Dr. Shreeshruthi N, N18565, Dr. D.N. Parkash, Dr. Rohini Chalekar, Dr. Asma M K, Dr. Gajaraj T Naik
Chief author
Dr. D.N.PRAKASH
Associate Professor
Dept. of Ophthalmology
MMC&RI, Mysore
bhanup7@yahoo.com
Presenting author
Dr. SHREESHRUTHI N
Postgraduate student
Dept. of Ophthalmology
MMC&RI, Mysore
shruthishree.13@gmail.com
Co-authors
Dr. ROHINI CHALEKAR
Dr. ASMA M K
Dr. GAJARAJ T NAIK
Post graduate students
MMC&RI
Mysore
Abstract
Purpose
The purpose of this research work is to study the outcome of primary autologous dermis fat graft following evisceration and enucleation in terms of orbital volume replacement and feasibility of prosthesis fitting.
Materials and method
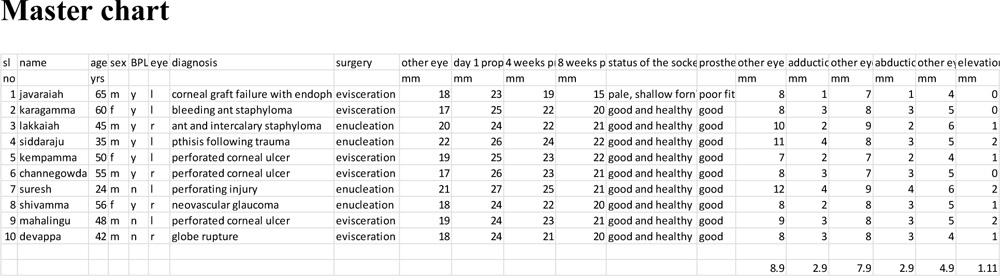
Study conducted on 10 patients undergoing evisceration and enucleation for various reasons who underwent dermis fat graft as a primary procedure. Graft was taken from the gluteal region. Post-operative orbital volume replacement was evaluated by luedde’sexophthalmometer,observing the deepening of the fornicesand by prosthesis stability.
Result
Good orbital volume replacement noted in all patients on post-op day 1(mean 25mm), 4 weeks(mean 23mm), 8 weeks(21mm). One of the patients had graft necrosis. Prosthesis fit was stable due to deepened fornices.
Conclusion
Dermis fat grafting as a primary procedure in patients undergoing evisceration and enucleation is cosmetically better with good orbital volume replacement and stable prosthesis fitting with good motility.
Key words: dermis fat graft, orbital volume replacement, orbital implants
Introduction and purpose of the study
The anophthalmic socket is always a blemish to a person who has had an enucleation/evisceration. Over the years the empty orbit develops a progressive sunken appearance. The cosmetic disfigurements which arise after enucleation of an eye include enophthalmos, retraction of the upper eyelid, deepening of the superior sulcus, backward tilt of the prosthesis, and stretching of the lower eyelid. These findings, summarised in ‘the post-enucleation socket syndrome’1, may arise separately or in combination and may vary in severity. This has been felt to be due to degeneration of the inactive extraocular muscles, orbital fat atrophy, and the tendency for normal senile enophthalmos. To regain a normal appearance after the enucleation they should be prevented and/or treated. This is best accomplished by substitution of the orbital volume loss (6-7 ml) with an adequate intra- orbital implant.
Proper implant sizing is crucial. Implant that provides about 65-70% of volume replacement is ideal, the remaining 35-30% being contributed by the prosthesis. Over the last decade various types of orbital implants have been developed like non-integrated, bio-integrated and biogenic2
Smith and Petrelli3 first described the use of autogenous dermis fat grafts as a secondary implant following extrusion of the primary implant. As a primary implant, the use of dermis fat graft has been described following ocular enucleation and evisceration.4Despite the success of alloplastic implants, autogenous graft as an orbital implant should not be discounted, as complications arising from alloplastic implants such as exposure and extrusion have been reported. In particular, exposure rates of porous implants after evisceration and enucleation range from 2 to 10%.5,6
Being autologous, it has neither the risk of rejection nor transfer of infection from cadaveric homologous tissue.
