Dr. Mihir Trilok Kothari, K08617, Dr.Shruti Lad, Md. Oliullah Abdal
FP938 No financial conflict
Kothari Mihir, AbdalOliUllah, Lad Shruti
Krishna Eye Center, Parel; Jyotirmay Eye Clinic and Ocular Motility Laboratory, Thane and Mahatme Eye Hospital, Nagpur
Introduction:
Amblyopia has a3-5%population prevalence and remains the commonest cause of monocular blindness in age group 20-50 years. Next to refractive error, amblyopia is an ophthalmic disorder with the best opportunity-cost. The conventional treatment for unilateral amblyopia is still the occlusion therapy or patching. However, there are at least6 major issues with this therapy.
- Residual Amblyopia
- Poor compliance
- Poor response in older children and adult amblyopes
- Recurrence after cessation of treatment
- Lack of improvement in the visuomotor skills, binocular fusion, stereopsis and ocular motility deficits viz. saccades and pursuits
- Slow improvement despite of long patching hours and good compliance
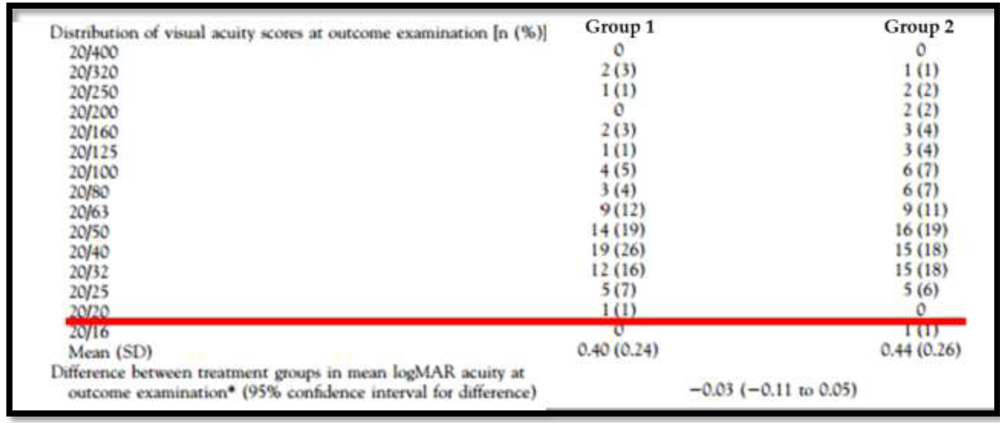
1] In ATS 2A – 6 hr versus Full time patching, aged 3-7 years age, patients with severe amblyopia more than 85% had residual amblyopia of >2lines at 4 months (Figure 1).
Figure 1: Showing the residual amblyopia after 6 hours/day patching (group 1) and full time patching (group 2) in anisometropic amblyopia as reported in ATS 2A of PEDIG.
2] Next to the age compliance is the single most important determinant of outcome of amblyopia therapy. The compliance to patching is reported to be 50-% in age group > 5 years. Highest reported compliance is 70%.
3]Adult Amblyopia in ATS 3- a randomized trial of treatment of amblyopia in children aged 7 to 17 years. < 50% responded to patching(47% in < 12 years and 25% in 12-17) if they had never done any patching in the past. Most patients, including responders, were left with major residual visual acuity deficit.
4] Approximately one fourth (24%) of successfully treated amblyopic children experience a recurrence within the first year after cessation of the treatment. Even with maintenance patching, 8-10% will have >1 line drop in the visual acuity.
5] Multiple residual deficits inbinocularity (fusion and stereopsis), hand eye coordination (fine motor skills) and ocular motor deficits (saccades, pursuits) are present in children with amblyopia and all of them a negative impact on the vision related quality of life in the affected individuals.
6] In ATS 2A (6hours/day versus full time patching for severe amblyopia) and ATS 2B (6hr and minimal 2hr patching for mild or moderate amblyopia) the fastest improvement in visual acuity was 4.8 lines in 4 months with 6hr/day patching.
Due to all these reasons it was necessary to look for newer, better and more effective option for the management of amblyopia.
In this study we report the results of home based as well as office based vision therapy for residual amblyopia.
Materials and Methods:
This prospective cohort study included children or adults aged >6 years having anisometropic or strabismic residual unilateral or bilateral amblyopia (inter eye acuity difference of > 2 lines) that did not respond to 100% compliance to 6 hours/day patching for atleast 3 months and full time-full spectacle correction of the refractive error. Patients with deprivational amblyopia or any other ocular comorbidity or neuronal defects were excluded. The patients were randomly assigned to office therapy or home therapy.
Office therapy (Group 1):
20 minutes session each of antisuppression using monocular fixation in binocular field (MFBF) were given using Sanet Vision Integrator touch screen system followed by Contour and random dot stereopsis exercises on 3D screen of the vision therapy system 4 (VTS4). The contrast of the dominant eye target was kept at the lowest level which induced fusion in the patient. In patients with large manifest squint, binasal occlusion was utilized to induce fusion to begin MFBF therapy. Following 2-3 sessions, none of the patients needed binasal occlusion. Alternate day sessions were given for 6 weeks and the data was analyzed. The patching of 2hrs/day was continued along with the office therapy. Spatial frequency (crowding) was increased as the visual acuity improved.
