Dr.Anjali Kiran, K16753, Dr. Gupta Roshmi, Dr.Parvathi T Hari
RARE PRESENTATION OF PRIMARY SEBACEOUS GLAND CARCINOMA IN ORBIT
Running title: Primary sebaceous gland carcinoma in orbit
ABSTRACT
Background
- Orbit , Oculoplasty and Ocular Oncology Services, Narayana Nethralaya, Bangalore, India\
Purpose:
To report three cases of primary sebaceous carcinoma in the orbit.
Methods:
Three patients presented with orbital mass lesions. First and second cases were 30 and 31 years old men, with swelling in lacrimal sac area. The third case is of a recurrent swelling in lacrimal gland area in a 54 year old male with history of excision of pleomorphic adenoma 25 years ago. CT scan showed heterogeneous enhancing mass with posterior extension in medial orbit in first two cases and a mass in lacrimal gland area, extending into intraconal space in third case. First case underwent incisional biopsy while excision was done for others.
Results:
All patients had poorly differentiated sebaceous carcinoma, confirmed by Immunohistochemistry. Additional radiotherapy was done in two patients.
Conclusion:
sebaceous gland carcinoma arising from meibomian glands, can rarely present in orbital tissues. This is the first report of the lesion within the inferiomedial orbit and lacrimal sac
Authors:
Dr ANJALI KIRAN 1
Dr PARVATHI HARI 1
Dr ROSHMI GUPTA 1
- Orbit , Oculoplasty and Ocular Oncology Services, Narayana Nethralaya, Bangalore, India
Corresponding author:
Dr ROSHMI GUPTA,
Orbit, Oculoplasty and Ocular Oncology Services,
Narayana Nethralaya
121/C, Chord Road, Rajajinagar,
Bangalore 560010
Phone: +91 900768037
INTRODUCTION
Sebaceous gland carcinoma (SGC) commonly arises from periocular tissues due to the abundance of sebaceous glands. The most common periocular tissues are meibomian glands, glands of Zeiss, glands of eyebrows, the caruncle and glands from the facial cutaneous surface. The hallmark of SGC is its tendency to masquerade as benign or malignant lesions, leading to a delay in diagnosis, unfavorable prognosis and increased mortality. Involvement of the orbit is commonly as secondary invasion form the eyelid or metastasis from elsewhere in the body. Primary sebaceous gland arising in the orbit is rare. Literature search shows only a few isolated primary orbital cases. We present three cases of primary SGC in the orbit- one from the lacrimal gland and other two from inferiomedial orbit.
CASE REPORT
CASE 1
A 30 year old gentleman was seen with left eye pain since 3 days and persistence of swelling following lacrimal sac surgery done 25 days elsewhere. On examination he had he had scar and induration in lacrimal sac area. With the history of recent lacrimal sac surgery suspecting infection oral antibiotics and analgesics were prescribed and asked for review after 1 week. On follow up pain had reduced, but swelling persisted. Syringing through both punctum was patent; hence an organizing hematoma or inflammation was thought of and asked to review again after 1 week with suggestion of hot fomentation. Patient reviewed with complaints of blurring of vision. On examination the swelling was more firm. An imaging and ENT opinion was sought. The CT orbit showed heterogeneous enhancing mass in the inferior medial orbit, eroding into inferior meatus. After consultation with the ENT surgeon an open incisional biopsy was done. The histopathology suggested poorly differentiated sebaceous carcinoma. Patient preferred referral to an oncologist in a different city. Under his care he received 2 cycles of neoadjuvant chemotherapy followed by medial orbitotomy with excision biopsy and dacryocystectomy along with excision of nasolacrimal duct. The surgery was followed by with stereotactic EBRT. The patient is on follow up with the oncologist.
CASE 2
A 31 year old gentleman was seen with complaints of left eye watering since 15 days. He had OS swelling without pain since 1 year, with increase in the swelling since 2 months. On examination he had mass palpable above and below medial canthal tendon with telecanthus. Syringing 1 month prior, done elsewhere, had been patent as per the patient. On current visit syringing was not patent. CT orbit showed homogenous mass from lacrimal sac area extending into extraconal medial orbit, scalloping the bone suggesting mass of long duration. Patient underwent excision biopsy. The mass was well circumscribed without adhesions encompassing the sac; hence the sac had to be removed. Mass was removed in toto. Histopathology was suggestive of sebaceous carcinoma. A second histopathology and Immunohistochemistry confirmed as sebaceous carcinoma. A systemic work up and referral to oncology team we work with was planned for adjuvant chemotherapy/radiation. PET scan was done did not show any hot spots anywhere in the body/orbit. The patient went to a surgical oncologist of his choice. Despite telephonic communication, no intervention was done from the oncologist. Patient is lost to follow up.
