Dr. Akanksha, Dr.Dipankar Das
Full text AIOC 2017- FP-1119:
Category: Uvea
Title of the paper: “The Pretentious Uveitis: Masquarade Syndromes”
Presenting Author- AkankshaKoul
Co- Author: Dipankar Das(D08987)
INTRODUCTION
Masquerade syndromes are disorders that can present with intraocular inflammation and are often misdiagnosed as a chronic idiopathic uveitis. The term “Masquerade Syndrome” was first used in 1967 to describe a case of conjunctival carcinoma that manifested as chronic conjunctivitis. (1) Today, it is used to describe disorders that simulate chronic uveitis and are not immune mediated in the usual way. Because of the nature of the underlying diseases, which often have detrimental consequences, early diagnosis and prompt treatment are critical. The underlying pathological pathways leading to the metastatic spread of tumour cells within the fluid compartments of the eye remain unclear.
Various systemic malignancies have been known to masquerade as chronic inflammatory disorders, more often as those not responding to conventional anti-inflammatory therapy.Reported literature exists for the presence of pseudohypopyon in patients with a malignant tumour such as Ewing’s sarcoma. (2)
We report three cases of masquerade syndrome – in a patient of Non-Hodgkin’s lymphoma(NHL), an Immunoglobulin G4 related disease and a paraneoplastic retinopathy secondary to lymphoma.
NHL is often fatal because of its association with the central nervous system and majority are of B cell origin. (3) The lymphomas are considerably more misdiagnosed since the patients are initially responsive to corticosteroids. It can be suspected in all cases of chronic posterior uveitis in patients over 50 years old.Immunoglobulin G4‑related disease (IgG4‑RD) is a relatively new and uncommon clinical entity seen in various organs and tissues of the body and associated with elevated serum levels of IgG4. (4) The disease has a relapsing‑remitting course, and it is associated with local tissue damage in various sites with characteristic histopathological appearance.
Paraneoplastic retinopathy (PR) is a progressive retinal disease caused by antibodies generated from neoplasms distant from the eye. PR is thought to be mediated by an autoimmune mechanism, and is associated with the presence of auto-antibodies in the serum.
Various types of neoplasms are known to cause PR, including malignancies of the lung, breast, cervix, colon, prostate/bladder, uterus/endometrium, and blood cells. Only two cases of PR associated with a sarcoma, a malignant tumour arising from mesenchymal cells, have been reported. (5)
It is extremely important to recognize these masquerading diseases, find the underlying primary cause and immediate treatment of the same, to reduce the associated morbidity and mortality. The physician should keep these differentials in mind to avoid misdiagnosing and providing wrong treatment for potentially fatal malignancies.
Case 1
62-year-old male patient presented to us with complains of blurred vision in the right eye since a week. It was a gradual painless decrease in vision. On examination the vision was 20/200 in the right eye with anterior segment inflammation cells ++, flare ++ and grade 1 hypopyon. On dilated posterior segment examination Exudative retinal detachment was noted. The intraocular pressure was recorded to be 8 mm of Hg in the right eye. The examination of left eye was unremarkable. On further questioning regarding the history of the patient, he revealed that he had been diagnosed to have abdominal Non-Hodgkin’s lymphoma and had received chemotherapy for the same 2 years back. During the follow up period of past 2 years all PET scans showed no active malignant lesion. In consultation with the internist, the patient was put on oral steroids at the dose of 1 mg/kg. on the follow up visit after a month, the patient showed clinical improvement and vision had improved to 6/9 with a trace hypopyon. But after 4 weeks, he came back with a recurrence with sudden decease in vision with grade 2 hypopyon and an intraocular pressure of 38 mm Hg (Fig 1). When a PET scan was advised in consultation of an internist, active lesions were picked up and the patient immediately referred to an oncologist for repeat cycles of chemotherapy.
