Dr. T Swetha, Dr.Sasikala Elizabeth Anil Kumar, Dr. Kalpana Narendran
Introduction:
In the growing modern medicine, cataract surgery in infants has become a common intraocular procedure. The time at which the child undergoes surgery and its relationship to the duration of deprivation has a vital role to play. Unilateral cataract operated within 6 weeks of birth results in better outcome. Bilateral cataract surgery should not be delayed longer than 10 weeks, else will lead to visual deprivation. The acceptable age at which intraocular lens (IOL) is planned for implantation is gradually decreasing. Calculation and selection of IOL power are among the major challenges for successful long term visual outcome in view of the axial growth and myopic shift in children. Presently, the initial desired refractive outcome following IOL implantation is towards hypermetropia, with the amount dependent on the child’s age.1 Refractive results after primary IOL implantation in children less than 24 months are variable. Limited data exists about their long term outcome.
Hence, we report our experience with these children in this study.
The study was aimed to analyze long term outcome in children who underwent cataract surgery for congenital cataract with intraocular lens implantation at ≤ 24 months of age.
Material and Methods:
This was a descriptive, analytic, retrospective study of children less than 2 years who had undergone phacoaspiration, primary posterior capsulotomy ( PPC ), anterior vitrectomy and primary IOL implantation with a minimum of 4 year follow up for congenital cataract. Traumatic cataracts and children with inadequate follow up were excluded. All children underwent a complete ocular evaluation. An ultrasound B scan was performed in cases with cataract obscuring the view of fundus. All surgeries were performed by a single senior surgeon. Keratometry was performed using hand held autokeratometer, and axial length was calculated using A-scan. IOL power was calculated using SRK II formula. IOL power was approximately based on the Dahan’s criteria (20% undercorrection in infants and 10 % under correction in toddlers). The operated eye received rigid PMMA lens or foldable acrylic lens.
Intraoperative details, immediate and late post operative complications were recorded. Post operatively visual acuity, retinoscopy, and spectacle spherical equivalence were recordedat 2 weeks, 1 month, 6 months and latest visit. Vision was recorded with Snellen’s chart at the latest visit. IOP was measured with pulse air non contact method and children with higher values were measured using Goldman applanation tonometer.
Results:
39 eyes of 30 children were analyzed. 21 children (70%) were operated for unilateral cataract and 9 children (30%) were operated for bilateral cataract. Of them 53% were male and 47% were female. 18 eyes (46.15%) were operated at ≤ 12 months of age and 21 eyes (53.84%) were operated between 13 months and 24 months of age. Mean age at surgery was 13.6 months (range 6 weeks to 24 months). Mean preoperative axial length was 21.14mm (range 18.35mm to 24.8mm) (Table-1). 49% presented with total cataract, 46% with lamellar cataract and 5% with posterior sub capsular cataract. The follow up ranged from 48 months to 116 months ( mean was 66.6 months ).
| PRE OPE AXIAL LENGTH(mm ) | NO. OF EYES |
| 18-20 | 11 |
| 20.01-22 | 15 |
| 22.01-24 | 12 |
| 24.01-26 | 1 |
Table: 1 Preoperative Axial Length of study group
Mean intraocular lens (IOL) power was 23.5 D. Of the type of IOL 90% eyes were implanted with acrylic lens and 10% with PMMA lens. All the eyes received an in the bag placement. None of the children had intra operative complications. 8(21%) had posterior capsule opacification and underwent membranectomy, 3(7.7%) children had IOL exchange due to large myopic shift. Nil had secondary glaucoma.
