Dr. Spurthi G Reddy, S12838, Dr.S Bala Murugan, Dr. Girish Bharat Velis, Dr.Annamalai O
CASE SERIES OF OCULAR TOXOCARIASIS (OT) IN A TERTIARY EYE CARE CENTRE IN SOUTH INDIA
Ocular Toxocariasis (OT) is a clinically well-defined manifestation of Toxocara infection caused by Toxocara canis or Toxocara cati. Dogs, wolves, and foxes are the definitive hosts for T.canis, whereas domestic cats host T. cati. It usually affects children, causing painless unilateralvision loss, strabismus, or leukocoria. Human infection occurs when a child ingests food or soil contaminated by the feces of one of those species harboring unembryonated eggs (with Stage 1 larvae). Eggs hatch into stage 2 larvae in the humanduodenum and perforate the intestinal wall to gain access to the bloodstream and can potentially get lodged (Stage 3 larvae) or get encysted in any part (Figure 1).
Figure 1: Life cycle of Toxocara canis
For Editor Sir to decide: CDC picture can violate the copyright
Toxocariasis is a significant international cause of posterior uveitis. One meta-analysis found that Toxocariasis ranks fifth most common, after toxoplasmosis, idiopathic, sarcoidosis, and Behcet disease.1
There are two forms of Toxocariasis, the Ocular Toxocariasis and the Visceral Toxocariasis (Visceral Larva Migrans) which rarely coexist in a single patient.
Purpose
To report the demographic, epidemiologic, clinical characteristics and therapeutic outcomes ofpatients with OT in a tertiary eye care center in South India.
Materials and Methods
A retrospective chart analysis of 30 eyes of 30 patients, presenting to theUvea services between 1st May 2013 and 31st May 2016 with a diagnosis of Ocular Toxocariasis, was conducted.Institute Ethics Committee approval was obtained.Inclusion criteria of enrolled patients were:
- Complete clinical records of best-corrected visual acuity (BCVA), slit lamp biomicroscopic examination, intraocular pressure, and availabletreatment records at baseline and follow-up visits,complications if any;
- Cases with complete evaluation to rule out TB and Syphilis (like Mantoux test, TPHA
- Evidence of active or inactive or presumed OTin one eye without any other evidence of inflammation in the other eye
- All other known causes of infectious and noninfectious uveitisand mimicking masquerading syndromes excluded by clinical features orrelevant tests, and
- Aminimum of 6 months of follow-up from the initiationof treatment.
All patients underwent a complete ocular as well as systemic examination,followed by baseline investigations. The information that we retrieved from the chart records included demographic(such as patient’s age, sex, laterality of uveitis) and clinical details (presenceof any inflammation in the anterior chamber or vitreous, treatment records,response to treatment in terms of progression/quiescence/recurrence of inflammation, duration of treatment and follow up from its initiation, visualoutcome, and complications, if any). Morphological description of clinical lesions (as they evolved from an acute stage up to healed stage until the last follow up) was obtained. Fundus Fluorescein angiography(FFA) images, USG B-scans and digital fundus images were analyzed wherever applicable.ELISA of serum or intra ocular fluids was performed in feasible cases.
Standardisation
All cases were evaluated by a single experienced uvea specialist (BM).
Steroids were given by more than one route of administration in 50% of patients.Oral steroids were given in the dose of 1mg/Kg and titrated according to bodyweight. Gastro protectives and calcium supplements were given along with steroids. Posterior Sub Tenon’s 0.5 cc Kenacortis given in 17%. Oral Albendazole was given in the dose of 10mg/Kg under cover of systemic steroids. Adjunct topical steroids and cycloplegics were given in eyes with active inflammation.
Results
A total of 30 eyes of 30 patients with OT were analysed. The demographic characteristics are summarised in Table 1. Reported patients with OT were young, with a median age of 18.4 years (Range 4–55 years) and slight female preponderence. Forty four percent patients with OT lived in the urban suburbs and 66% in rural environment. Patients with OT were located to 6 districts of Tamilnadu and Puducherry.
Table 1: Demographic Characteristics
| Mean age at presentation (years) | 18.4 (4-55) |
| Sex
Male Female
|
43%(n=13) 57%(n=17) |
| History of contact with pets | 13% |
| History of Pica | 7% |
| Environment
Urban Rural |
44% 66% |
All reported patients with OT had unilateral eye disease.We report 93% patients with active OT at presentation had resolution of inflammation at the time of their last office visit. Vision loss was the most commonly reported symptom affecting 85% of patients with OT with 70% of them having permanent vision loss. Reasons for permanent vision loss were subretinal granulomatous mass/scar, peripheral granuloma with traction bands, RD or posterior pole granuloma noted on ophthalmologic examination. Granulomas were peripheral in 74%, which is consistent with studies2 (Figure 2).Tables 2 and 3 summarise the data on clinical presentation and sequelae respectively.
