Dr.FalguniA Chudasama, C17993, Dr. Tejas
Himanshu Desai, Dr. Shaileen Parikh, Dr. Parul
Danayak
Abstract
Study of Comparison of outcome of Vitrectomy With & Without Internal Limiting Membrane peeling for Rhegmatogenous Retinal Detachment
Chief Author: Dr Falguni A Chudasama
Co-Authors: Dr Tejas Desai, Dr Shaileen Parikh, Dr Parul Danayak
Introduction:
The purpose of this study is to represent Internal Limiting Membrane (ILM) peeling in repair of retinal detachment due to Proliferative Vitreoretinopathy (PVR). The purpose is to analyze the effect of ILM (internal limiting membrane) peeling on anatomical and visual outcomes of vitrectomy with and without ILM (internal limiting membrane) peeling for rhegmatogenous retinal detachment, especially regarding postoperative development of epiretinal membrane.
Aims and Objectives
To analyze the effect of ILM(internal limiting membrane) peeling on the anatomical & visual outcomes in patients undergoing vitrectomy surgery for PVR related retinal detachment.
Methods:
A prospective case control study performed at Shree C.H.Nagari Eye Hospital, Ahmedabad over duration of two years. The patients were divided into two groups:
(A) Patients with Retinal detachment surgery with ILM peeling &
(B) Patients with Retinal detachment surgery without ILM peeling
Patients entered in study after obtaining an informed consent. Preoperative evaluation included detail history, best corrected visual acuity, slit lamp examination, dilated fundus examination and measurement of intraocular pressure in all patients. All patients underwent vitrectomy surgery for PVR related retinal detachment. Postoperatively, best corrected visual acuity, dilated fundus examination & Optical Coherence Tomography was taken at one & half month to assess retinal status, PVR changes & macular status to rule out any macular pucker formation. Various statistical methods were to be used to analyze the significance of the results.
Results
In Group A, the mean age of the patients was 52.36± 12.2 years and in Group B 56.7 ± 14.2 years. There are no significant differences between the two groups with regard to sex, mean duration of retinal detachment (p = 0.60), mean preoperative visual acuity (logMAR p= 0.57), and?what grade grade of proliferative vitreoretinopathy (p = 0.35) in our study.
In our study the final visual acuity (logMAR) was 1.64 +/- 0.74 in group A and 1.41 +/- 0.74 in group B (p = 0.37).Anatomic success rate (81.81%) was achieved in both the groups. In our study epiretinal membrane involving macula was found in 5 patients (22%) in Group A while 11 patients (50%) in Group B (p<0.05).
Conclusion
Internal limiting membrane peeling in vitrectomy surgery for the treatment of rhegmatogenous retinal detachment with PVR may prevent formation of epiretinal membrane without adversely affecting visual acuity.
Introduction
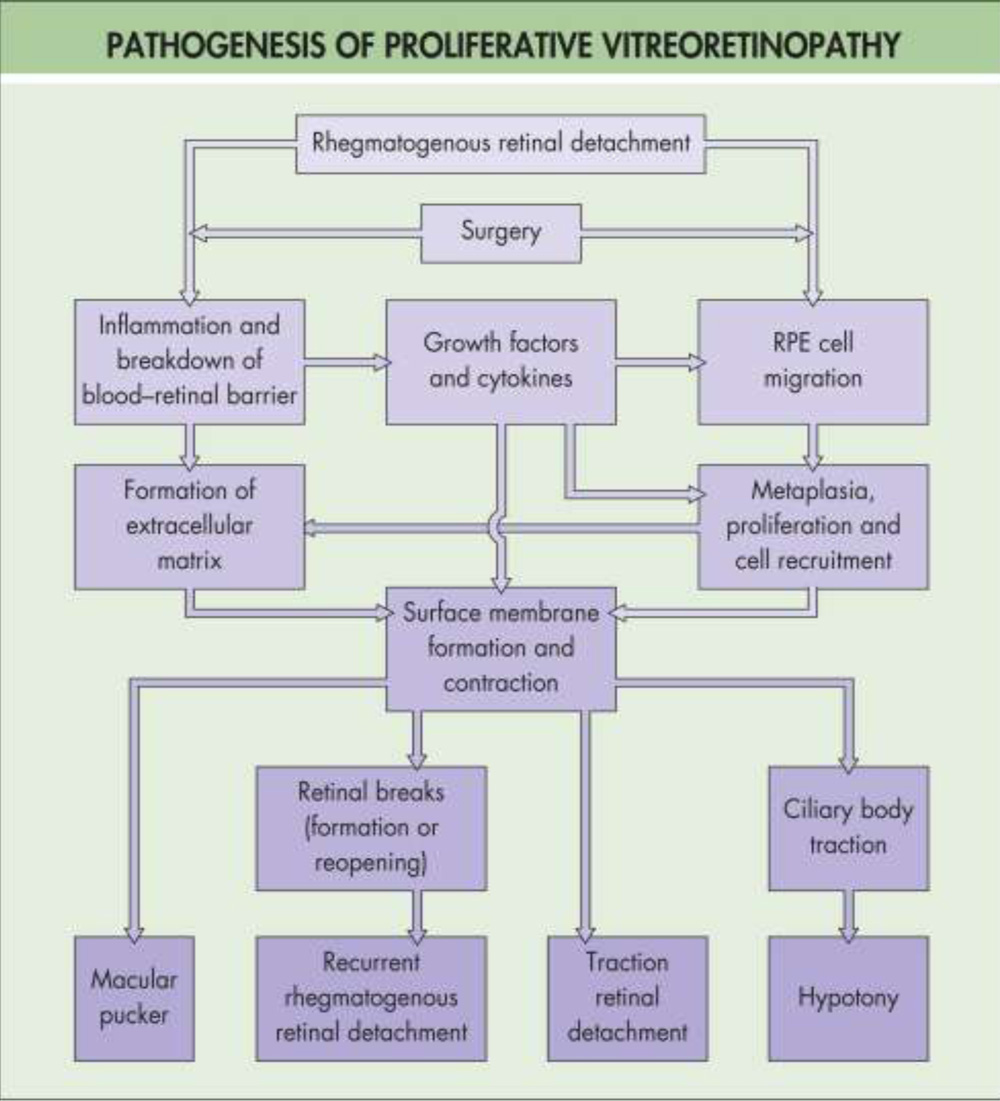
Rhegmatogenous retinal detachment is a condition in which fluid from the vitreous cavity passes through a retinal defect into the subretinal space to cause separation of the neural retina from the underlying retinal pigment epithelium (RPE). The Proliferative Vitreoretinopathy is proliferation of avascular fibrocellular retinal membranes associated with rhegmatogenous retinal detachment.
