Dr. Haard Shah, S17850, Pradeep Susvar, Dr. Pramod Sadashiorao Bhende, Dr.Kushal S Delhiwala
Introduction
Complete attachment of the complicated retinal detachment (RD) due to any etiology is the most challenging task for the retinal surgeon. One of the most common reason for such difficulty is the presence of proliferative vitreoretinopathy (PVR). Retinal detachment of any etiology induces cellular reaction and proliferation which is responsible for PVR development. These type of response caused contractile pre-retinal and/or sub retinal membranes. The main purpose of the surgery in complex retinal detachment specially with anterior PVR is to stabilize the posterior retina, thereby facilitating the patient to achieve maximum functional outcome. In such situations of circumferential and anterio-posterior traction, additional step of relaxing retinectomy (RR) can be performed during vitrectomy to relieve such traction, after stabilizing posterior pole with per-carbon liquid ( PFCL). With the background of very few literature discussing complete 360 degree RR, we present this study on a large series of peripheral 360 degree relieving retinectomy performed for complicated retinal detachment- its indications and outcome.
Materials and Methods
Hundred and one eyes of 100 patients were reviewed retrospectively in which360 degree RR was performed during complicated RD surgeries. All the surgical procedures were done between years 2010 to 2014 by four retinal surgeons having minimum experience of 10 years in single tertiary eye centre.
Inclusion criteria:
- Complex retinal detachment of all etiologies requiring intraoperative 360 degree relaxing retinectomy.
Exclusion criteria:
- Follow-up less than 6 weeks visit
All patients underwent complete pre- and postoperative examinationsincluding best corrected visual acuity (BCVA), intraocular pressure (IOP) assessment, slit lamp bio microscopy, indirect ophthalmoscopy and ultrasonography (USG) if fundus was not visible. Anatomical outcome was defined as retinal status at each post-operative follow-up. Visual recovery was defined as post-operative BCVA improved by one line compared to pre-op BCVA. Total attachment was defined as attached retina without any edge lift. Partial retinal detachment (recurrence) was defined as edge lift/ retinal detachment without macular involvement. Total retinal detachment (recurrence) was defined as recurrence involving Macula. Hypotony was defined as IOP ≤ 5 mm Hg and increased IOP as ≥ 22 mm Hg. BCVA > 3/60 was considered as ambulatory vision. Postoperative assessment included complete anatomical reattachment of retina and macula, the need for re-surgeries for recurrences, anterior segment complications and whether silicone oil was removed or not.
Surgical technique
All eyes underwent standard 3-port 20 or 23 gauge pars plana vitrectomy utilizing non-contact wide angle viewing system. Choice of gauge was based on surgeon’s discretion. Lensectomy was performed in selected cases based on adequacy of peripheral retinal visualization and manipulation as well in eyes with associated total cataract. Intraocular lens was left in place for pseudophakic eyes. After thorough vitreous base shaving, extensive membrane peeling was done with conventional techniques and using perfluoro n-octane injection to assess residual traction. The decision to proceed for 360° RR was made after noticing persistent retinal traction in spite of maximum membrane removal and in eyes where retinal incarceration or intrinsic contraction prevented settling of retina. In all cases, endodiathermy was applied to margins of peripheral retina from where it was to be cut in order to prevent bleeding. RR was performed with microvit along with removal of non-functional anterior retina. Once the traction was relieved, PFCL was injected to flatten the retina. Endolaser photocoagulation was done in 4-5 rows posterior to the margins of 360° RR taking care not to go near to optic disc and macula in case very posterior RR. Inferior iridectomy was made with microvit cutter in cases where lensectomy was performed. Direct PFCL -silicone oil exchange was performed under visualization. The choice of 1300 Cst or 5500 Cst silicone oil tamponade was based on surgeon’s discretion.
Results
The study included 101 eyes of 100 patients. One patient underwent bilateral surgery. Mean age of the patients was 36.46(range 4-85) years. Out of these, 87 were male and 14 were female. Forty five patients had right eye pathology, 54 patients had left eye pathology and 1 patient had bilateral involvement. Average follow-up was 15.42 months ( range 1.5-68). More than 67% of patients had follow up more than six months.
Presenting BCVA ranged from 6/36 to light perception (PL). Presenting mean IOP was 9.44 mm Hg (Range 0-40) (excluding those measured digitally). Mean IOP at six weeks and final visit was 8.55 mm Hg and 8.83 mm Hg respectively.
Intraoperative retinal attachment was seen in all cases. In 92 cases 1300 Cst silicone oil was used as tamponading agent and in rest 5000 Cst silicone oil was used.