CASE 3
A 50 year old gentleman was seen with right eye swelling and pain since 1 year. The patient had undergone surgery 17 years back for lacrimal gland. It was then diagnosed as pleomorphic adenoma as documented from the discharge summary and HPE report. On examination he had 5mm proptosis, inferior dystopia and palpable lacrimal gland. Vision and IOP were within normal limits. Limitation in adduction and abduction were noted. He also had diplopia in left gaze. Following imaging he underwent orbitotomy with excision biopsy. The histopathology reported with a differential diagnosis of sebaceous carcinoma and pleomorphic adenocarcinoma. Immunohistochemistry excluded primary minor salivary gland- Acinic cell and Oncocytic carcinoma. An overlap between primary adnexal-eccrine mucinous carcinoma and sebaceous carcinoma was reported. But retention of MSH2 nuclear staining and ER negative favoured the diagnosis of sebaceous carcinoma. Plan was to refer to an oncologist for adjuvant chemotherapy/ radiation. But the patient did not meet the oncologist. He came back after 7 mths with complaints of headache and recurrence of mass. He has been advised imaging to rule out intracranial extension. The patient is yet to review with the imaging films.
DISCUSSION
All the three cases presented with mass lesions in the orbit without any obvious involvement or history of eyelid or conjunctival lesions. PET scan and systemic examination did not reveal any systemic involvement. Second opinion on histopathology and Immunohistochemistry was done to confirm the diagnosis of SGC.