Case 2
A 23‑year‑old Indian female presented with the chief complaints of dimness of vision, pain and redness in the right eye (OD) for 3 months. The patient was previously treated elsewhere with two posterior sub‑Tenon injections of triamcinolone acetonide given 6 weeks apart. Other medical, surgical, and family histories were unremarkable. On examination, ocular alignment was normal with a visual acuity of counting finger at 3 m in the OD. There was minimal sclerouveitis noted in the inferior‑temporal quadrant of OD. On slit‑lamp examination, OD showed 360° posterior synechiae with anterior chamber flare and cells (+++) with 1 mm hypopyon(Fig 2). There was a suspected mass in the inferior‑temporal quadrant behind the iris, pushing it anteriorly. The left eye examination was unremarkable. B‑scan ultrasound (B‑scan USG) of OD was suggestive of ciliary body mass with adjoining exudative retinal detachment (ERD). USG bio‑microscopy findings were consistent with the findings of B‑scan USG.
Based on the clinical examination and baseline investigations, we came to the differential diagnosis of ciliary body melanoma or similar tumors. Magnetic resonance imaging suggested the possibility of ciliary body melanoma in OD. After obtaining informed consent, enucleation was carried out in OD, and eyeball specimen was sent to ocular pathology laboratory for histopathological analysis. In grossing, there was a grayish‑white‑coloredtumor seen in the inferior‑temporal part of the ciliary body measuring (10.99 × 7.98) mm. Adjoining the grayish‑white ciliary body mass, there was an ERD noted.An eosinophilic mass was seen in the ciliary body with diffuse plasmacytoid cells, with reactive lymphoid follicle and other inflammatory cells.
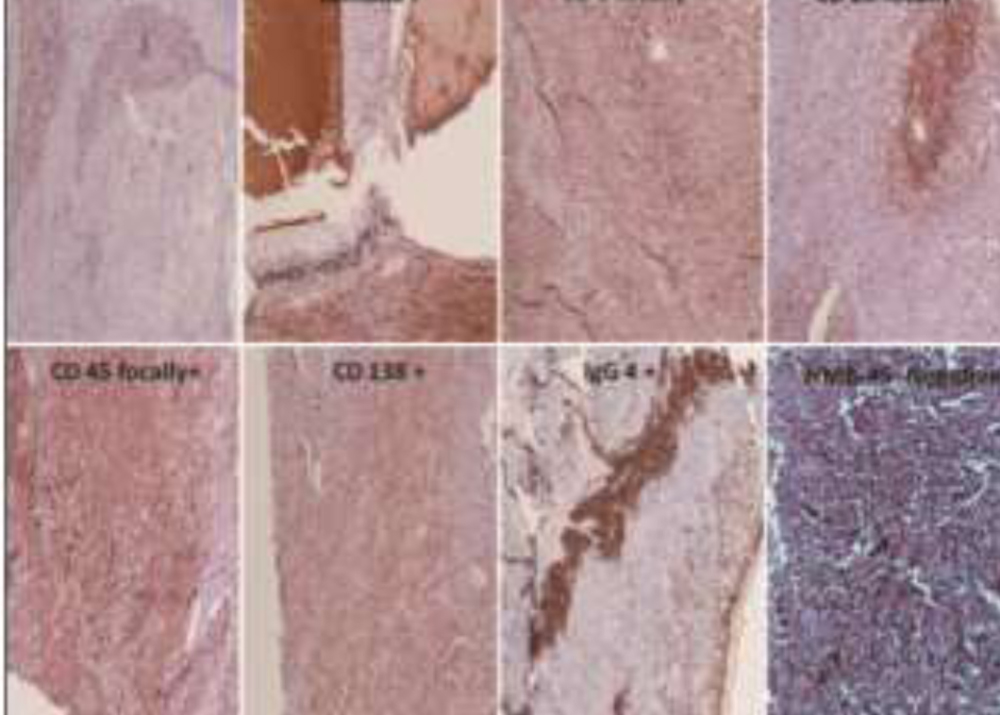
Immunohistochemistry (IHC) was advised to explore the possibility of various inflammatory lesions. The steps for IHC were carried by kit methods available commercially. IHC for both Kappa and Lambda was positive. Cluster differentiation (CD20, CD3, and CD45) was focal‑positive. CD138 was positive in the specimen and HMB45 was negative. IHC for IgG4 was positive in occasional cells which also expressed CD138 (plasma cells). All positive controls showed appropriatepositive immunostaining. Negative control slide did not show immunostaining. IgG4‑positive plasma cells were seen in high‑power field in the documented slides. Nearly, 30% of all the CD138 positive plasma cells were found to be IgG4‑positive(Fig 3). Protein chemistry revealed hypergammaglobulinemia with higher levels of total protein and gamma fraction. No myeloma band or Bence Jones protein was detected. Serum IgG4 levels were also elevated. A haematologist was consulted, and bone marrow examination revealed mild anaemia, for which she was given supportive treatment. In the postoperative period, the patient was given a course of oral steroids. On follow‑up at 6 weeks, she was given prosthesis in OD, and the patient was doing well till her last review.