The purpose of this research work is to study the outcome of primary autologous dermis fat graft following evisceration and enucleation in terms of orbital volume replacement and feasibility of prosthesis fitting.
Objectives of the study
To study the following aspects in patients undergoing primary autologous dermis fat graft following evisceration
- Orbital volume replacement
- Feasibility of prosthesis fitting
Source of data collection
Patients attending out-patient and in-patient department, department of ophthalmology, K R Hospital, Mysore, requiring evisceration for various reasonswho fulfill the inclusion and exclusion criteria.
Method of data collection
Sample size: 10
Study type: prospective study
Inclusion criteria
All the subjects undergoing evisceration and enucleation for various reasons (with dermis fat graft as a primary procedure)
Exclusion criteria:
- Old and debilitated
- Subjects less than sixteen years of age
Materials and methods
A total of 10 patients presenting to the out-patient department of ophthalmology, K R Hospital, Mysore, requiring evisceration and enucleation for various reasons were enrolled in the study. Old and debilitated patients, and those under 16 years of age were excluded. A detailed history was taken. Anterior segment was examined usingslitlamp. Ophthalmoscopic examination, proptometry, tonometry were done wherever necessary. Examination also included assessment of general health, routine blood tests (blood sugar, haemoglobin, total and differential leucocyte count) blood pressure, and electrocardiogram. CT-scan/MRI was advisedwherever necessary. Patients were taken for either eviscerstion or enucleation depending on the condition of the eye. This was followed by dermis fat grafting. Graft was taken from the gluteal region.
Procedure of evisceration
360⁰peritomy done. Corneal button removed. Intra-ocular contents scooped out. Frill evisceration done leaving behind 3mm of the sclera at the optic nerve head.
Procedure of enucleation
360⁰peritomy done. All the 6 extra-ocular muscles were identified, secured and disinserted. Optic nerve cut and the eyeball removed.
Harvesting dermis fat graft
Donor site i.e. upper outer quadrant of the left gluteal region was prepared aseptically and an oval shaped margin marked with predetermined measurements from the eye socket after enucleation, making provision for an extra 2 millimetres for anticipated shrinkage when tissue is transplanted. The junction between the epidermis and dermis was infiltrated locally with normal saline mixed with Adrenalin 1 in 10000 injections.
The epidermis over the marked out site was shaved off with No. 22 surgical blade. The underlying dermis with fat was then excised using No. 11 blade, elliptically shaped to fit the orbital socket (18 –20mm in longest diameter, 14-16 mm in width and about 4–6mm in depth) and placed in saline solution. The wound at the donor site was then closed with interrupted sutures using 2/0 Vicryl suture and dressed with betadine ointment.
DFG implantation
The DFG was implanted into the posterior tenon’s space. Secured extra-ocular muscles (in those cases following enucleation) and conjunctiva was then sutured to the edge of DFG separated from anterior tenon’s with 6/0 Vicryl suture in an interrupted fashion.
Post-operative
Post operatively; the eyes were treated with combined antibiotic/corticosteroid ointment q.i.d for a month. Ocular prosthesis (thin shelled) was fitted after 4 weeks. Patients were followed up till 8 week.
Outcome measures
Orbital volume replacement by proptometry and deepening of the fornices by stability of prosthsis fit were analysed. Motility of the prosthetic eye in extreme directions of gaze was measured using a plastic ruler. Temporal limbus a marker for adduction, nasal limbus for abduction, and inferior limbus for elevation. Depression could not be assessed accurately as upper eyelid covers the eye in down-gaze.
Results
Prospective study, on 10 patients who underwent evisceration/enucleation with primary dermis fat grafting.Statistical analysis done using SPSS software version 22. Frequency tables, T-tests were used.
Study included 3 female and 7 male patients between 24 and 65 years of age.