Primary SGC of the lacrimal gland is very rare with less than 10 cases reported worldwide. Shibata M et al reported of SGC in an anophthalmic socket of 65 years hypothesised due to chronic irritation from a poorly fitted ocular prosthesis. Kiratli et al reported of SGC of lacrimal gland which presented with metastatic parotid gland mass. Briscoe et all have suggested on the presence of heterotopic sebaceous tissue in the lacrimal gland as a possibility of primary lacrimal gland SGC.
Rath S et all have reported of a recurrence of SGC in the lacrimal sac, 5 years following successful wide margin excision of SGC of lid with uninvolved margins.
References
1 Shibata M, Usui Y, Ueda S, Matsumura H, Nagao T, Goto H. A case of orbitalsebaceous gland carcinoma developing in an anophthalmic socket 65 years afterenucleation. Clin Ophthalmol. 2013;7:1825-7. doi: 10.2147/OPTH.S44639.
2.Kiratli H, Tarlan B, Fırat P. Primary sebaceous carcinoma of the lacrimalgland. Orbit. 2012 Oct;31(5):352-4. doi: 10.3109/01676830.2012.678921.
3. Rath S, Honavar SG, Reddy VA, Naik MN, Vemuganti GK, Murthy R. Sebaceouscarcinoma of the eyelid metastasizing to the lacrimal sac after 5 years. Orbit.2009;28(5):309-12
4. Briscoe D,Bonshek SMR,Jackson A,Leatherbarrow A. Primary sebaceous carcinoma of the lacrimal gland.Br J ophthalmol 2001;85:625-633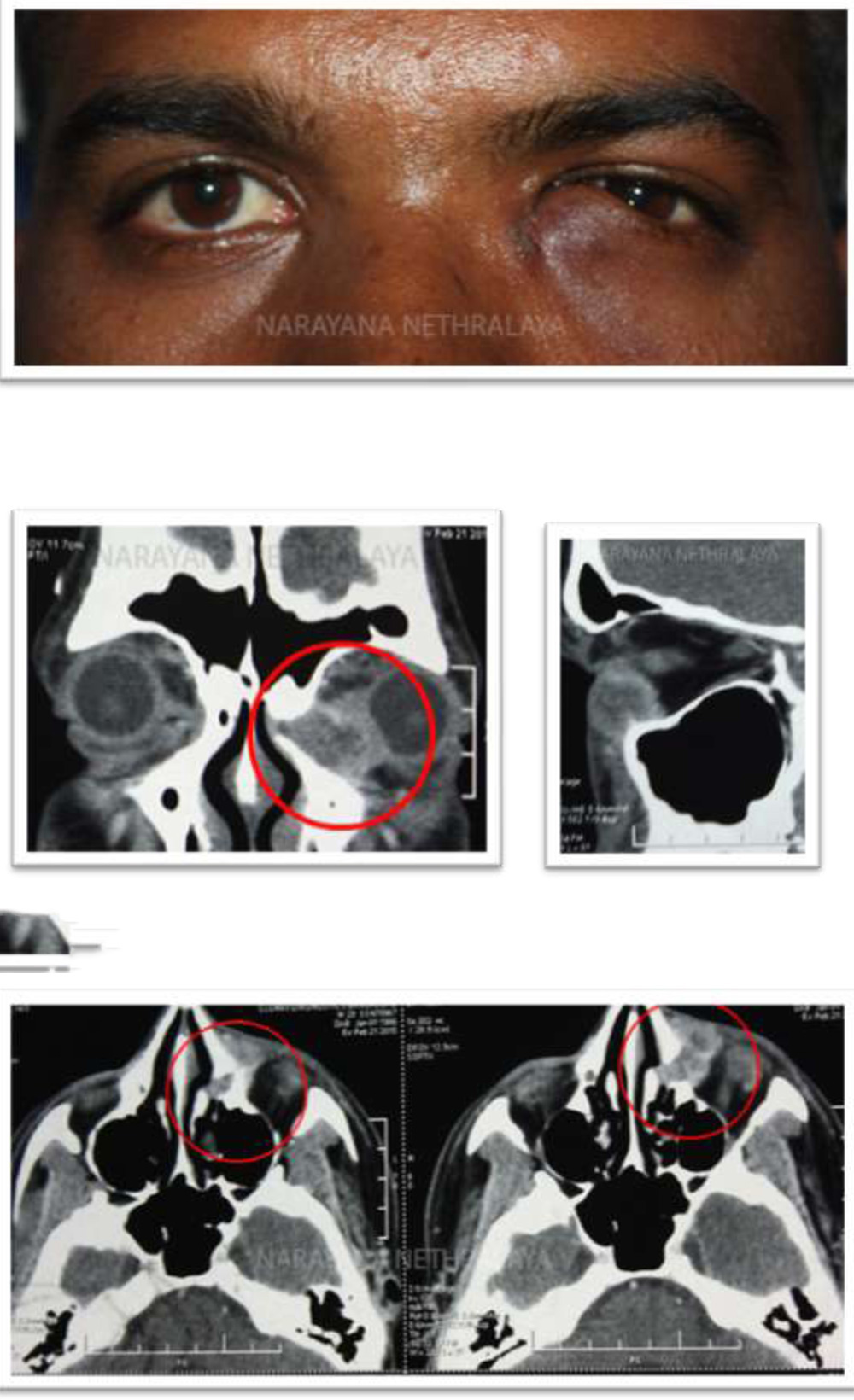

LEGENDS :
Figure 1:
Clinical photograph showing scar and induration in lacrimal sac area.
Figure 2,3,4:
Computerized Tomography of orbit showing heterogenous enhancing mass in left inferiomedial orbit, eroding into inferior meatus. Coronal , sagittal and axial sections respectively.