Home therapy (Group 2):
5 hours / week of MFBF was given for 6 weeks sans patching using 3D anyglyph goggles and android game called Stereoblocks. The dominant eye settings of the stereo block game were adjusted to 100% contrast and the lazy eye setting was adjusted to the minimum contrast that lead to fusion response. Data was analyzed after 6 weeks of therapy.
Results:
In group 1, sixteen eyes of 11 children were included. 5 had bilateral and 6 had unilateral (anisometropic/strabismic/mixed) amblyopia. Mean age was 12.5 years. Mean improvement in bilateral amblyopia (n=10) was 0.26, p<0.01 (paired t test) and in unilateral amblyopia (n=5) it was 0.28, p=0.05. Maximum improvement in bilateral amblyopia was 0.48 (5 lines on logMAR chart) and in unilateral was 0.6 (6 lines). 4 patients with age >18 years experienced mean 2.5 lines improvement.
in group 2, seven eyes of seven patients were included that aged 6-15 years. Five hadstrabismic amblyopia and 2 had anisometropic amblyopia. The best corrected vision improved in all by 1-3 lines a mean 1.8 lines improvement.
Discussion:
In this study MFBF was associated with significant improvement in visual acuity of the eye with residual amblyopia. The improvement was more rapid compared to conventional occlusion and more effective in office based therapy either because of simultaneous part time patching or due to monitored therapy or both.
The principle of the dichoptic therapy is that a contrast adjusted stimulus is presented exclusively to each eye where-in the image of right eye was visible only to that eye and the image of the left eye was visible only to the left eye. The brain was forced to integrate the images into a single perception.
Normallybinocular interaction does not occur in amblyopia. Weak, noisy signals from the amblyopic eye can contribute to binocular vision if suppression by the fellow eye is reduced when fellow-eye contrast is reduced (or by any other method of by signal attenuation).
Recently work from Robert Hess, Eileen Birch, Robert Sanet etc. have demonstrated that dichoptic treatment by home therapy or office therapy or using dichoptic movies can be useful in children as well as adult amblyopia.
In the study by Birch EE, Binocular iPad treatment for amblyopia was given.4 hr/ week / 4 weeks of Sham games vs. iPad dichoptic games were given.Sham iPad group had no significant improvement. Binocular iPad group had mean visual acuity improvement by > 1 line. They found more improvement with more compliance and more improvement (3 lines more ) with associated patching, similar to what we have experienced during this study. With iPad games, best improvement was 4.7 lines in 1 month and the continued treatment did not show further improvement. Also, there was no recurrence after cessation for 3 months. They reported no effect on stereoacuity. The limitation of the treatment was compliance because the tasks are intensive and repetitive and up to 40% of unsupervised patients werenoncompliant.
In summary, the new Dichoptic therapies along with patching seem very promising. However, further studies are needed to identify the long term effect on the vision related quality of life with these newer modalities of treatment and its sustenance. Vision therapy using SVI, VTS 4 or home therapy may be effective in the treatment of disorders of binocular vision especially for the oculomotor deficits and visuomotor skills.
References:
- Sengpiel F, Jirmann KU, Vorobyov V, Eysel UT. Strabismic suppression is mediated by inhibitory interactions in the primary visual cortex.Cereb Cortex. 2006 Dec; 16(12):1750-8.
- Bi H, Zhang B, Tao X, Harwerth RS, Smith EL 3rd, Chino YM.Neuronal responses in visual area V2 (V2) of macaque monkeys with strabismic amblyopia.Cereb Cortex. 2011 Sep; 21(9):2033-45.
- Hess RF, Mansouri B, Thompson B. A new binocular approach to the treatment of amblyopia in adults well beyond the critical period of visual development. RestorNeurolNeurosci. 2010;28:793–802.
- Hess RF, Thompson B, Black JM, et al. An iPod treatment of amblyopia: an updated binocular approach. Optometry. 2012;83:87–94.
- Thompson B, Blum JR, Maehara G, Hess RF, Cooperstock JR. A game platform for treatment of amblyopia. IEEE Trans Neural Sys Rehab Eng. 2011;19:280–89.
- Knox PJ, Simmers AJ, Gray LS, Cleary M. An exploratory study: prolonged periods of binocular stimulation can provide an effective treatment for childhood amblyopia. Invest Ophthalmol Vis Sci. 2012;53:817–24.
- Birch EE, Li SL, Jost RM, Morale SE, De La Cruz A, Stager D Jr, Dao L, Stager DR Sr. Binocular iPad treatment for amblyopia in preschool children. J AAPOS. 2015 Feb;19(1):6-11.
- Li SL, Jost RM, Morale SE, Stager DR, Dao L, Stager D, Birch EE. A binocular iPad treatment for amblyopic children. Eye (Lond). 2014 Oct;28(10):1246-53.
- LiSL, Reynaud A, Hess RF, Wang YZ, Jost RM, Morale SE, De La Cruz A, Dao L, Stager D Jr, Birch EE. Dichoptic movie viewing treats childhood amblyopia. J AAPOS. 2015 Oct;19(5):401-5.