Proliferative vitreoretinopathy (PVR) is the most common cause of ultimate failure after surgical treatment for rhegmatogenous retinal detachment by reopening otherwise successfully treated retinal breaks, create new retinal breaks, and distort or obscure the macula.27
 Classification of Retinal Detachment with Proliferative Viteroretinopathy, 198327
Classification of Retinal Detachment with Proliferative Viteroretinopathy, 198327
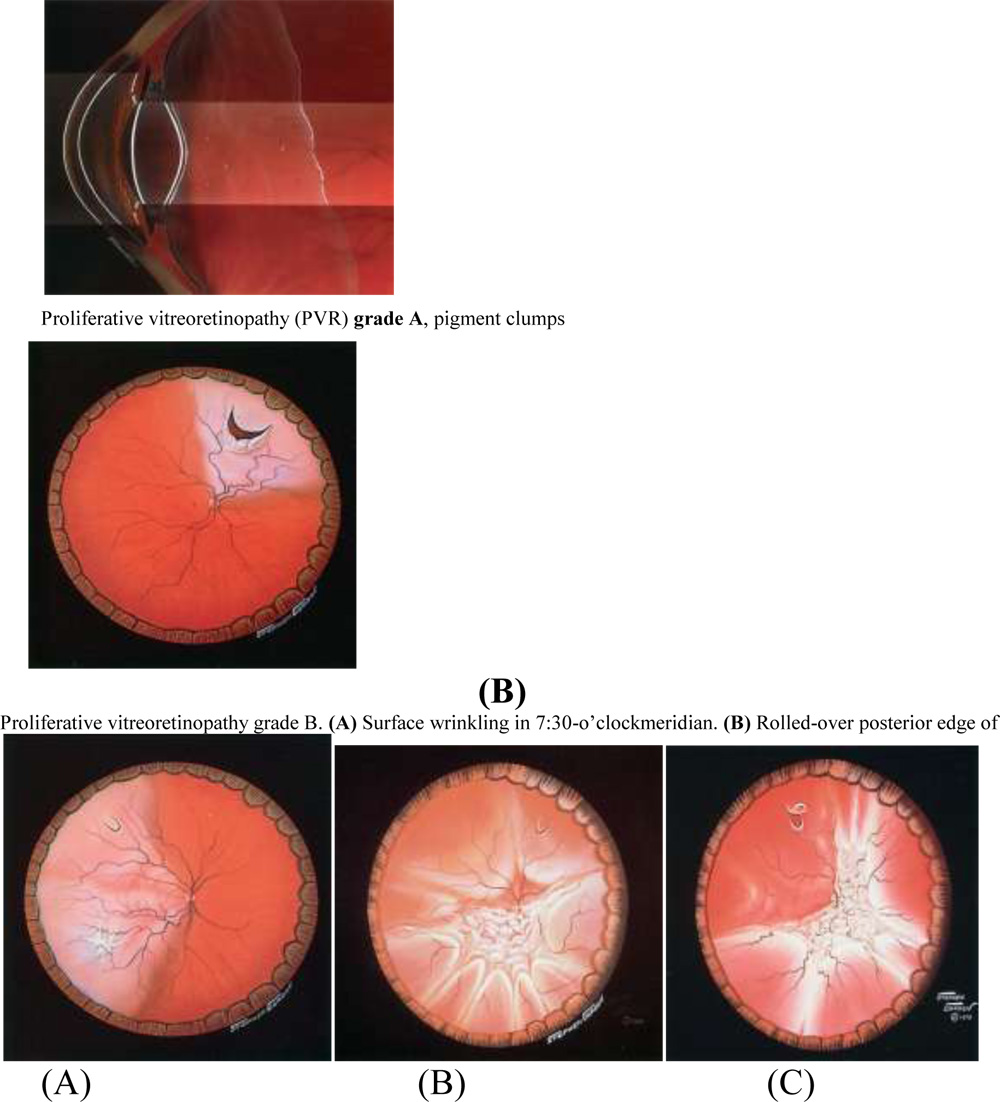 Proliferative vitreoretinopathy grade C. (A) Grade C-1, one quadrant of fullthickness
Proliferative vitreoretinopathy grade C. (A) Grade C-1, one quadrant of fullthickness
retinal folds. (B) Grade C-2, two quadrants of full-thickness retinal folds. (C) Grade
C-3, three quadrants of full-thickness retinal folds.
TREATMENT
The presence of PVR in conjunction with retinal detachment may rule out pneumaticretinopexy as the procedure of choice, and significant PVR may necessitatevitrectomy.
In the absence of open retinal breaks, PVR does not require treatment unless the macula is involved. Localized traction detachments posterior to a scleral buckle are stable and asymptomatic. However, macular pucker after otherwise successful retinal detachment surgery remains the most common cause for reduced visual acuity and distortion. Such cases often benefit from membrane peeling.