Case 3
62-year-old malepresented to us with a decrease in vision in the left eye since last five days. he gave history of being diagnosed to have mediastinal liposarcoma 3 years back for which he was treated. On his presentation to us, his vision was 6/9 in the left eye. Anterior segment examination showed cataract with minimal inflammation in the anterior segment. Dilated fundus examination showed multiple choroidal lesions in the left eye(Fig 4). Visual field testing showed depression the central visual field of the left eye and the optical coherence tomography showed macular edema. Fundus fluorescein angiography showed multiple hypo fluorescent lesions in the mid AV phase with late hyper fluorescence. Electrophysiological testing of the left eye was done which showed marked reduction in the amplitude of waves in the left eye as compared to the right which was essentially normal. A diagnosis of paraneoplastic retinopathy secondary to metastasis from the mediastinal liposarcoma was made and patient put on oral immunosuppressant (mycophenolate mofetil) and oral steroids. He was referred to the oncologist for further follow up and treatment of his liposarcoma reoccurrence.
DISCUSSION
Masquerade syndrome should be considered in all patients presenting with unclear or treatment-resistant ocular inflammation. Making the right diagnosis has vital consequences for patients as most cases are malignant. Lymphomas in particular should be considered as a differential diagnosis in middle-aged patients as it is the commonest cause of masquerade syndrome. The following are necessary in order to differentiate between other causes of masquerade syndrome: a careful history, clinical examination, investigations as indicated, including ultrasound, fluorescent angiography, neuroimaging, CSF cytology and finally a vitrectomy or chorioretinal biopsy with immunohistological examination. (6) In our first case, reoccurrence of the primary malignancy coincided with a recurrence of ocular inflammation which was a vital clue.
IgG4‑RD is a systemic condition characterized by tissue IgG4‑positive lymphoplasmacytic infiltrative lesions in the body with high serum level of IgG4. IgG4‑RD is a recently proposed clinical entity with varied clinical features, but its pathogenesis remains to be understood clearly. Our second case was a 23‑year‑old female presented with sclerouveitis in OD. Ancillary imaging of OD showed ciliary body melanoma.
After enucleation, on histopathology, plasma‑lymphocytic inflammations were noted in iris and ciliary body region. No intraocular tumor was seen in the ciliary body region. On IHC, plasmacytoma was ruled out due to polyclonality in Kappa and Lambda light chain positivity. The patient in our case was younger than the normal age of presentation and presented with intraocular inflammation. Our present understanding of ophthalmic IgG4‑RD having several unique characteristic is limited to orbital and adnexal tissues.
Paraneoplastic retinopathy is usually seen with a wide range of malignancies but rarely following a liposarcoma. A liposarcoma is a malignancy of fat cells that occurs in deep soft tissue and is mostly seen in the limbs and retroperitoneum. (7) Most of the patients with liposarcoma have no symptoms until the tumor becomes large and causes pain or functional disturbances in neighbouring organs. Thus, additional experiments are needed because it is known that the ant retinal antibody can be produced not only in PR, but also in other retinal degenerative diseases as a secondary complication of retinal cell death. (8) Our experience with this case demonstrated that it is important for ophthalmologists to be aware that liposarcoma can be the cause of PR. In these cases, the visual symptoms may precede the discovery of this tumor, because liposarcoma usually grows silently in deep soft tissues without any local symptoms. The role of anti-retinal antibody as an adjunct to diagnosis needs further evaluation.
