Dr. Mekhla Naik, N18166, Dr. Marian Anne Jacob, Dr. S. Krishnakumar, Dr. Giridhar Anantharaman
Abstract
Intratarsal keratinous cyst(ITKC) is the third common cause of tarsal swelling after chalazion &sebaceous cell carcinoma. We report a solitary series of six cases of ITKC from India with mean age of52.67±13.02yrs presenting with non-inflamed eyelid nodule sized 1-14mm in diameter. The cysts appeared as solid, whitish opalescent or yellow-white, subcutaneous nodules fixed to the tarsus. The embedded tarsal cysts weresurgically excised completely along with a portion of underlying tarsus, through a lid crease incision. Histopathological evaluation revealed stratified squamous epithelium linings & keratin contentswithin the lumen in all specimen. No recurrence occurred in all patients.Our series highlights clinical & pathological characteristics of ITKC, including absence of inflammatory signs withcharacteristic embedment intothe tarsus. A complete excision of cysts with partial tarsectomy by transcutaneous approach was proved to be an effective treatment for prevention of recurrence.
Introduction
The most common cause of lid swellings includes chalazia & sebaceous gland carcinomas1.Other causes of lid swelling have not been studied as extensively as the fore mentioned ones1. However this newly emerging entity namely Intratarsal Keratinous Cyst (ITKC), seems to be the third most common cause of lid mass1. The diagnosis of this new entity is important as incomplete excision leads to recurrences1,2. Confirmationis done by histopathological examination2. Histopathology shows the presence of stratified squamous epithelium in the walls & keratin content in the lumen, which is different from that found in the epidermal / epidermoid cyst1,2,3,4.The entity shows a negative reaction with Alcian Blue & Periodic acid Schiff stains & a positive immunochemical reaction with epithelial membrane antigen2.
In our current case series, we analyze the clinical and histopathologic features and surgical outcomeof intratarsal keratinous cyst (ITKC) in a series of six patients from South India.
Materials and Methods
It was a retrospective, interventional and clinicopathologic study of six patients presenting with Intratarsal keratinous cyst (ITKC), carried out at Department of Orbit and Oculoplasty,Kerala, India, between August 2013 to May 2016.The clinical history of the patients including history of previous surgery and recurrences was reviewed along with the slit lamp findings. All cases were operated by a single surgeon through a lid crease incision and included a partial tarsectomy. The excised specimens were sent for histopathological evaluation
Results
Six patients with an average age of 52.67±13.02 years hadupper eyelid cysts ranging from 1-14 mm in diameter. The duration of the symptoms ranged from 1-20 years. However, in two patients the duration was unknown. All patients presented with slow growing, non-tender upper lid mass. One patient additionally presented with symptoms of ghost images associated with increase in size of the mass. The cysts presentedas solid subcutaneous nodules fixed to the tarsus mostly with whitish or yellowish-white hues. The overlying skin was freely mobile over the lesion. On eversion, no signs of inflammation were seen on the tarsal surface. One cyst revealed a bluish discoloration on the tarsal side.
Fig 1: showing a 10 x 10 mm cystic lesion with the overlying skin stretched. The skin is freely mobile & an old scar is seen.
 Fig 2A: showing a non inflamed mass on the cutaneous aspect of the right upper lid; Fig
Fig 2A: showing a non inflamed mass on the cutaneous aspect of the right upper lid; Fig
2B: showing the same mass with bluish discolouration on the tarsal surface  The cysts embedded in the tarsus were completely excised with a portion of the underlying tarsus by a surgical procedure through a lid crease incision. One of the cysts ruptured intraoperatively releasing a milky fluid4 as opposed to the routine cheesy secretions found in dermoid cysts or the yellowish-white gelatinous contents of epidermal cyst3.
The cysts embedded in the tarsus were completely excised with a portion of the underlying tarsus by a surgical procedure through a lid crease incision. One of the cysts ruptured intraoperatively releasing a milky fluid4 as opposed to the routine cheesy secretions found in dermoid cysts or the yellowish-white gelatinous contents of epidermal cyst3.