Figure 2: Peripheral granuloma with traction band (B-scan)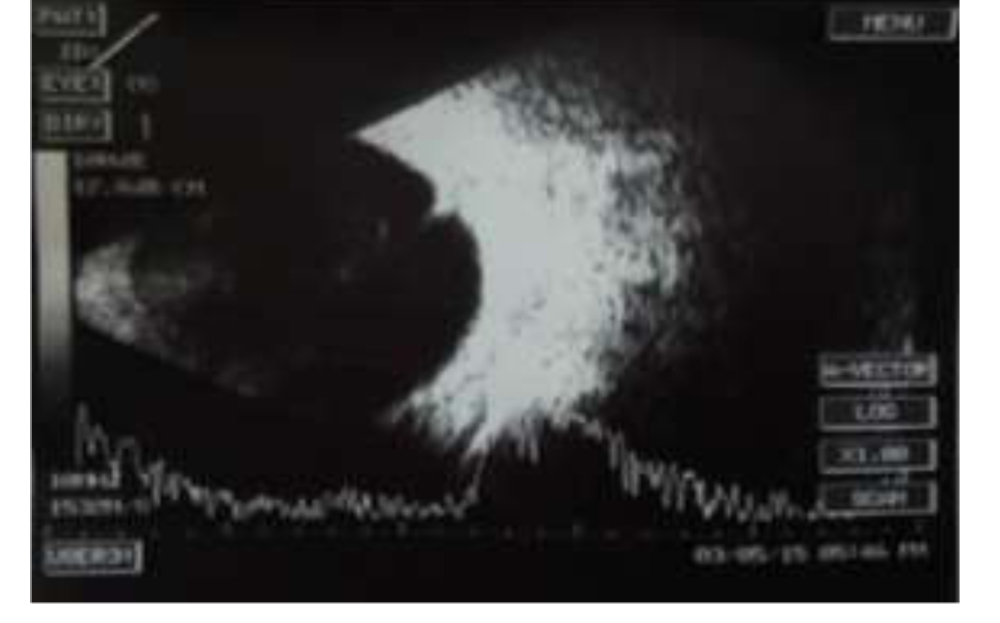
Figure 3: Posterior pole granuloma
 Table 2: Clinical presentation and course
Table 2: Clinical presentation and course
| Active OT | 66% |
| Sequelae | 21% |
| BCVA
Improved Stable Worsened |
20%(6) 10%(3) 13%(4) |
| Hypopyon uveitis | 3.5% |
| Peripheral granuloma | 74% |
| Posterior pole granuloma | 26% |
| Endophthalmitis | 3.5% |
Table 3: Sequelae
| Scarring | 20.6% |
| ERM | 10% |
| CME | 10% |
| Retinal fold | 7% |
| TRD | 3.5% |
| Cataract | 2% |
| SACG | 7% |
Surgical treatment (Table 4) was done for complications from Toxocara infection. The most common surgical procedure performed was pars plana vitrectomy (10%). Diode Cyclo Photo Coagulation was done for one eye which developed secondary angle closure glaucoma with no visual potential. Barrage laser was done for one eye with focal TRD. Sequelae at presentation were found in 20% (6 patients), with majority of them being sub retinal scarring.
Surgical intervention – Table 4
| PPV | 10% |
| Diode CPC | 3.5% |
| Cataract extraction | Nil |
Data regarding medical treatment showed corticosteroidsas the most common treatment used, the route of drugadministration varied, with approximately half being provided more than one route. Few required periocular steroid administration.
Discussion
Our study demonstrates that Ocular Toxocariasis remains acause of preventable vision loss affecting primarily children.Reported data regarding age and sex of patientswith OT in this study were consistent with results from previousstudies.3,4
Painless unilateral vision loss wasthe number one symptom in patients with OT; these data areconsistent with symptoms of patients with OT reported fromsmaller case studies.5 Peripheral subretinal granulomatousmass/scar was the most common sign seen in patients with OTreported in our study. This finding parallels results fromprevious studies in which peripheral granuloma was the mostcommon ophthalmologic finding, accounting for approximatelyone half of all reported cases.6-8A significantportion of patients with OT in this survey had a posterior pole granuloma (Figure 3). Posterior pole granulomas are more common inchildren with leukocoria, strabismus, or vision loss whothen present to ophthalmologists.9Migration of granuloma has been reported in literature but not noted in any of our cases.10
Although we know infection with Toxocara can lead topermanent debilitating ocular damage, it remains an obscuredisease. Increasing public awareness about toxocariasis isthe first step in reducing human exposure to Toxocara.Healthcare professionals, especially pediatricians and familyphysicians, are in a unique position to counsel familiesabout toxocariasis during routine medical visits.