Table 1 Sex distribution in the study
| Sex of the patients | Frequency | Percent | |
| Valid | female | 3 | 30.0 |
| male | 7 | 70.0 | |
| Total | 10 | 100.0 | |
7 patients underwent evisceration and 3 enucleation. Indications were perforated corneal ulcer in 3, globe disfigurement due to trauma in 3, anterior staphyloma in 2,painful blind eye due to neovascular glaucoma in 1, and failed corneal graft with endophthalmitis in one of the patients.
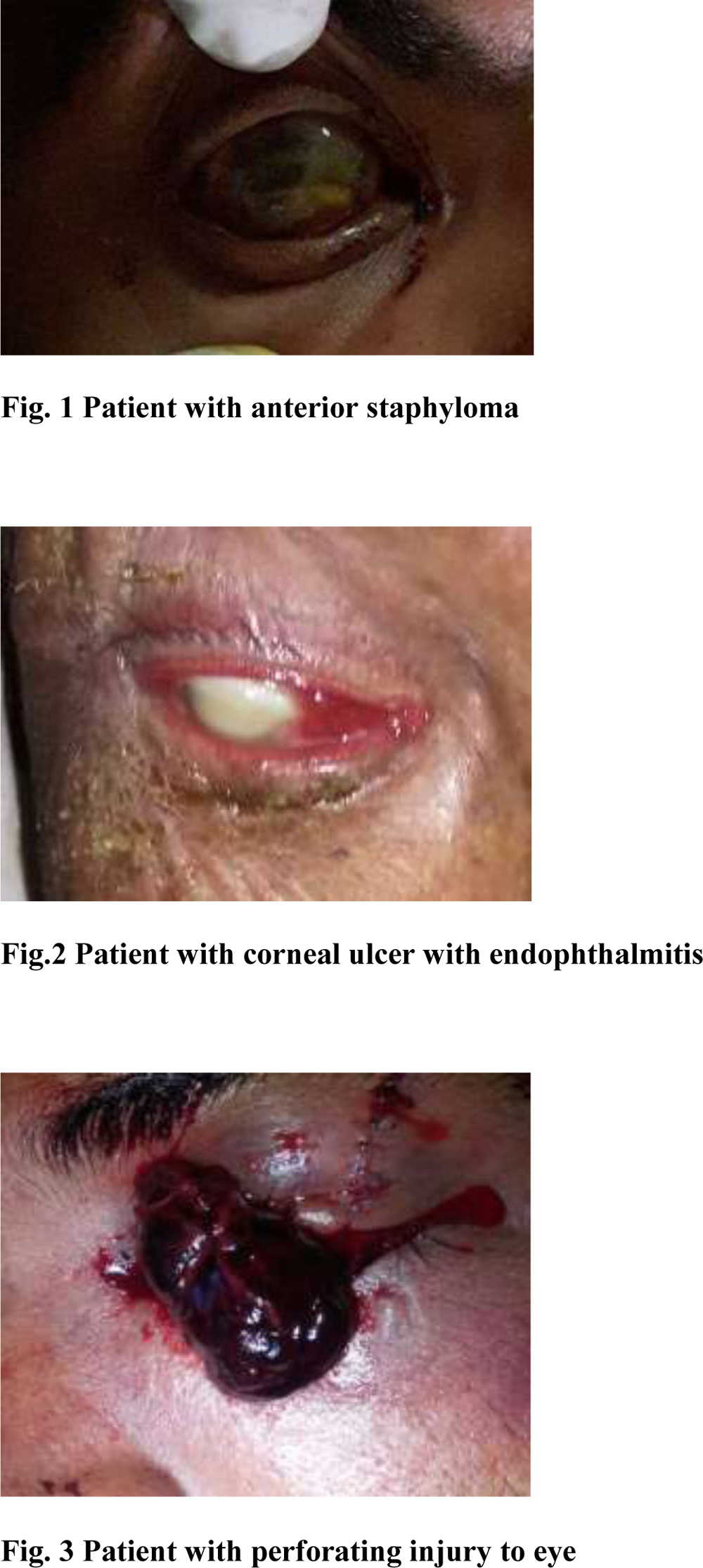 Fig. 3 Patient with perforating injury to eye
Fig. 3 Patient with perforating injury to eye
Table 2 Laterality of the eye in the study
| Eye involved | Frequency | Percent | |
| Valid | Left | 6 | 60.0 |
| Right | 4 | 40.0 | |
| Total | 10 | 100.0 | |
Left eye was operated in 6 and right eye in 4 of the patients.