Fig 3: showing the cyst attached to the tarsus intraoperatively

Fig 4A: showing another patient with a cyst on the left upper eyelid;Fig 4B: same patient showing ruptured cyst discharging milky white fluid intraoperatively
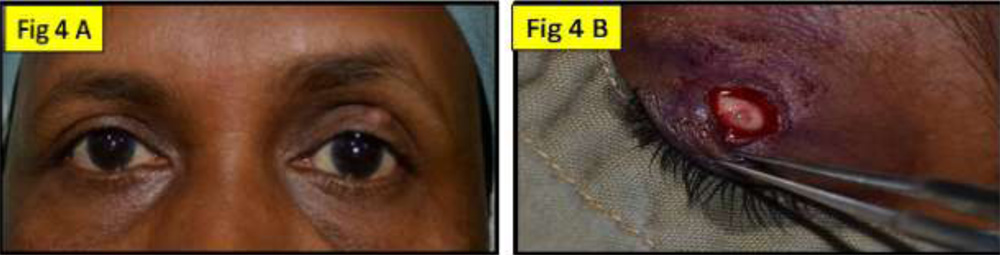 Fig 5A: showing intraoperatively the lid crease incision, the excised cyst & the resulting eyelid defect; Fig 5B: same patient showing the full thickness from the tarsal aspect
Fig 5A: showing intraoperatively the lid crease incision, the excised cyst & the resulting eyelid defect; Fig 5B: same patient showing the full thickness from the tarsal aspect 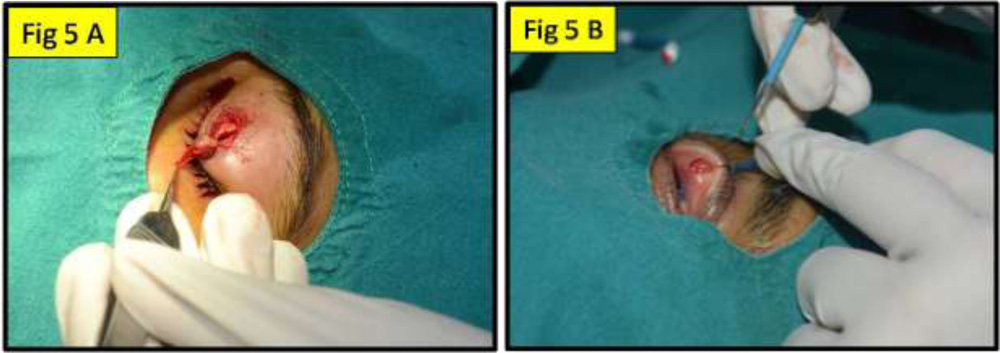 Fig 6: showing an excised specimen (cyst)
Fig 6: showing an excised specimen (cyst)
Histopathologic evaluations of all the specimens revealed stratified squamous epithelium linings along with a distinct cuticle lining the lumen and keratin contents. Hair structures were found in the dermis portion of one of the specimens but none within the cysts or the walls.
Fig 7: original magnification 4x, histopathology (hematoxilin & eosin) of the cyst showing 1. Eosinophilic undulating cuticle 2. Lamellate keratin 3. Multilayered squamous epithelium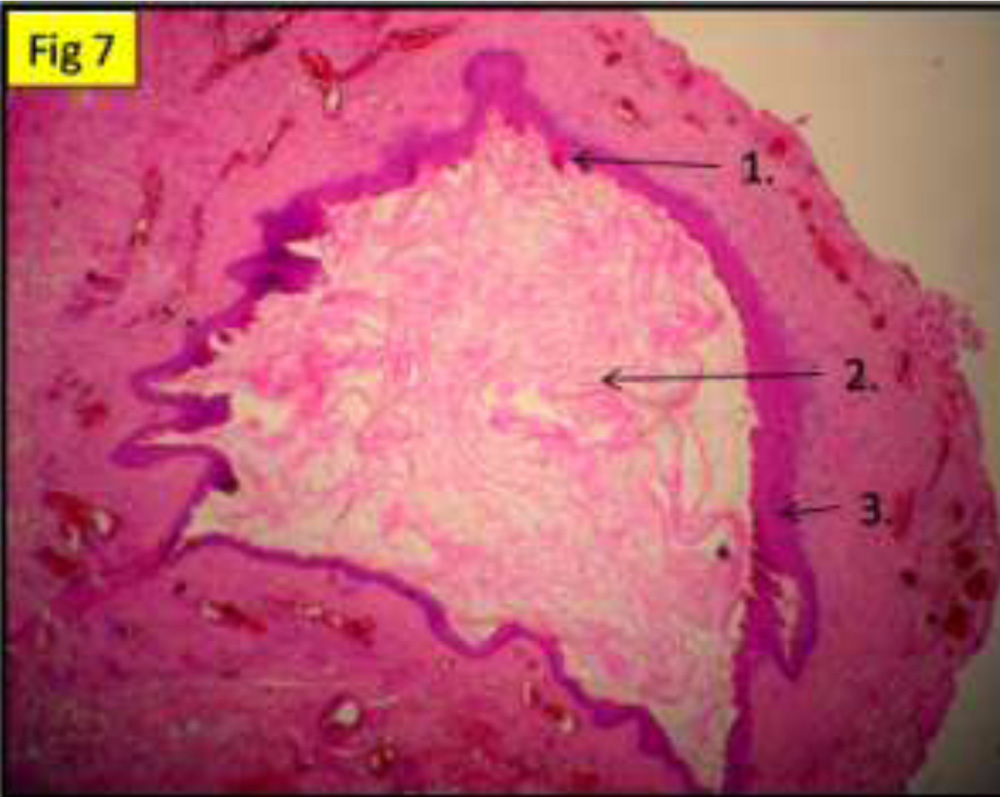
Table 1: showing the details & histopathology of all the patients
| Sr no | Age | Sex | Duration | Eye | Prev sx | Presence of keratin in lumen | Cyst wall layers | Type of epithelium | Hair structures | Date of reporting |
| 1 | 68 | F | Not mentioned | OD | No | + | ML | SS | No | 26/11/15 |
| 2 | 38 | F | 1 | OS | No | + | ML | SS | No | 06/12/15 |
| 3 | 65 | M | Not mentioned | OS | No | + | ML | SS | No | 06/04/15 |
| 4 | 59 | M | 3 | OS | No | + | ML | SS | No | 14/11/14 |
| 5 | 46 | M | 3 | OD | No | + | ML | SS | No | 12/08/13 |
| 6 | 40 | F | 20 | OS | Yes | + | ML | SS | In dermis | 10/5/16 |
| F = female; M = male; ML = multilayered; SS = stratified squamous epithelium | ||||||||||
Follow up:All the patients have been followed up routinely. No recurrence has been noted in the patients till date. The single patient complaining of ghost images has been symptomatically relieved post operatively.