Table 1 shows different indications for which 360 degree RR was done.
| Indications | Eyes | Percentage (%) |
| Recurrent RD | 37 | 36.63 |
| Primary Rheg RD | 23 | 22.77 |
| Post wound repair | 13 | 12.87 |
| RD with No breaks | 10 | 9.90 |
| Blunt trauma | 6 | 5.94 |
| Endophthalmitis | 5 | 4.95 |
| Diabetic CRD | 3 | 2.97 |
| Uveitic | 2 | 1.98 |
| FEVR | 1 | 0.99 |
| ARN | 1 | 0.99 |
Table-1: Different Indications
CRD: Combined retinal detachment, FEVR: Familial Exudative VitreoRetinopathy, ARN: Acute Retinal Necrosis
Chart 1 shows the pattern of vision change after surgery. Only 4.28% of patients had ambulatory vision pre-operatively which increased to 24.28% of patients after surgery which maintained till last follow-up. (Chart 2)
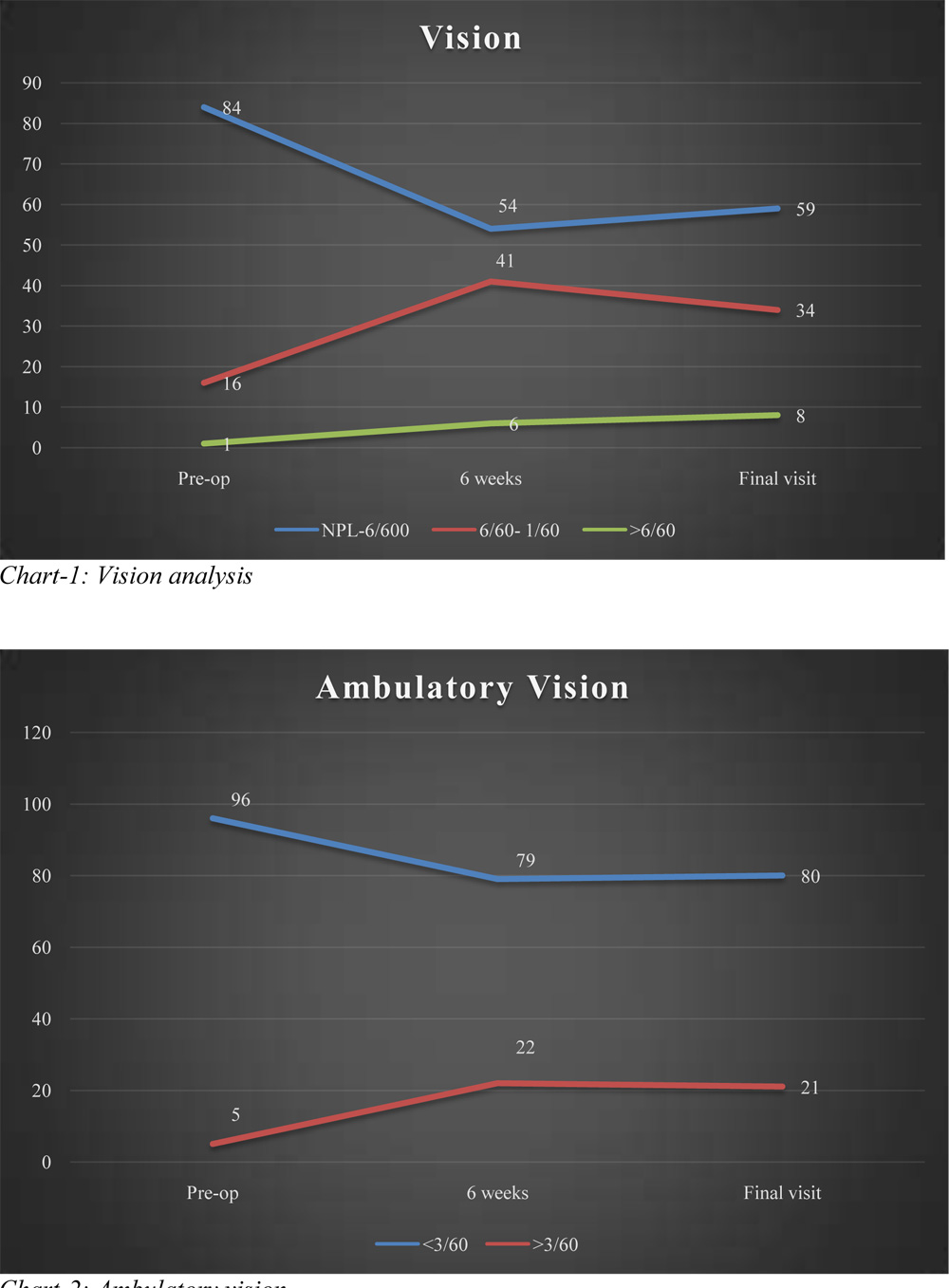 Chart-2: Ambulatory vision
Chart-2: Ambulatory vision
Table-2 shows anatomical outcome after the surgery, nearly 60% of patients showed attached retina. Repeat surgical intervention was done in nearly 32% case of total recurrence and partial recurrence. Remaining cases of recurrences were best left alone without further surgical intervention
| Anatomical Outcome | Eyes | Percentage (%) |
| Attached Retina | 60 | 59.41 |
| Partial Recurrence | 18 | 17.82 |
| Total Recurrence | 19 | 18.81 |
| No View | 4 | 3.96 |
Table-2 Anatomical outcome
Chart-3: Anatomical Outcome-flow chart
 Chart 2 showed the flow chart of the anatomical outcome. 50 eyes showed attached retina after primary surgery and 47 eyes showed detached retina. Out of these 47 eyes 22 eyes had partial recurrence and 25 had total recurrence, Repeat intervention was done in 7 eyes of partial recurrence and 8 eyes of total recurrence and out of these 15 eyes 10 eyes had reattached retina at final visit.