Shift in mean spherical equivalence (SE) was 4.43D at 2weeks postoperative to (-1.02D) at latest visit. Figure-1 shows the spherical equivalence of all the children at the latest visit. Mean myopic shift was 5.91D. Mean final visual acuity was 6/36 (logMAR-0.76). 46.1% had final visual acuity better than 6/18.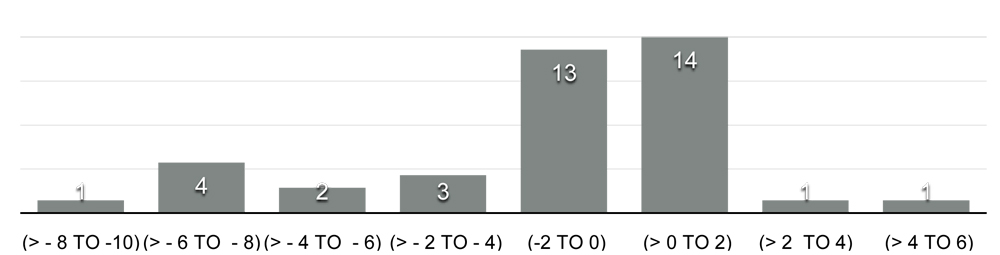
Comparison between children operated less than 12 months and 13 to 24 months of age for the myopic shift and visual acuity in the last visit had very high statistical significance (p<0.0003) (Table-2). Mean visual acuity at the latest visit in unilateral cataracts was 5/60 and 6/12 in bilateral cataracts, when compared showed high statistical significance (p<0.0001). 77% in the bilateral cataract group achieved final vision better than 6/18 (Table-3).
| ≤ 12 MONTHS | 13 -24 MONTHS | |
| LATEST VISIT VISUAL ACUITY
( Snellen’s ) |
6/60 | 6/24 |
| NO. OF EYES WITH VISION BETTER THAN 6/18 | 4 | 14 |
| MEAN SE 2WKS POST OP | 5.54 D | 3.47 D |
| MEAN SE LATEST VISIT | -2.27 D | 0.06 D |
| MEAN MYOPIC SHIFT | 7.51 D | 3.41 D |
| MEMBRANECTOMY | 5 Eyes | 3 Eyes |
| IOL EXCHANGE | 2 Eyes | 1 Eye |
Table: 2 – Comparison between children operated less than 12 months and 13to 24 months- Post operative visual and surgical outcome
| UNILATERAL CATARACT | BILATERAL CATARACT | |
| LATEST VISIT VISUAL ACUITY
( Snellen’s ) |
5/60 | 6/12 |
| NO. OF EYES WITH VISION BETTER THAN6/18 | 4 | 14 |
| MEAN SE 2WKS POST OP | 4.35 D | 4.51 D |
| MEAN SE LATEST VISIT | -1.58 D | -0.36 D |
| MEAN MYOPIC SHIFT | 5.65 D | 4.9 D |
| MEMBRANECTOMY | 5 Eyes | 3 Eyes |
| IOL EXCHANGE | 1 Eye | 2 Eyes |
Table: 3 – Comparison between children with unilateral and bilateral cataract- Post operative visual and surgical outcome
Discussion :
The final goal of pediatric cataract surgery is successful visual rehabilitation. Careful and diligently performed primary IOL implantation can be an effective method of aphakic correction in children younger than two years of age with reduced complications.2 The long term outcome of primary IOL in children less than 2 years is not clear due to very few studies reporting such results.3
Our study had 70% unilateral and 30% bilateral cataracts while the study by Jagat Ram et al reported 44% and 66% respectively.2 Our study comprised 53% male and 47% female children while Amit Gupta et al had 49% and 51% respectively.4 In his study the mean age at surgery was 11.21 ± 5.90 months 4, while our study reports it as 13.6 months. We had 46.1% children operated within 12 months and 53.8 % between 13 to 24 months of age wherein, the other study by Jaspreet Sukhija et al was 63% and 27% respectively.3 Studies which have reported safety profile of primary IOL implantation had a mean follow up as short as 8.5 months4 and as long as 102 months.3
Gouws et al. showed that 50% achieved 6/18 or better visual acuity5 and Jaspreet Sukhija et al had final best corrected visual acuity 6/18 or more in 92% eyes, about 73% achieved 6/12 or better when both eyes were operated.3 Our study had mean visual acuity of 6/36 and about 6/12 in the bilateral cataract group when both eyes were operated, results comparable to the above studies.
| Post op complications | Amit Gupta et al4 | Jagat Ram et al2 | Our study |
| PCO | 6.7% | 13.3% | 21% |
| Fibrinous membrane | 4.2% | 8.9% | – |
| Glaucoma | – | 0.5% | – |
Table 4 : Comparison of post op complications with other studies.