Table 3 Number of patients under Below poverty line
| BPL CARD HOLDER | Frequency | Percent | |
| Valid | No | 3 | 30.0 |
| Yes | 7 | 70.0 | |
| Total | 10 | 100.0 | |
Majority of the patients (70%) were BPL card holders, who could not resort to other means of orbital volume replacement.
All the patients underwent primary dermis fat grafting following evisceration or enucleation.
 Fig. 4 Intra-op picture showing suturing dermis fat graft to the host conjunctiva
Fig. 4 Intra-op picture showing suturing dermis fat graft to the host conjunctiva
 Fig. 5 Post-op day1 picture following dermis fat grafting
Fig. 5 Post-op day1 picture following dermis fat grafting Fig. 5 Post-op 8 Fig. 5 Fig.5 Post-op 8 weeks picture following dermis fat grafting showing well integrated dermis fat graft and good orbital volume replacement
Fig. 5 Post-op 8 Fig. 5 Fig.5 Post-op 8 weeks picture following dermis fat grafting showing well integrated dermis fat graft and good orbital volume replacement
Fig. 6 Post-op 8 weeks picture following dermis fat grafting with prosthesis in-situ
Following dermis fat grafting, orbital volume replacement was studied by luedde’sproptometer.
Table 4 Proptometry reading of the other eye and test eye following dermis fat grafting
| Other eye proptometry | Post-op day 1 proptometry | Post-op 4 weeks proptometry | Post-op 8 weeks proptometry |
| mm | mm | mm | Mm |
| 18 | 23 | 19 | 15 |
| 17 | 25 | 22 | 20 |
| 20 | 24 | 22 | 21 |
| 22 | 26 | 24 | 22 |
| 19 | 25 | 23 | 22 |
| 17 | 26 | 23 | 21 |
| 21 | 27 | 25 | 21 |
| 18 | 24 | 22 | 20 |
| 19 | 24 | 23 | 21 |
| 18 | 24 | 21 | 20 |
| 19 | 24.8 (25) | 22.3 (22.8) | 20.3 (20.9) |
Mean proptometry of the other eye was 19mm. Operated eye mean proptometry was 25mm on post-op day 1, 23mm post-op 4th week, and 21mm post-op 8th week.
One of the patients had graft necrosis and was considered a failure.
9 out of 10 patients had good graft take up. A good orbital volume replacement was seen after 8 weeks post-operatively. 90% success rate found in the procedure done.
In 9 out of 10 patients, socket with the graft was healthy with deep fornices. Prosthesis fit was stable.
Table 5 Number of successful prosthesis fit
| Prosthesis fit | Frequency | Valid Percent | |
| Valid | fail | 1 | 10.0 |
| good | 9 | 90.0 | |
| Total | 10 | 100.0 | |
Table 6 Test statistics for the successful prosthesis fit
| Prosthesis fit | |
| Chi-Square | 6.400 |
| df | 1 |
| Asymp. Sig. | .011 |
We also measured the motility of the prosthetic eye in adduction, abduction and elevation.
 Fig. 7 Prosthetic eye motility tested using a plastic ruler
Fig. 7 Prosthetic eye motility tested using a plastic ruler
Table 7 Comparison of prosthetic eye motility with that of the other eye
| Mean motility | Other eye | Prosthetic eye | Failed eye with prosthesis |
| Adduction (mm) | 8.9 | 2.9 | 1 |
| Abduction (mm) | 7.9 | 2.9 | 1 |
| Elevation (mm) | 4.9 | 1.11 | 0 |
| Table 8 Paired Samples Statistics (eye motility) | |||||
| Oe- other eye
Te- test eye |
Mean | N | Std. Deviation | Std. Error Mean | |
| Pair 1 | Oe-add | 9.1250 | 8 | 1.72689 | .61055 |
| Te-add | 2.8750 | 8 | .83452 | .29505 | |
| Pair 2 | Oe-abd | 8.0000 | 8 | .75593 | .26726 |
| Te-abd | 2.8750 | 8 | .64087 | .22658 | |
| Pair 3 | Oe-ele | 5.0000 | 8 | .75593 | .26726 |
| Te-ele | 1.2500 | 8 | .70711 | .25000 | |
The motility of the successfully fat-grafted eye was reduced substantially in all patients as compared with the motility of the contralateral eye. A motility loss of 50% or more was found.