Chart 2 showed the flow chart of the anatomical outcome. 50 eyes showed attached retina after primary surgery and 47 eyes showed detached retina. Out of these 47 eyes 22 eyes had partial recurrence and 25 had total recurrence, Repeat intervention was done in 7 eyes of partial recurrence and 8 eyes of total recurrence and out of these 15 eyes 10 eyes had reattached retina at final visit.
Out of total 60 eyes showing retinal attachment at final follow-up, 44 eyes showed visual improvement compared to pre-op vision. Out of 22 eyes with partial re-detachment, 7 were re-operated. Out of rest 15, six eyes showed improved vision, 4 eyes showed deteriorated vision and 5 eyes showed no difference between pre-op and post-op vision. In 4 eyes after primary surgery fundus view was not possible. Out of these one eye showed total retinal detachment in ultrasound, this patient had no PL vision in that eye. Rest three eyes had attached retina on ultrasound, all these cases had pre-op and post op PL vision.
Silicone oil removal (SOR) was possible in 15eyes (14.85%). Mean SOR time after primary surgery was 10 months. Following SOR, 13eyes showed visual improvement, 1 eye showed one line less vision than pre-op and 1 eye showed no change in vision than pre-op. Post SOR mean IOP 9.53 mm Hg (range 1-16). Though Post SOR IOP decreased in few patients only two patients developed hypotony after SOR.
Table 3 showed different complications at final visit. Most common complications noted were hypotony and band shaped keratopathy.
In cases with keratopathy, 10 patients improved vision than pre-op, 3 patients had same vision as before and 4 patients had less vision than pre-op.
In case with hypotony, 21 patients had improved vision than pre-op, 7 patients had same vision as pre-op and 5 patient had less vision than pre-op.
| Complications | Eyes | Percentage (%) |
| Nil | 36 | 35.64 |
| Hypotony | 33 | 32.67 |
| BSK | 17 | 16.83 |
| High IOP | 7 | 6.93 |
| Disc pallor | 3 | 2.97 |
| Others | 5 | 4.95 |
Table-3: Post op complications at final visit.
Discussion:
The major cause of unsuccessful retinal detachment surgery is severe PVR. Retinectomies are required for complex retinal detachments with severe anterior PVR.(1) In our study most common indications for which relaxing retinectomy was required were recurrent retinal detachments followed by post-traumatic cases. In post traumatic cases, initial impact causes massive damage to retinal layers leading to severe PVR changes. Eyes with pre-existing severe PVR have more chances to go in post-operative severe PVR because of inflammation and retinal pigment epithelial cells exposure.(2) We performed 360 degrees relaxing retinectomy to relieve circumferential and anteroposterior traction in complex cases of retinal detachments after removing all pre-retinal membranes. After doing such complex procedure retinal leaflets become mobile under continuous fluid pressure, so to stabilize the posterior retina PFCL is a good option. (1) There are different ways of performing retinectomy. Shu Jiuan Sheu et al described dashed line retinectomy in which diathermy was applied in a dashed pattern under air or silicone oil and then retinectomy can be performed by tearing the dashed line with diathermy. Excision of the anterior retina can be done with microvit under air or silicone oil. In our study we used PFCL to flatten the posterior retina making a safer way to perform a good 360 degrees retinectomy after diathermy. Long acting gas or silicone oil are used as tamponading agents for complex retinal detachments (3). In our study we used silicone oil as tamponading agent in all cases. In comparison to long acting gas tamponade silicone oil tamponade gives better retinal attachments rate, and also by using silicone oil dependence on post-operative position decreases.(3) Tseng et al suggested that eyes in which silicone oil was used as tamponade agent showed good anatomical success initially but less functional outcomes. (4). Mancino et al also suggested that eyes with inferior retinal detachment with PVR showed better result with inferior 180 degrees retinectomy with silicone oil.(5)
In our study we found anatomical success rate of nearly 60%. Among all cases of re-detachment nearly 30% cases were re-operated for total and partial re-detachment each. Whether to re-operate the case is surgeon’s preference and mostly depend upon the functional outcome prediction after the re-surgery.