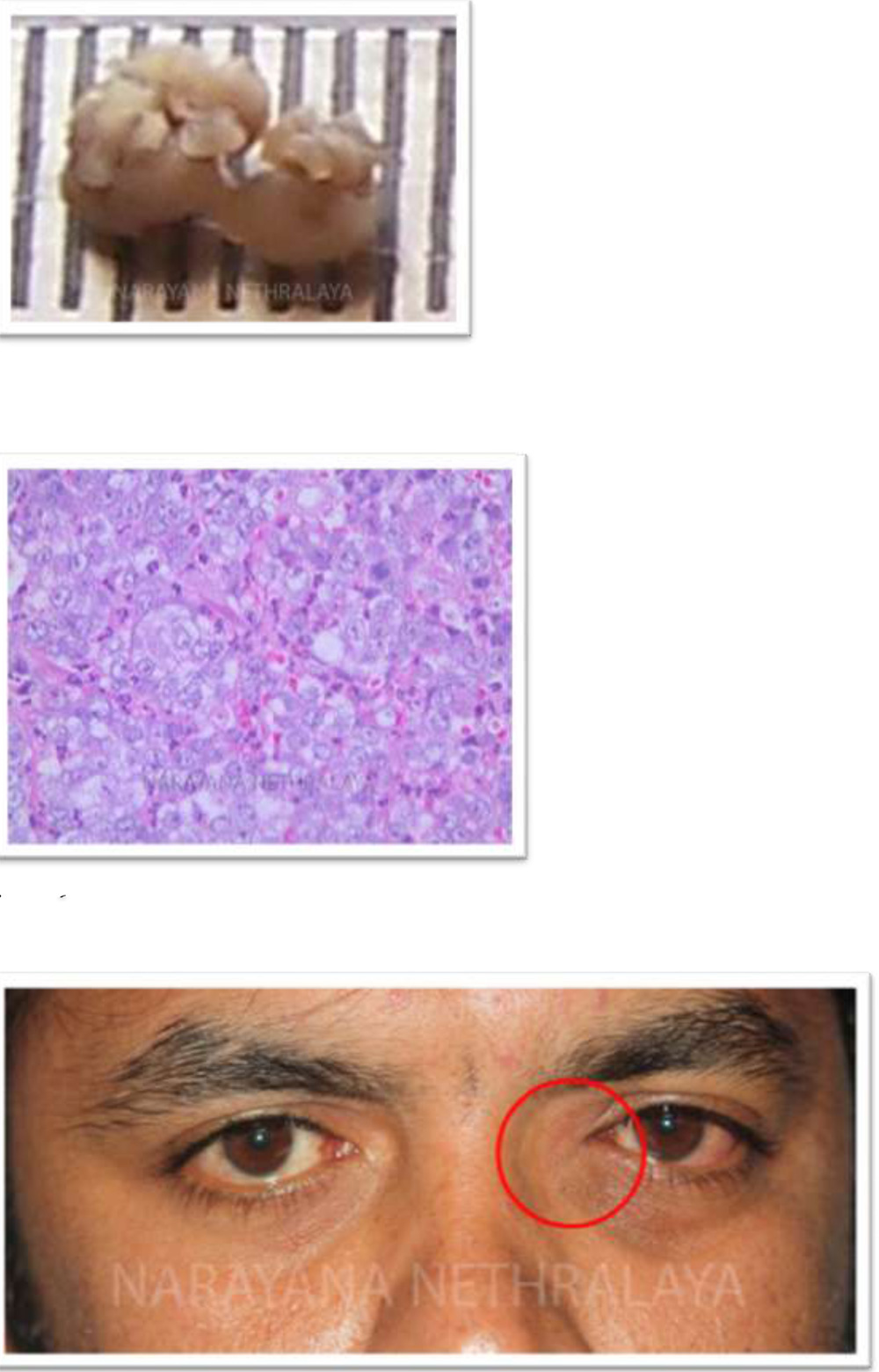
Figure 5:
Histopathology :Shows incised mass
Figure 6:
Histopathology : Photomicrograph showing infiltrating malignant tumor. Large cells with foamy cytoplasm. Poorly differentiated sebaceous gland carcinoma.
Figure 7:
Clinical photograph showing mass above and below medial canthal tendon. Telecanthus can also be noted.
Figure 8,9:
Computerized tomography of orbit shows homogenous mass from sac area, extending into extraconal medial orbit scalloping the bone. Coronal and axial sections respectively.
Figure 10:
Histopathology shows excised well circumscribed mass, removed in toto.