|
Table 9 Paired Samples Test (eye motility) |
||||||
| Oe-other eye
Te-test eye |
Paired Differences | t | df | Sig. (2-tailed) | ||
| Mean | Std. Deviation | |||||
| Pair 1 | Oe add – te add | 6.25000 | 1.28174 | 13.792 | 7 | .000 |
| Pair 2 | Oeabd – teabd | 5.12500 | .83452 | 17.370 | 7 | .000 |
| Pair 3 | Oeele – teele | 3.75000 | .88641 | 11.966 | 7 | .000 |
Profile plot for adduction, abduction and elevation (prosthetic eye compared to failed eye)
Fig. 8 Profile plots for motility (prosthetic eye and failed eye)
Mean motility of the prosthetic eyes was better than that of the eye with failed graft.
Discussion
Autologous dermis fat graft (DFG), composed of dermis and an attached subcutaneous fat, is an acceptable volume replacement implant for primary enucleation and evisceration.7-12 The dermal component, in orbit reconstruction provides structural support for the ingrowth of conjunctiva over the graft and its eventual vascularization. This minimizes reabsorption of graft fat with resultant replacement of lost orbital volume.9
It also preserves conjunctival surface area and deepens conjunctival fornix depth to enhance prosthesis fitting.9 Being autologous, it has neither the risk of rejection nor transfer of infection from cadaveric homologous tissue.10-12
Our study population included 3 females and 7 males between 24 and 65 years of age. 3 (30%) of them underwent enucleation and 7 (70%) evisceration. Indications were perforated corneal ulcer in 3 (30%), globe disfigurement due to trauma in 3 (30%), anterior staphyloma in 2(20%), painful blind eye due to neovascular glaucoma in 1 (10%) and failed corneal graft with endophthalmitis in one (10%) of the patients.
Majority of our patients (30%) were BPL card holders, who could not resort to costlier synthetic implants.
All the patients underwent primary dermis fat grafting following either evisceration or enucleation, operated by a single surgeon. Post-operatively, orbital volume replacement was analysed by proptometry on post-op day 1, 4th week and 8th week. It was seen that there was progressive decrease in proptometry reading which is due tofat shrinkage. It has been analysed by Dr. Al-Mujaini Abdulla et. al.,10that there is lack of predictability of fat shrinkage, resulting in underestimation of the volume of the fat required for orbital volume replacement.
To account for fat shrinkage, in our study we had purposely harvested comparatively a larger volume of fat with respect to the contents removed. There was good orbital volume replacement in 9 (90%) cases by 8th week post-operatively with a mean proptometry value of 21mm. In contrast, in children, it is seen that there is proliferation of the fat graft with subsequent integration with the orbital tissues. There may sometimes be overgrowth requiring debulking.11
By 8th week post-operatively, there was a good grafted, healthy socket, with deep fornices in 9 (90%) cases, resulting in stable prosthesis fit.
One of the cases showed necrosis of the graft with rapid decrease in its volume with poor take-up. There was poor vascularity and the graft appeared pale. There was dehiscence of the conjunctiva from the graft edge in one quadrant. However, there were no signs of infection. Patient was not willing for regrafting. There were no other complications seen unlike in other studies. A similar study conducted on Ghanaian children by Dr.Essuman VA et.al.,11 showed necrosis in 7% of the cases. There were other comlications like infection, microcysts, overgrowth requiring debulking.
All the eyes received prosthesis by the end of 6-8th week post-operatively and the fit was analysed. 9 (90%) patients showed stable fit. In one (10%) of the eyes with graft necrosis, prosthesis was not stable, with frequent extrusion.