CONCLUSION
There are many entities that can present as chronic intraocular inflammation. In the absence of a correct diagnosis, inappropriate therapy may be prescribed, which can be dangerous. Malignancy and other diseases should be considered in cases of chronic uveitis that do not respond to aggressive medical therapy, and in all patients with undiagnosed inflammatory eye diseases. Direct treatment of the malignancy or underlying condition may be required to control the uveitis.
REFERENCES
1.Theodore FH. Conjunctival carcinoma masquerading as chronic conjunctivitiss. Eye Ear Nose Throat Monthly 1967; 46: 1419-1420.
2.DeAngelis LM, Yahalom J, Thaler H, et al. Combined modality therapy for primary CNS lymphoma. J ClinOncol 1992; 10: 635-643.
3.Nussenblatt RB, Whitcup SM, Palestine AG. Masquerade syndromes in uveitis: fundamentals and clinical practice. St Louis: Mosby, 1995;Chapter 29:325–33
4.Lee CS, Harocopos GJ, Kraus CL, Lee AY, Van Stavern GP, Couch SM, et al. IgG4‑associated orbital and ocular inflammation. J Ophthalmic Inflamm Infect 2015; 5:15.
5.Hammerstein W, Jürgens H, Göbel U. Retinal degeneration and embryonal rhabdomyosarcoma of the thorax. FortschrOphthalmol. 1991; 88:463–465
6.Korfel A, Thiel E, Bechrakis NE, Krause L. Masquerade Syndrome.DtschArztebl 2007; 104(8): A490–5.
7.Ferrario T, Karakousis CP. Retroperitoneal sarcomas: Grade and survival. Arch Surg. 2003; 138:248–251.
8.Kondo M, Mokuno K, Uemura A, Kachi S, Nakamura M, Kondo A et al.Paraneoplastic retinopathy associated with retroperitoneal liposarcoma. Clinical Ophthalmology 2010;4: 243–245.
Fig 2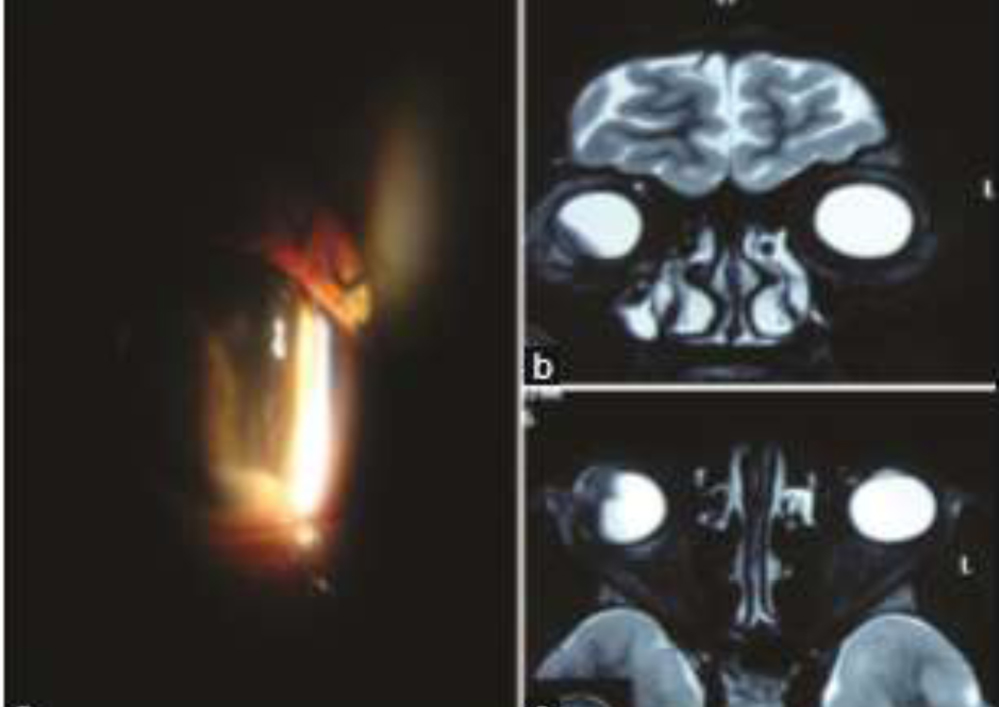
Fig 3