Macular Epiretinal Membranes
Iwanoff first described the abnormal proliferation of cellular membranes on the inner retinal surface in 1865.33
Since this initial description, surface proliferation in the macular region has been subsequently described as epimacular membrane, macular pucker, cellophane maculopathy, preretinal macular fibrosis, wrinkling of the internal limiting membrane, among others.34-40
Most commonly, macular epiretinal membranes (ERMs) are asymptomatic or cause mild symptoms of metamorphopsia and/or modest decreased central acuity.
A minority of these membranes can cause sufficient macular distortion and macular edema.
Epiretinal membrane formation is not uncommon following successful retinal detachment surgery, occurring in 4–8% of eyes. Retinal breaks both before and after laser or cryoretinopexy are frequently associated with subsequent retinal surface membrane proliferation .41-49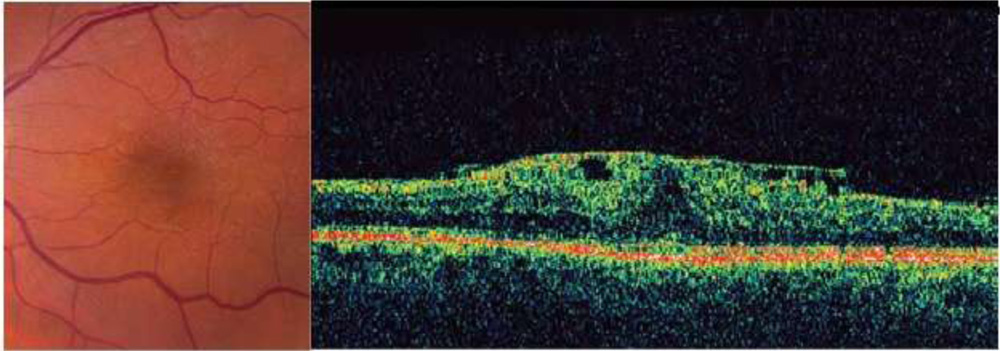 (a) ERM following cryotherapy of a peripheral retinal break. (b) OCT showing highly reflective ERM, corrugation of retinal surface, loss of foveal depression, and increased central macular thickness
(a) ERM following cryotherapy of a peripheral retinal break. (b) OCT showing highly reflective ERM, corrugation of retinal surface, loss of foveal depression, and increased central macular thickness
Foos suggested that the glial cells found in the thin, idiopathic membranes were derived from the glial cells of the superficial retina (fibrous astrocytes and Muller cells) that had migrated through breaks in the internal limiting membrane (ILM) to proliferate on the retinal surface.50
ERMs occurring following retinal breaks and detachment are felt to have a different pathogenesis. In these situations, retinal pigment epithelial (RPE) cells gain access to the vitreous cavity through the retinal break and settle on the macular surface, subsequently developing a membrane. These membranes are architecturally enhanced by the presence of fibrocytes and macrophages, stimulated in part by the inflammation associated with vitreous hemorrhage and/or surgical repair.
Most published reports on the ultrastructure of epiretinal macular membranes have been on vitrectomy specimens in elderly patients.
Vinores and colleagues studied the ultrastructural and electron immunocytochemical characterization of cells in epiretinal membranes. Their work suggests that both RPE cells and retinal glial cells are most likely to be the major participants in the pathogenesis of epiretinal membranes.51
Symptomatology: Subtle complaints of blurring of vision or metamorphopsia may develop with increasing traction, membrane opacification, or macular edema, and the onset is often insidious.
Clinical assessment: The membrane may be very fine and translucent without an identifiable edge. These may be identifiable only on careful contact lens biomicroscopy and can be as subtle as a fine ‘sheen’ in the macular region.
There may be blunting or an irregularity of the foveal light reflex. These finding may be best appreciated on red-free or monochromatic green or blue light.
More extensive membranes may take on an opaque appearance and obscure underling retinal vasculature. They may be pigmented, particularly in the case of membrane formation following the treatment of a retinal break or retinal detachment, severe intraocular inflammation, or vitreous hemorrhage.51-53
OCT can play an important role in the clinical assessment of eyes with ERMs.
OCT can not only detect ERMs, but also assist in topographic localization, identification of vitreoretinal relationships (such as in the vitreomacular traction syndrome), detection of macular holes, and quantitation of macular thickness and macular volume.
In addition to value in clinical characterization, OCT has therapeutic value in preoperative planning. The co-existence of a macular hole, the presence of a bilaminar ERM, or knowledge of substantive macular edema may lead the surgeon to modify his or her approach.
It also has considerable prognostic value in counseling patients as to the eye’s likely visual potential.
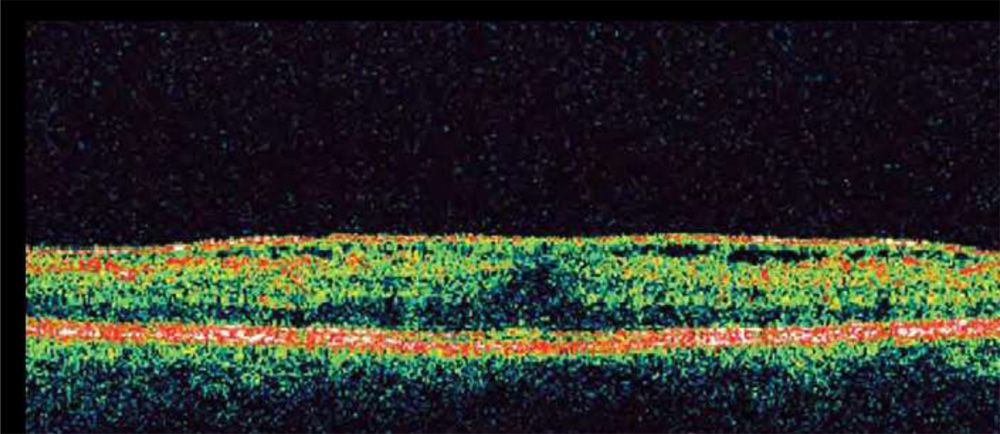 Fig. OCT showing typical ERM features including highly reflective ERM, multiple points of retinal attachment, loss of foveal depression, and increased retinal thickness.