We also measured the motility of the prosthetic eye in extreme directions of gaze. A noticeable lag of movement of the prosthetic eye was measured when compared to the contra-lateral eye in all directions of gaze. This decrease in motility may be explained by orbital tissue changes which follow enucleation and evisceration, fibrosis of the extraocular muscles, and inadequate transmission of movement from the anterior surface ofthe socket to the posterior surface of the prosthesis.A similar finding of overall lag of motility in prosthetic eye with various types of orbital implants was reported by other researchers.13-15 Motility of the prosthetic eye was least in case of failed graft.
Conclusion
Dermis fat grafting as a primary procedure in patients undergoing evisceration and enucleation is cosmetically better with good orbital volume replacement and stable prosthesis fitting with good motility.
Surgical procedure is easier to perform and requires minimum infrastructure. Primary dermis fat grafting is a novel technique for orbital volume replacement following enucleation and evisceration, especially in a developing nation like India where most of the population belong to BPL group, who cannot afford synthetic implants.
Bibliography
- Ton J Smit, Leo Koornneef, Erica Groet, Frans W Zonneveld, A Jan Otto. Prosthesis motility with and without intraorbital implants in the anophthalmic socket. Bnrtish Journal of Ophthalmology, 199;175:667-70.
- Kundu B, Sinha MK, Mitra S, Basy D.Synthetic Hydroxyapatite-based Integrated Orbital Implants: A Human Pilot Trial. Indian J Ophthalmol 2005;53:235-4.
- Smith B, Petrelli R. Dermis-fat graft as a movable implant within the muscle cone. Am J Ophthalmol. 1978;85:62-6.
- Paris GL, Spohn WG. Correction of enophthalmos in the anophthalmic orbit. Ophthalmology. 1980;87:1301-8.
- Li T, Shen J, Duffy MT. Exposure rates of wrapped and unwrapped orbital implants following enucleation. OphthalPlastReconstr Surg. 2001;17:431-5.
- McNab A. Hydoxyapatite orbital implants. Experience with 100 cases. Aust N Z J Ophthalmol. 1995;23:117-23.
- Essuman VA, Tagoe N N, Ndanu T A, Ntim-Amponsah C T. Dermis-Fat Grafts and Enucleation in Children in a West African Population. PlastReconstr Surg. 2013;131(3):457e–458e. doi: 10.1097/PRS.0b013e31827c7365. [PubMed] [Cross Ref]
- Sami D, Young S, Petersen R. Perspective on Orbital Enucleation Implants. Surv Ophthalmol.2007;52(3):244–265. [PubMed]
- Martin P, Rogers P, Billson F. Dermis-fat: evolution of a living prosthesis. Aust and N Z J Ophthalmol.1986;14(2):161–165. [PubMed]
- Al-Mujaini Abdullah, Ganesh Anuradha, Al-Zuhaibi Sana. Autogenous Dermis-Fat Orbital Implant for Anophthalmic Socket. Sultan QaboosUniv Med J. 2007;7(2):145–148. [PMC free article] [PubMed]
- Mitchell KT, Hollsten DA, White WL, O’Hara MA. The Autogenous Dermis-Fat Orbital Implant in Children. J AAPOS. 2001;5(6):367–369. [PubMed]
- Reza V M, McMullan TFW, Burroughs JR, Isaacs DK, Tsirbas A, White GL, Jr, Anderson RL, McCann JD. Autologous dermis graft at the time of evisceration or enucleation. Br J Ophthalmol. 2007;91(11):1528–1531. [PMC free article] [PubMed
- Sassmannshausen J, Bornfeld N, Kluge A, Sauerwein W, Harting F, Wessing A. Enucleation combined with orbital implants formalignant melanoma ofthe uvea. IntOphthalmol 1989; 13: 243-51.
- Tyers AG, Collin JRO. Baseball orbital implants: a review of 39 patients. BrJ7 Ophthalmol 1985; 69: 438-42.
- Bosniak SL, Nesi F, Smith BC, Schechter B, Cote R. A comparison of motility: autogenous dermis-fat vs synthetic spherical implants. Ophthalmic Surg 1989; 20: 889-981.