Pet ownersshould be counseled to dispose of pet faeces promptly and totake their pets to the veterinarian for regular deworming.Emphasis should also be placed on good hygiene practices,such as hand washing, especially after exposure to high-riskareas such as sandboxes and playgrounds. Children shouldbe prevented from accidentally ingesting dirt.
Soil prevalence studies have documented higher concentrations of Toxocara eggs in warmer climates, which correlates with climate in South India. Previous studies have also established ownership of a dog or cat as a risk factor for infection with Toxocara5, but majority of our patients did not own a household pet.
Current serologic testing for antibody to theToxocara parasite does not reliably indicate active infection;studies have also shown that the immunoglobulin-GToxocara antibody can remain detectable for years after treatment, which limits the applicability of the test to monitortreatment success.11 In addition, a negative test resultdoes not rule out Toxocara infection.12 One recent studysuggests that testing for intraocular Toxocara antibody productionmay help establish the diagnosis of OT, althoughmost ophthalmologists arenot testing intraocular fluid.13 Testing for eosinophilia israrely done because it is neither sensitive nor specific fordiagnosing ocular Toxocara infection.14ELISA titer of 1:32 carries a 78% sensitivity and 92% specificity in VLM and 1:8 carries 90% sensitivity and 91% specificity in OLM. Specificity and sensitivity can be unreliable due to cross reaction with helminths and sub clinical seropositivity respectively.
Conclusion
Systemic and periocular corticosteroids are the first line and mainstay of therapy in active OT and use of antihelminthic drugs is equivocal and have to be used under cover of steroids. Ocular Toxocariasis continues to occur in South India, where it affects mainly children and young adults and may cause permanent vision loss. Healthcare professionals should counsel patients and their family members about prevention strategies in an effort to decrease infection rates and morbidity due to Toxocara.
Physicians will need to continue to rely on ophthalmologic examination findings to diagnose OT and use diagnostic test results cautiously in making the diagnosis.
References
1.Chang JHM, Wakefield D. Uveitis a global perspective. Immunol Inflamm 2002; 10: 263-279.
2.Woodhall D, Starr MC, Montgomery SP, Jones JL, Lum F, Read RW, Moorthy RS. Ocular toxocariasis: epidemiologic anatomic and therapeutic variations based on a survey of ophthalmic subspecialiats. J Ophthalmology 2012; 119: 1211-7.
3.Domenico Otranto , Mark L Eberhard. Zoonotic Helminths affecting the human eye. Parasit Vectors 2011: 4: 41. (E-Pub).
4.Mulvihill A, Bowell R, Lanigan B, O’Keefe M.Uniocular childhood blindness: a prospective study J Pediatr Ophthalmol Strabismus.1997; 34(2):111-4.
5.Schantz PM, Weis PE, Pollard ZF, White MC. Risk factors fortoxocaral ocular larva migrans: a case-control study. Am JPublic Health 1980; 70:1269 –72.
6.Pivetti-Pezzi P. Ocular toxocariasis. Int J Med Sci 2009; 6:129 –30. (E-Pub).
7.Wilkinson CP, Welch RB. Intraocular toxocara. Am J Ophthalmol1971; 71:92130.
8.Gillespie SH, Dinning WJ, Voller A, Crowcroft NS. TheSpectrum of ocular toxocariasis. Eye (Lond) 1993; 7:415– 8.
9.Ellis GS Jr, Pakalnis VA, Worley G, et al. Toxocara canis Infestation: clinical and epidemiologic associations with seropositivity in kindergarten children. Ophthalmology 1986; 93:1032–7.
10.Dhashanii Sivaratnam, Visvaraja Subrayan, Nadir AliTransvitreal migration of a Toxocara larva resulting in a second chorioretinal granulomaJapanese Journal of Ophthalmology 2008;52(5):416-7.
11.Małafiej E, Spiewak E. The significance of the level of antibodiesin the evaluation of the effects of treatment of toxocariasis. Wiad Parazytol 2001; 47:805–10
12.Schantz PM, Meyer D, Glickman LT. Clinical, serologic andepidemiologic characteristics of ocular toxocariasis. Am JTrop Med Hyg 1979; 28:24–8.
13.de Visser L, Rothova A, de Boer JH, et al. Diagnosis of oculartoxocariasis by establishing intraocular antibody production.Am J Ophthalmol 2008; 145:369 –74
14.Bass JL, Mehta KA, Glickman LT, et al. Asymptomatic toxocariasisin children: a prospective study and treatment trial.Clin Pediatr (Phila) 1987; 26:441– 6.