Fig. OCT showing typical ERM features including highly reflective ERM, multiple points of retinal attachment, loss of foveal depression, and increased retinal thickness.
Treatment
It is impossible to predict for any patient what will be the course of any specific ERM. This renders decisions difficult regarding surgery and the timing of surgery. In cases with significant or progressive vision loss, debilitating metamorphopsia or diplopia, surgical intervention should be considered.
Role of Internal Limiting Membrane Peeling:
Because of its rigidity, the internal limiting membrane is considered a significant source of retinal stiffness, especially in posterior pole disease.55,56
A minimally destructive form of retinal dissection, ILM peeling, is commonly and successfully employed for release of retinal tension in a variety of posterior pole diseases.
Intraoperative tissue staining is widely used for optimum visualization in ILM peeling when complete and thorough posterior pole ILM removal is thought to be critical to the surgery’s success.57-59
Indocyanine green-assisted ILM peel has been described in many ocular disease states, including macular hole repair, repair of staphylomatous posterior pole retinal detachments, macular hole-related retinal detachments, myopic traction maculopathy, and epiretinal membrane prevention in retinal detachments.60-67
Further, it is now frequently employed in diabetic macular edema which is recalcitrant to focal laser photocoagulation and intravitreal antivascular endothelial growth factor or anti-inflammatory therapy, and is thought to have a mechanical effect.68-71
A recent study focusing on optical coherence tomography findings in patients who underwent ILM peeling in conjunction with PVR-retinal detachment repair demonstrates that the technique is now also being adapted for difficult retinal detachment cases.72
ILM peeling of the posterior pole is a non-standard approach to PVR detachments, and is not represented well in the literature.
The rationale for its use is based on other well studied surgical applications in posterior pole diseases, such as macular pucker and macular hole.
Theoretically, ILM peeling reduces retinal tension transmitted to the posterior pole. Removal of this tensile layer offers the mechanical advantage of relaxing the surface tractional forces.
It increases retinal compliance by the creation of a central “soft spot”, which allows adjacent areas to relax better.
ILM removal can also create a plane by which to undermine and dissect PVR,73especially if it is posteriorly located.
Additionally, it reduces the likelihood of recurrence of posterior epiretinal membrane/PVR formation67 and subsequent redetachments, while maximizing macular visual function.
INTERNAL LIMITING MEMBRANE PEEL
Techniques for removal of the ILM involve establishing an elevated edge of the ILM and then peeling the ILM from around the macula.
Establishing an initial edge may be accomplished with the use of a barbed microvitreoretinal blade74or with the use of fine intraocular end-grasping forceps to ‘pinch’ and elevate the ILM.75
The ILM peel is most often performed in a circular motion around the macula (‘maculorhexis’)
The identification and peeling of the ILM is technically challenging. Adjuvants to improve visualization of the ILM include indocyanine green dye (ICG), trypan blue dye, and triamcinolone acetonide.
Indocyanine green dye is instilled onto the surface of the retina in an air-or fluid-filled eye. The ICG selectively stains the ILM, and the ILM may be more easily identified and elevated with the use of diamond-dusted silicone cannula or with fine end-grasping forceps.
Retinal and retinal pigment epithelial toxicity76–78 have been reported and questions have arisen about potentially diminished visual acuity in eyes exposed to intravitreal ICG dye.79
Others report excellent results with the use of adjunctive-ICG without evidence of toxicity.80 No randomized, prospective trials have been performed.
Trypan blue stains both the ILM and epiretinal membranes.
The staining of the ILM is less intense than the staining achieved with ICG.81,82 There have been no reports of toxicity associated with trypan blue.
Triamcinolone acetonide can be injected intraoperatively onto the surface of the macula. While it does not stain the internal membrane, it adheres to the surface and may facilitate identification of the ILM.83,84
Brilliant blue dye stains ILM. More intense than staining achieved by trypan blue.95
AIMS AND OBJECTIVES
To analyze the effect of ILM (internal limiting membrane) peeling on the anatomical & visual outcomes in patients undergoing vitrectomy surgery for PVR related retinal detachment.
REVIEW OF LITERATURE
- Girard P, Mimoun G, et al studied “Clinical risk factors for proliferative vitreoretinopathy after retinal detachment surgery,” published in Retina, in 1994 vol 14. Purpose of their study was to identify the clinical risk factors for the development of severe proliferative vitreoretinopathy (PVR) after retinal detachment surgery.93
Girard P1, Mimoun G, et al “Clinical risk factors for proliferative vitreoretinopathy after retinal detachment surgery,” published in Retina, in 1994 vol 14.
It was a retrospective study of 1020 patients with either no PVR or with PVR of grade C1 or less at initial examination was conducted. After surgery, severe PVR was defined as grade C2 or worse. Severe PVR developed after surgery in 107 patients (10.5%). The results indicated that in addition to the size of breaks, extent of detachment, and presence of preoperative inflammation or low-grade PVR, iatrogenic problems also were important factors in the pathogenesis of severe PVR after surgery for retinal detachment.
Odrobina D, Bednarski M et all did study “Internal limiting membrane peeling as prophylaxis of macular pucker formation in eyes undergoing retinectomy for severe proliferative vitreoretinopathy,” Published on Feb 2010 in Retina.89
Odrobina D, Bednarski M, Cisiecki S, Michalewska Z, Kuhn F, et al. Internal limiting membrane peeling as prophylaxis of macular pucker formation in eyes undergoing retinectomy for severe proliferative vitreoretinopathy. Published on Feb 201in Retina ;32(2):226-31. doi: 10.1097/IAE.
