examination and PCR in all curetted specimens of chalazion. Study regarding diagnosis of cutaneous tuberculosis recommends histopathology and isolation of the organism in culture or by PCR are principal diagnostic tools for diagnosis5. Histopathology gives us the typical histological appearance of tuberculosis lesions like caseous necrosis and PCR amplifies the DNA of the bacteria.
Once the diagnosis is made ophthalmologists and infectious disease specialist should work together to treat the patient with recommended doses appropriate for age and for adequate duration. Systemic investigations like chest x-ray should be ordered to rule out pulmonary tuberculosis which is more common. Follow-up is required in all cases on treatment to look out for side effects of ATT. Steroids may be necessary in cases of worsening of condition due to paradoxical reaction to standard regimen of ATT6.
References:
1.Ozdal PC, Codere F, Callejo S, et al. Accuracy of the clinical diagnosis of chalazion. Eye (Lond) 2004; 18: 135-8.
2.Mittal R, Tripathy D, Sharma S, Balne PK. Tuberculosis of eyelid presenting as a chalazion. J.ophtha. 2013; 5:1103.
3.Yang JW, Kim YD. A case of primary lid tuberculosis after upper lid blepharoplasty. Korean J Ophthalmol. 2004; 18: 190-5.
4.Agarwal R, Agarwal S. Isolated Right Upper Eyelid Tuberculosis: A Case Report with Review of the Literature. Journal of Clinical and Diagnostic Research. 2012; 6: 1068-1069.
5.Zhang LJ. Combination of laboratory diagnostic tests for cutaneous tuberculosis. Indian J Pathol Microbial. 2016; 59: 271-2
6.Seo Y, et al. A case of paradoxical reaction after treatment of eyelid tuberculosis. Korean J Ophthalmol.2014; 28: 493-5.
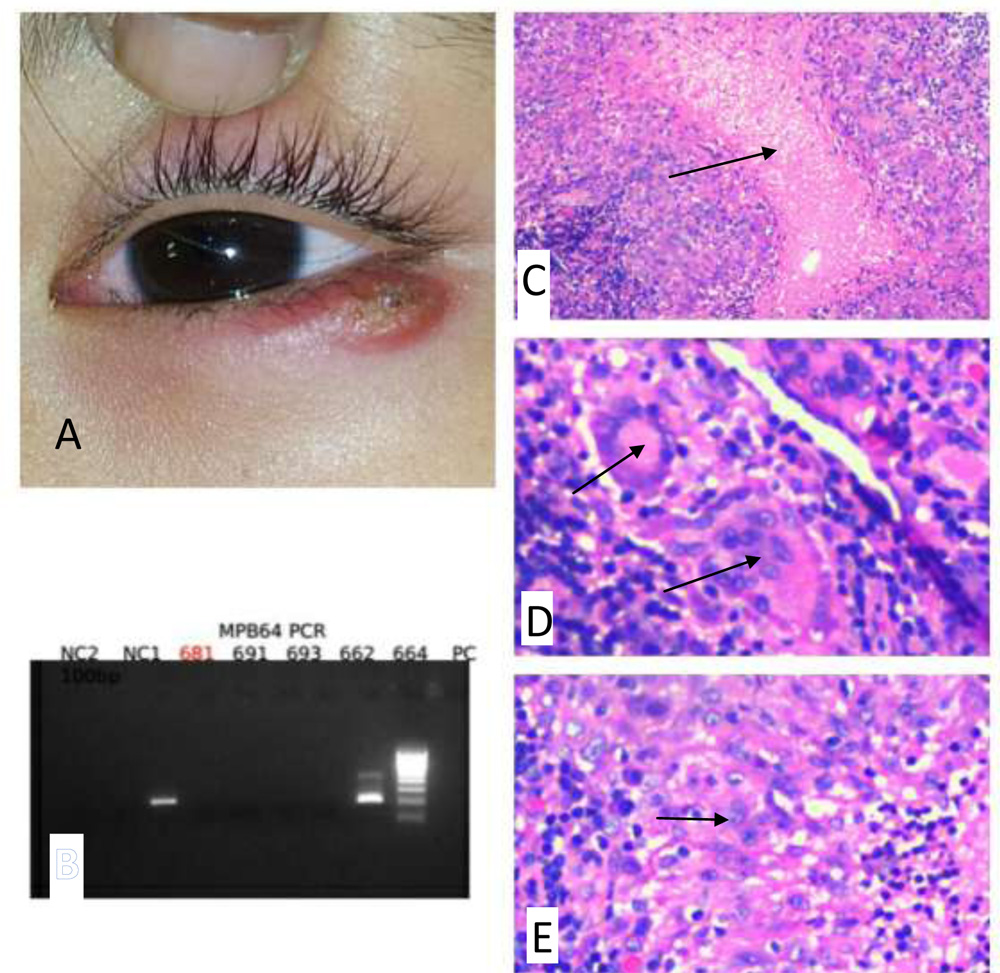
A. Clinical picture showing left lower lid swelling with erythema, B.PCR showing positive
for MPB64 gene, Histopathology: C. Necrosis, D. Giant cells, E. Epitheloid cells.