Vasavada et al reported visual axis opacification in 39.8% of the children and postulated that the anterior vitreous face is more reactive in young children which can act as a scaffold not only for lens epithelial cell proliferation but also fibrinous exudates, pigment epithelial cells and cells that are formed following the breakdown of the blood aqueous barrier causing posterior capsule opacification.2,6 Our patients underwent manual PPC via anterior route after IOL implantation as it has increased resistance to a radial tear as compared to vitrector in infantile eyes. We had higher incidence of membranectomy in comparison to Amit Gupta et al (6.7 %)4 and Jagat Ram et al (13.3%)2 studies (Table-4); however most of these eyes underwent surgery before 12 months. There was no recurrence of visual axis opacification after membranectomy in our study.
Trivedi et al reported the incidence of glaucoma to be 24.4% after IOL implantation.7 Wong et al reported that 13.5% of infant eyes undergoing IOL implantation are likely to develop glaucoma.8 It has also been noted that incidence of glaucoma can be reduced by placing foldable IOL.4 Our study majority (90%) of the children received foldable acrylic intraocular lens and we had nil cases of secondary glaucoma (Table-4).
| Jaspreet Sukhija et al3 | Jagat ram et al2 | Our study | |
| Immediate post op SE | 1.64D | 3.38 D | 4.43D |
| Final SE | -1.42 D | -0.51D | -1.02D |
| Myopic shift | 3.06 D | 3.89 D | 5.91 D |
Table 5: Comparison of spherical equivalence (SE) among other studies.
We had 3 children undergoing IOL exchange for reason of myopic shift at age of 8 years. Children operated at early age can have much more myopic shift than older children. This is because their IOL power is fixed, while the lens power in the phakic eye changes so as to compensate for the axial growth. This trend of myopia in pseudophakic eye is the result of normal eye growth. Studies have shown that pseudophakic eyes tend to have most growth (axial elongation) during the first 2 years of life, and continue to grow slowly up till the age of 8 years.9 Determination of the accurate IOL power for an infant eye poses a unique challenge. Children would emmetropise or tend to be slightly myopic by the time they would be school going.2Crouch et al showed a myopic shift of 5.96 in children <2 years age with a mean follow up of 5.4 years similar to our study. For better refractive results, studies have shown a guide for selecting IOL power in pediatric cataracts, using current formulas with the understanding that new formulas will need to be devised for better prediction of IOL power.10
To conclude, with the improvement in surgical techniques and presently available modern surgical equipment, cataract surgery in young eyes has become much safer. It results in visual rehabilitation in children with IOL implantation at a much younger age. Our study shows a favorable long term outcome of primary IOL implantation in children who were operated before 2 years of age. The importance lies in choosing an appropriate IOL power in this age group in view of the myopic shift.
REFERENCES
- Lloyd I C, Ashworth J, Biswas S. Advances in the management of congenital and infantile cataract. Eye 2007; 21:1301–9.
- Ram J, Brar GS, Kaushik S. Primary intraocular lens implantation in the first two years of life: Safety profile and visual results. Indian J Ophthalmol 2007;55:185-9
- Sukhija J, Ram J, Gupta N, Sawhney A, Kaur S. Long-term results after primary intraocular lens implantation in children operated less than 2 years of age for congenital cataract. Indian J Ophthalmol. 2014;62:1132–5
- Gupta A, Kekunnaya R, Ramappa M, Vadavalli PK. Safety profile of primary intraocular lens implantation in children below 2 years of age.Br J Ophthalmol. 2011;95:477-8
- GouwsP, HussinHM, MarkhamRH. Long term results of primary posterior chamber intraocular lens implantation for congenital cataract in the first year of life. Br J Ophthalmol 2006;90:975‐
- Vasavada AR, Trivedi RH, Nath VC. Visual axis opacification after AcrySof intraocular lens implantation in children. J Cataract Refract Surg 2004;30:1073e81.
- Trivedi RH, Wilson ME Jr, Golub RL. Incidence and risk factors for glaucoma after pediatric cataract surgery with and without intraocular lens implantation. J AAPOS 2006;10:117e23.
- Wong IB, Sukthankar VD, Cortina-Borja M, et al. Incidence of early-onset glaucoma after infant cataract extraction with and without intraocular lens implantation.Br J Ophthalmol 2009;93:1200e3.
- Althomali T, Awad AH. Myopic shift in pediatric pseudophakia: Long-term follow-up. Saudi J Health Sci 2012; 1: 85-8.
- Crouch ER, Crouch ER Jr, Pressman SH. Prospective analysis of pediatric pseudophakia: Myopic shift and postoperative outcomes. J AAPOS 2002;6:277‑82