The purpose of their study was to analyze the effect of internal limiting membrane (ILM) peeling on the anatomical and functional outcomes in patients having proliferative vitreoretinopathy-related retinal detachment, especially regarding the postoperative development of macular pucker.
It was consecutive and prospective stud of 84 patients. All eyes underwent retinectomy with silicone oil tamponade for retinal detachment because of proliferative vitreoretinopathy. In Group A (33 eyes), the ILM was also peeled; in Group B (51 eyes), the ILM was left intact. Median follow-up in Group A was 28.2 ± 7.2 months and in Group B 27.4 ± 6.5 months.
They found that Primary peeling of the ILM allowed complete removal of all the epiretinal membranes and successfully prevented the development of pucker.
- Aras C, Arici C et all studied “Peeling of internal limiting membrane during vitrectomy for complicated retinal detachment prevents epimacular membrane formation,” Published on may 2009 in Graefes Arch Clin Exp Ophthalmolology.90
Aras C, Arici C, Akar S, Müftüoglu GYolar MArvas, et al. Peeling of internal limiting membrane during vitrectomy for complicated retinal detachment prevents epimacular membrane formation. Published on may 2009 in Graefes Arch Clin Exp Ophthalmol.;247(5):619-23. doi: 10.1007/s00417-008-1025-y.
The purpose of their study was to investigate the clinical benefit of internal limiting membrane (ILM) peeling at the macula for the prevention of epimacular membrane formation following vitreous surgery using silicone oil for the treatment of complicated retinal detachment.
Method was a non-randomized, retrospective, interventional study of a case series. Patient charts were reviewed retrospectively for 20 consecutively recruited patients who underwent successful primary vitrectomy with ILM peeling at the macula using silicone oil (group 1) and 22 consecutively recruited patients who underwent successful primary vitrectomy using silicone oil without ILM peeling at the macula for complicated rhegmatogenous retinal detachment (group 2). The mean follow-up time was 24.6 +/- 7.6 weeks in group 1 and 34.1 +/- 12.6 weeks in group 2 (p = 0.01).
The main outcome measures were distant visual acuity and epimacular membrane formation. The data were analyzed and compared using Fisher’s Exact test, Pearson Chi-square test, independent t-test, Mann-Whitney U-test, and a repeated ANOVA. They found that ILM peeling at the macula during vitreous surgery with silicone oil for the treatment of complicated retinal detachment may prevent epimacular membrane formation without negatively affecting distant visual acuity.
- Odrobina DC, Michalewska Z et all studied, “High-speed, high-resolution spectral optical coherence tomography in patients after vitrectomy with internal limiting membrane peeling for proliferative vitreoretinopathy retinal detachment,” Published on june 2010 in 91
Odrobina DC, Michalewska Z, Michalewski J, Nawrocki J et al. High-speed, high-resolution spectral optical coherence tomography in patients after vitrectomy with internal limiting membrane peeling for proliferative vitreoretinopathy retinal detachment. Published on june 2010 in Retina. 30(6):881-6. doi: 10.1097/IAE.0b013e3181c96952.
The purpose of their study was to present the retinal morphology after silicone oil removal in patients after vitrectomy with internal limiting membrane peeling and silicone oil tamponade for proliferative vitreoretinopathy retinal detachment.
Nineteen patients after vitrectomy or retinotomy with internal limiting membrane peeling for proliferative vitreoretinopathy retinal detachment were included in this study. All patients were interviewed, and an ophthalmologic examination was performed pre- and postoperatively. Fifteen months after silicone oil removal, all patients were examined with spectral optical coherence tomography Copernicus.
They found that Spectral optical coherence tomography Copernicus allows detailed imaging of retinal microstructure and helps us understand why patients have lowered visual acuity after successful retinal detachment surgeries.
It is suspected that the absence of macular pucker may be caused by systematic peeling of the internal limiting membrane during vitrectomy.
- John R Minarcik et all studied, “Virtual retinectomy: indocyanine green-assisted internal limiting membrane peeling as a surgical adjunct in repair of recurrent rhegmatogenous retinal detachment due to PVR,” Published on 24 april 2012 in Dove press journal Clin Ophthalmol.92
John R Minarcik, Manfred A von Fricken. Virtual retinectomy: indocyanine green-assisted internal limiting membrane peeling as a surgical adjunct in repair of recurrent rhegmatogenous retinal detachment due to PVR. Published on 24 april 2012 in Dove press journal. Clin Ophthalmol. 2012;6:631-6. doi: 10.2147/OPTH.S29654.
The purpose of their study was to describe and evaluate a surgical approach, known as internal limiting membrane (ILM) peeling, as an adjunct to repair of recurrent retinal detachment due to proliferative vitreoretinopathy (PVR).
This was a retrospective case series. All eyes underwent repair of recurrent PVR-related rhegmatogenous retinal detachment incorporating macular indocyanine greenassisted ILM peeling.
Fourteen eyes from 14 patients were included with a minimum follow up period of 6 months. Anatomic success with single surgery was achieved in 11 of 14 (79%) of the operated eyes using this technique, and eventual success was achieved in all eyes (100%). Among the failed repairs prior to ILM peeling, 8/14 eyes had scleral buckles, 7/14 had silicone oil tamponade, and two had inferior retinectomies. There was no subsequent development of epiretinal membranes after ILM peeling.
They found that ILM peeling in conjunction with vitrectomy and peeling of peripheral membranes is an effective technique with a high anatomic success rate in the challenging scenario of PVRrelated recurrent detachments. They described the technique as an alternative to the traditional retinectomy.
- Moon Soo Heo, Hyun Woong Kim, et al published “The Clinical Features of Macular Pucker Formation after Pars Plana Vitrectomy for Primary Rhegmatogenous Retinal Detachment Repair” in Korean j ophthalmology, 2012 oct; 26(5); 355-361.94
Moon Soo Heo, Hyun Woong Kim, et al published “The Clinical Features of Macular Pucker Formation after Pars Plana Vitrectomy for Primary Rhegmatogenous Retinal Detachment Repair” in Korean j ophthalmology, 2012 oct; 26(5); 355-361.