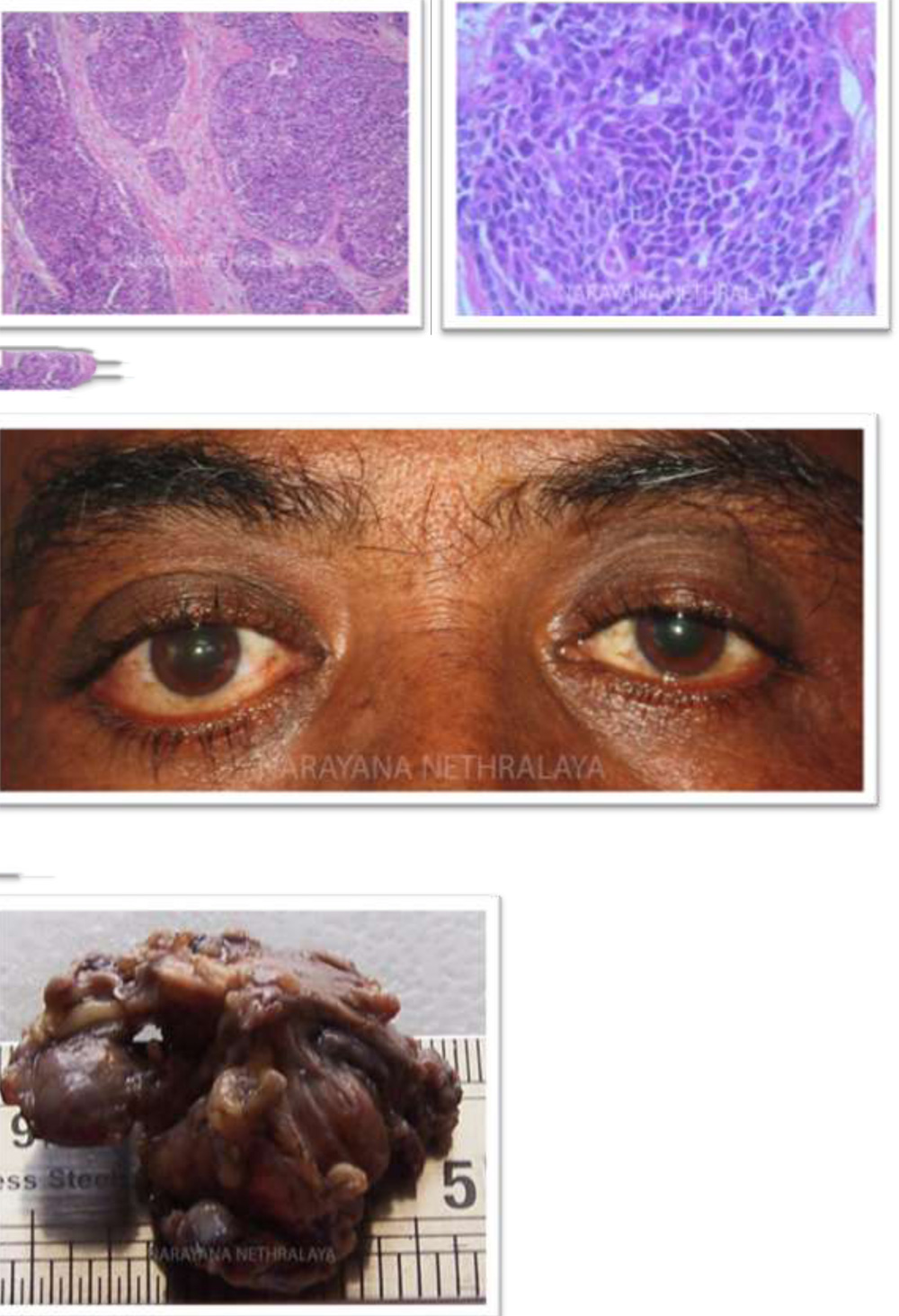
Figure 11,12:
Histopathology : Photomicrograph showing tumor cells arranged in lobular pattern with intervening fibrovascular septa.
Figure 13:
Clinical photograph showing OD dystopia
Figure 14:
Histopathology : Showing mass excised
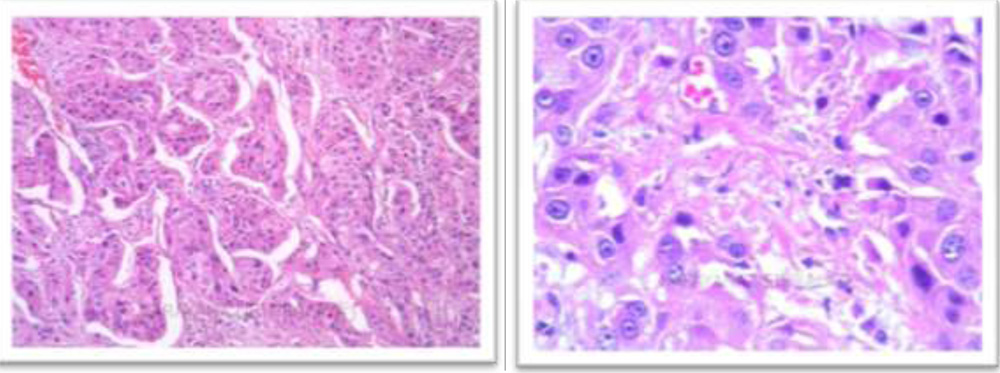
Figure 15,16:Histopathology : Photomicrographs shows tumor cells arranged in groups , cords and trabeculae. Large polygonal cells with pale to granular cytoplasm, round vesicular nuclei with prominent nucleoli.