Discussion
Jakobiecet al named the cyst as INTRATARSAL KERATINOUS CYST OF THE MEIBOMIAN GLAND1. It arises from the sebaceous lobule duct1. The characteristic clinical and histopathological features include freely mobile skin over the lesion, absence of inflammatory features, extension to conjunctival aspect, fibrous wall without sebaceous lobules, keratinizingsquamous epithelium without granular layer and transformation of lining cells to eosinophilic undulating cuticle1,2,5,6.Expression of cytokeratin (CK) in the lining epithelium of the cyst wall is a specific marker for ITKC1,6.
These cysts normally occur singly but Kim et al have reported a solitary case with 11 cysts in a single eyelid7
The most common differential diagnosis3,5 include:
1) Chalazion whose histopathology reveals epithelioid, histiocytes and inflammatory giant cells surrounding lipid vacuoles.
2) Steatocystoma, which is lined by nonkeratinising squamous epithelium with keratohyaline granules and the walls,contain sebaceous gland. The cyst contains pale staining flocculent material.
3) Dermoid Cysts are attached to the superior pole of tarsus but are extrinsic to the tarsus. Histopathology shows keratinising squamous epithelium with keratohyaline granular layer and pilosebaceous units in the walls.
4) Epidermal cysts arise from dermis and are freely mobile with a prominent granular layer.
5) Intratarsal Pilomatrixoma.
6)Intratarsal cysticercosis
Management:
- Full thickness eyelid resection in small lesions
- Dissection of the extratarsal part with partial tarsectomy and cauterisation of the edges in large lesions
Conclusion
Our study revealed the clinical and pathological characteristics of ITKC, including the absence of inflammatory signs, lesion partially embedded in the tarsus1,2,4. Always maintain high index of suspicion in patients with non-inflamed atypical upper lid cyst of long standing duration with prominence on cutaneous aspect as well as conjunctival aspect2,4. Also they need an aggressive initial management as complete excision of cysts via a transconjunctival2 or a transcutaneous5 approach with partial tarsectomy was proved to be an effective treatment for prevention of recurrence1,2,4,6,7.
References:
- Jakobiec FA, Mehta M, Iwamoto M et al.Intratarsal keratinous cysts of the meibomian gland: distinctive clinicopathologic and immunohistochemical features in 6casesAm J Ophthalmol. 2010 Jan;149(1):82-94.
- Zhang ZD, Li X, Li M et al. Clinicopathological features and surgical treatment ofintratarsal keratinous cysts. Am J Dermatopathol. 2013 Feb;35(1):78-82
- Lucarelli MJ, Ahn HB, Kulkarni AD et al. Intratarsal epidermal inclusion cyst. OphthalPlastReconstr Surg. 2008 Sep-Oct;24(5):357-9.
- Kim JA, Kim N, Choung HK, Lee MJ, Lee C, Khwarg SI. Clinical features of intratarsal keratinous cysts. Eye (Lond).2016 Jan;30(1):59-63.
- Patel VS, Meyer DR, Carlson JA. Intratarsal keratinous cysts of the meibomian gland (a sebaceous duct cyst): report of 2 cases. Am J Dermatopathol.2011 Aug;33(6):624-7.
- Rajaii F, Ghafourian A, Eberhart CG. Intratarsal keratinous cyst – an emerging entity. Case Rep Ophthalmol.2013 Oct 5;4(3):160-4.
- Kim HJ, Wojno TH, Grossniklaus HE. Multiple intratarsal keratinous cysts of the eyelid. Ophthal Plast Reconstr Surg.2012 Sep-Oct;28(5):e116.