The purpose of their study was to investigate the incidence and predisposing factors of macular pucker formation after pars plana vitrectomy in patients who developed primary rhegmatogenous retinal detachment.
They retrospectively reviewed a consecutive series of 284 eyes in 284 patients who underwent primary retinal detachment repair by pars plana vitrectomy alone between January 1, 2009 and December 31, 2010.
In this study, 6.1% of eyes which underwent pars plana vitrectomy alone for primary retinal detachment developed a postoperative macular epiretinal membrane. Overall, the 70.0% of eyes which underwent secondary vitrectomy with membrane peeling for removal of macular pucker showed a favorable visual outcome.
Ø Prashant Naithani, Naginder Vashisht et al published, “Brilliant blue G-assisted peeling of the internal limiting membrane in macular hole surgery” in Indian J Ophthalmol, 2011 Mar-Apr; 59(2): 158–160. 95
Prashant Naithani, Naginder Vashisht et al published, “Brilliant blue G-assisted peeling of the internal limiting membrane in macular hole surgery” in Indian J Ophthalmol, 2011 Mar-Apr; 59(2): 158–160.
They performed a 23-gauge pars plana vitrectomy with brilliant blue G-assisted ILM peeling in six patients with idiopathic macular holes, to assess the staining characteristics and short-term adverse effects of this dye.
Adequate staining assisted in the complete removal of ILM and closure of macular holes in all cases. There was no evidence of intraoperative or postoperative dye-related toxicity. Brilliant blue G appears to be safe dye for ILM staining in macular hole surgery
Materials and Methods
- A prospective case control study being performed at Shree C.H.Nagari Eye Hospital, Ahmedabad from January 2013 to 30 august 2014.
- Sample size 44 patients divided in two groups
- Group A : Retinal detachment surgery with ILM peeling (22 patients)
- Group B : Retinal detachment surgery without ILM peeling (22 patients)
- Patients entered in study after obtaining an informed consent.
- Detailed Clinical History was taken preoperatively.
- Preoperative evaluation included best corrected visual acuity, slit lamp examination, and measurement of intraocular pressure in all patients.
- Dilated fundus examination was carried out using binocular indirect ophthalmoscope with indentation & extent of detachment including PVR grading was noted.
- Fundus photo, OCT (Optical Coherence Tomography) was taken.
- After surgery, follow-up of patients was done at one & half month postoperatively.
- The corrected visual acuity, fundus examination and OCT was taken & included in the statistical analysis
Inclusion / Exclusion criteria
Inclusion criteria
- Rhegmatogenous Retinal Detachment with proliferative vitreoretinopathy grade B, C1 & C2
- Recurrent Retinal Detachment with PVR grade <C3
Exclusion criteria
- Tractional / Exudative Retinal Detachment
- Retinal Detachment with macular hole
- Retinal Detachment with grade D proliferative vitreoretinopathy
Surgical Technique
- Conjunctival peritomy done 360 degree.
- Belt Buckle will be passed through four partial thickness sclera tunnels & tied in superotemporal quadrant location estimated as lying about 2–3 mm posterior to an imaginary line drawn between the muscle insertions. ( Optional)
- 23-gauge pars plana vitrectomy done including core vitrectomy & peripheral vitrectomy with Close vitreous base shaving with external scleral depression to be performed & complete vitrectomy done by triamcinolone staining.
- Brilliant blue staining of the posterior pole accomplished with several brief directed pulses of dye around the macula with a soft tip catheter with avoidance of the fovea.
- Peeling and removal of any visible PVR membranes and bands will be also performed in all cases prior to ILM (internal limiting membrane) removal.
- The staining followed by prompt and complete removal of the dye with the cutter on aspiration mode.
- After effective staining, ILM dissection initiated in the posterior pole with end-grasping forceps, and carried out as far as possible, to the arcades or beyond, if necessary.
- Air Fluid exchange done. Retina settled.
- Breaks were sealed either with endolaser or cryo.
- After subretinal fluid drainage, tamponade will be accomplished with either 12% C3F8 or 1000 cst silicone oil.
The main outcome measures:
1) Anatomic success rate using single surgery.
2) Distant visual acuity using snellen’s distant visual acuity chart.
3) Epiretinal Membrane (ERM) formation & macular pucker formation : To define ERM, we have used clinical biomicroscopy and Optical Coherence Tomography (OCT)
Statistical analysis
Appropriate statistical test like mean, SD, range are applied for descriptive purpose and for drawing inference of collected data tests of significance like paired and unpaired t test, correlation coefficient are applied with the help of biostatistician.
OBSERVATIONS AND RESULTS
A prospective case control study was performed on 44 patients at Shree C.H.Nagari Eye Hospital, Ahmedabad.
TABLE 1
| GROUP | No. of Patients |
| A ( Vitrectomy + Ilmp) | 22 |
| B ( Vitrectomy without Ilmp) | 22 |
Patients were equally divided between Group A (Retinal detachment surgery with ILM peelin) &Group B (Retinal detachment surgery without ILM peeling).
TABLE 2
SEX DISTRIBUTION
| SEX | A ( Vitrectomy + Ilmp) | B ( Vitrectomy without Ilmp) | Total No. |
| MALE | 17 (77.3%) | 14 (63.63%) | 31 (70.45%) |
| FEMALE | 5 (22.72%) | 8 (36.36%) | 13 (29.54%) |
| TOTAL | 22 | 22 | 44 |
Out of 44 patients 31 patients were male & 13 patients were female
TABLE 3 ( Age Distribution)
| GROUP A | GROUP B | |
| Mean Age | 52.36 | 56.7 |
| Standard deviation | 12.2 | 14.2 |
In Group A, the mean age of the patients was 52.36± 12.2 years and in Group B 56.7 ± 14.2 years. ( P value 0.1170 calculated by using Mann Whitney Test, statistically not significant).
TABLE 4 ( Lens Status)
| LENS STATUS | Group A | Group B | Total |
| Pseudophakia | 16 (72.7%) | 17 (77.27%) | 33 (75%) |
| Aphakia | 0 | 1 (4.5%) | 1 (2.3%) |
| Phakic | 6 (27.27%) | 4 (18.18%) | 10 (22.7%) |
| Total | 22 | 22 | 44 |
In Both the groups Majority of patients were having pseudophakia which came out to be 75% of total paients.
TABLE 5 Etiological Factor
| Causative Factor | Group A
(No of patients) |
Group B
(No of patients) |
| Cataract surgery | 16 (72.7%) | 18 (81.81%) |
| Myopia | 6 (27.3%) | 5 (22.7%) |
| Blunt Trauma | 3 (13.6%) | 4 (18.2%) |
So, history of complicated cataract surgery was the most common factor responsible for retinal detachment in both the groups. Myopia and trauma were the next two common causes followed by cataract surgery.
TABLE 6
Duration of Retinal Detachment in days
| Group | A | B |
| Mean Days | 20.5 | 19.81 |
| Standard deviation | 8.5 | 11.31 |
P value calculated using Mann whitney Test 0.60 (No significance difference between two groups)
There are no significant differences between the two groups with regard to mean duration of retinal detachment (p = 0.60) as mentioned in table 6.
TABLE 7
Preoperative vision in logMAR
| Group | A | B |
| Mean vision | 2.68 | 2.59 |
| Standard deviation | 0.28 | 0.38 |
P value calculated using unpaired t test is 0.578 which is suggestive of no significance difference between two groups
There are no significant differences between the two groups with regard to mean preoperative visual acuity (logMAR p= 0.57) as mentioned in table 7.
TABLE 8
PVR Grade
| No of patients | Group A | Group B |
| PVR grade B | 17 | 18 |
| PVR grade C | 5 | 4 |
There is no major difference between two groups with regards to proliferative vitreoretinopathy grade as shown in table 8
Table 9
Endotemponade Used
| Endotemponade | GROUP A | GROUP B | Total |
| 12% C3F8 | 9 | 5 | 14 |
| Silicone Oil | 13 | 17 | 30 |
| Total | 22 | 22 | 44 |
Patient distribution depending on the type of endotemponade used is shown in table 9.
Table 10
Area of ILM peeling & PVR Grade
| Area of peeling | Grade B
No of patients |
Grade C
No of patients |
Total no of patients |
| 2 Disc diameter | 5 | 4 | 9 |
| 3 Disc diameter | 10 | 3 | 13 |
Intra operative area of ILM peeling was noted down to know any correlation between area of peeling and surgical outcome. Table10 shows no of patients having different area of peeling.
ANALYTICAL DATA
- Data tabulation was performed on Microsoft-excel worksheets. Statistical analysis was done using Graph Pad InStat-3 software.
- Comparison between pre-operative and post-operative values in individual groups was analysed using PAIRED T TEST (in data following normal distribution) and WILCOXON MATCHED PAIRS TEST (in data not following normal distribution).
- While comparison between the groups for all variables was done using Mann- Whitney Test & Chi square test.
- A “p” value ≤ 0.05 was considered statistically significant.
Table 11
Comparison of preop & postop Visual acuity (VA)
(At 6 weeks postop)
(in Log MAR)
| Group | Preop VA
(Mean) |
Postop VA
(Mean) |
P value |
| A | 2.68 | 1.64 | <0.0001 |
| B | 2.59 | 1.41 | <0.0001 |
| Total patients | 2.63 | 1.53 | <0.0001 |
P values were calculated using wilcoxon matched paired test which is <0.0001 which is highly significant is suggesting that improvement in visual outcome in both the groups is statistically significant.
Table 12
Comparison of final visual outcome between two groups
(At 6 weeks postop)
(in Log MAR)
| Group A | Group B | |
| Mean VA | 1.64 | 1.41 |
P value 0.37
P value was calculated using Mann-Whitney Test which came out to be 0.37 which is not significant.
It is suggesting that internal limiting membrane peeling procedure is not negatively affecting visual outcome.
Table 13
Comparison of Anatomical Success Rate at 6 weeks postop
| Group | % Patients with of Retina on |
| A | 81.81% |
| B | 81.81% |
Both the groups have same anatomical success rate which is suggesting that ILMP is not inadvertently affecting anatomical success rate.
Table 14
No of Patients Developing ERM at 6 weeks postop
| Group | No of patients having ERM | % of patients having ERM |
| A | 5 | 22.72% |
| B | 11 | 50% |
Chi square test was applied to find out p value which was 0.05 suggestive of significance of the difference between two groups.
It is suggesting that internal limiting membrane peeling procedure reduces rate of epiretinal membrane formation in patients following retinal detachment surgery.
Table 15
ILM peeling area affecting vision & ERM formation at 6 week postop
| Area of peeling | No of patients | Mean VA | No of patients having ERM |
| 2 Disc diameter | 9 | 1.61 | 3 (33.33%) |
| 3 Disc diameter | 13 | 1.66 | 2 (15.38%) |
Visual outcome is not affected by area of peeling of ILM as p value is 0.92 calculated by Mann Whitney Test which is not statistically significant.
Table 16
| Mean vision | Mean CFT | |
| Patients having ERM | 1.60 | 269.43 |
| Patients not having ERM | 1.39 | 247.75 |
Visual outcome in patients developing ERM is compared with patients not developing ERM. P value calculated using Mann Whitney Test is 0.21 which is not significant.
Same way there is no major difference in central foveal thickness on optical coherence tomography where P value comes 0.47, again statistically not significant.
Table 17
Complications
| No of patients | Group A | Group B |
| Iatrogenic Break | 3 | 1 |
| Redetachment | 3 | 3 |
| Full thickness macular hole | 1 | 1 |
| Corneal edema | 0 | 2 |
| Progressive cataract | 1 | 2 |
| Raised intra ocular pressure | 1 | 2 |
Apart from expected routine complications of vitrectomy such as progressive cataract formation, raised intra ocular pressure & redetachment the major complication in group A was iatrogenic break formation while ILM peeling procedure.
All 3 patients who developed iatrogenic extramacular break were lasered on table, but still one patient developed redetachment at six weeks postop.
All patients with redetachment required second surgery to re attach retina with silicone oil endotemponade.
DISCUSSION
- In our study, in Group A, the mean age of the patients was 52.36± 12.2 years and in Group B 56.7 ± 14.2 years. ( P value 0.1170, statistically not significant) & it is comparable to similar studies performed by Odrobina D, Bednarski M et al & Aras C, Arici C et al.
- Using ILM peeling in conjunction with vitrectomy and peeling of peripheral membranes is an effective technique with a high anatomic success rate (81.81%) in our study in the challenging scenario of PVR-related recurrent retinal detachments.
It is comparable with study performed by John R Minarcik et al, “Virtual retinectomy: indocyanine green-assisted internal limiting membrane peeling as a surgical adjunct in repair of recurrent rhegmatogenous retinal detachment due to PVR,” Published on 24 april 2012 in Dove press journal Clin Ophthalmol.92where they achieved 79% anatomical success rate.
- There are no significant differences between the two groups with regard to sex, mean duration of retinal detachment (p = 0.60), mean preoperative visual acuity (logMAR p= 0.57), and grade of proliferative vitreoretinopathy (p = 0.35) in our study.
It is compared with study performed by Arac C et al, “Peeling of internal limiting membrane during vitrectomy for complicated retinal detachment prevents epimacular membrane formation.” In which there was no significant difference between these factors.
- All patients in both groups gained improvement in vision from mean logMAR preoperative vision of 2.63 to 1.53 ( p value <0.0001) which is statistically significant.
In our study the final visual acuity (logMAR) was 1.64 +/- 0.74 in group A and 1.41 +/- 0.74 in group B (p = 0.37) so that we can comment that internal limiting membrane peeling procedure is not negatively affecting visual outcome or anatomical success rate.
These visual outcome is compared with study performed by Odrobina D et al where the mean logarithm of the minimum angle of resolution visual acuity at the final follow-up visit was 1.89 ± 0.87 in Group A ( with ILMP) and 1.85 ± 0.83 in Group B(without ILMP) (P = 0.6, t-test).
It is also comparable to study done by aras c et al where the final visual acuity (logMAR) was 0.60 +/- 0.30 in group 1 and 0.72 +/- 0.35 in group 2 (p = 0.49).
- In our study epiretinal membrane involving macula was found in 5 patients (22%) in Group A while 11 patients (50%) in Group B. This data showed significant increase in the rate of ERM at post-op 6 weeks in Group B (P=0.05).
It is comparable to other studies also. In study performed by Odrobina D, Bednarski M et al no case of macular pucker was observed in Group A, but macular pucker was observed in 9 eyes (17.6%) in Group B at the final examination (P = 0.008, Fisher exact test).
In another study performed by Aras C, Arici C et al epimacular membrane formation was observed in six eyes in group 2 (without ILMP) where as no epimacular membrane formation was seen in group 1 (with ILMP) (p = 0.02).
- Correlation between area of internal limiting membrane peeling & formation of epiretinal membrane is not mentioned in literature. In our study we found that Epiretinal membrane formation & Visual outcome is not affected by area of peeling of ILM as p value is 0.92(statistically not significant).
- Same way epiretinal membrane formation is not associated with increase in central foveal thickness (p value 0.47) or any major difference in visual outcome (p value 0.21) in our study. These factors are also not well mentioned in other studies. However mean follow up in our study is only 6 weeks.
- In group A while doing internal limiting membrane peeling intra operatively three patients developed extramacular iatrogenic breaks which were lasered on table. One patient out of these three developed redetachment for which re surgery was required at six weeks postop.
- One patient developed full thickness macular hole with subretinal fluid & another two patients developed redetachment due to unknown cause. This redetachment rate was comparable to group B were also 4 patients developed redetachment at 6 weeks postop. Out of these four patients in group B one had full thickness macular hole.
CONCLUSION
- There are no significant differences between the two groups with regard to mean age (p=0.11), sex, mean duration of retinal detachment (p=0.60), mean preoperative visual acuity (logMAR p=0.57), and grade of proliferative vitreoretinopathy (p=0.35).
- The final visual acuity (logMAR) was 1.64 +/- 0.74 in group A and 1.41 +/- 0.74 in group B (p=0.37) so that we can comment that internal limiting membrane peeling procedure is not negatively affecting visual outcome or anatomical success rate (81.81% in both groups).
- There is significant increase in the rate of ERM formation at post-op 6 weeks in Group B (PPV without ILM peeling) (P=0.05)
- Epiretinal membrane formation & Visual outcome is not affected by area of peeling of ILM as (p=0.92)(statistically not significant).
- Epiretinal membrane formation is not associated with increase in central foveal thickness (p=0.47) or any major difference in visual outcome (p=0.21) in our study.
- Internal Limiting Membrane peeling during vitrectomy surgery in Rhegmatogenous Retinal Detachment has significantly reduced rate of epiretinal membrane formation when compared with control group without any significant difference in visual outcome or anatomical success rate.
Proforma for comparison of outcome of Vitrectomy with & without ILM Peeling for Rhegmatogenous Retinal Detachment