We had achieved intraoperative attachment in 100 % of cases. Most common etiologies which required 360 degrees of relaxing retinectomy were RD with severe PVR and RD secondary to trauma. There was significant difference in anatomical outcome between these two etiologies (P<0.002). There was statistical significant difference between pre-operative and final BCVA between these two groups
The functional outcome of the study was best judged by visual gain and maintenance of intra-ocular pressure. . In our study nearly 84% of patients had initial BCVA less than 6/600 and at last follow-up nearly 59% of patients had vision less than 6/600. Nearly 5% patients had ambulatory vision, which increased to 21% after surgery and it was maintaining till last follow-up.Post-op BCVA at final visit improved compared to pre-op BCVA, which was statistically significant. (p-value <0.01 paired T-test). Touka Banee et al demonstrated no significant association between pre-op good visual acuity and final visual outcome,(1) but from this analysis ,one can suggests that the cause of the low vision in most of the patients was eye condition at initial presentation. Eyes with initial less PVR with good visual acuity performs better post-operatively as compared to others. We observed that pre-op visual acuity is important predictor of postoperative final visual outcome and anatomical success. Though over period of time anatomical and visual outcome decreases, we had observed that there was no significant difference in anatomical attachment and visual acuity parameters at 6 weeks and at final follow-up.
Khaled AG Shalby et al in his study mentioned that extent of RR did not have influence on the final visual outcome(6)
Post-operatively most common complication seen was low IOP (Hypotony). In our study Hypotony was defined as IOP<5 mm Hg. Nearly 32.67% of patients developed hypotony at last follow-up. It has been proposed that hyptony is because of large bare choroid after retinectomy is available for the intra-ocular fluid absorption and also because of primary retinal pathology associated with ciliary body detachment. Though silicone oil filled eye tends to have high IOP Khaled AG Shalby et al showed there is no statistical significant association between hypotony and intra-ocular tamponade. It has been also demonstrated that post-operative phakic eyes have less chances of developing hypotony because lens act as barrier between Anterior PVR changes and ciliary body region.(6) There was significant difference in visual acuity between pre-op and final visit in all cases of hypotony in this study. We have reported 16.83% of patients with band shaped keratopathy after surgery. Banaee et al described that eyes with history of two or more vitrectomies, history of trauma, congenital/hereditary anterior segment abnormalities have greater tendencies of getting keratopathy.(1) There was no significant difference in occurrence of postoperative keratopathy in patients operated for different etiologies in this study and it was also not significantly associated with final anatomical outcome.
Because of chronic low IOP most of the surgeons tend to keep silicone oil for long period of time. Only 14.85% of patients underwent silicone oil removal up to last follow-up. Silicone oil removal depends upon surgeon’s decision and in our study, it was driven by maintenance of intra-ocular pressure, retinal status, and complications associated with silicone oil like glaucoma, cataract and keratopathy. Mostly silicone oil removal was deferred in hypotony and unstable retina. Eyes which underwent silicone oil removal has significant difference between pre-op and post op visual acuity (P value<0.01).
We highlight this study as a largest case series in the literature on 360 degree retinectomies having a maximum follow up of 68 months. Limitations here are of retrospective analysis, and non-comparative study. Though the follow upis reasonably good period, more longer follow-up may give further long term anatomical and functional changes in these diseased eyes.
Conclusion:
Though 360 degree RR is difficult surgical manoeuvre, with help of evolving small gauge instrumentation, new surgical techniques it can be performed routinely in settling complex retinal detachments with good anatomical success.
Though anatomical success is not correlated with functional visual gain, some patients do gain ambulatory vision.
References:
- Banaee T, Hosseini SM, Eslampoor A, Abrishami M, Moosavi M. Peripheral 360 retinectomy in complex retinal detachment. Retina. 2009;29(6):811-8.
- Mendes TS, Gomes AMV, Rocha BS, Junior HVP, Abujamra S. Evaluation of retinectomy in the treatment of severe proliferative vitreoretinopathy. International Journal of Retina and Vitreous. 2015;1(1):1.
- Tsen C-l, Horng Y-H, Sheu S-J. Dashed line relaxing retinotomy in the management of retinal detachment with anterior proliferative vitreoretinopathy. Clinical ophthalmology (Auckland, NZ). 2015;9:585.
- Tseng JJ, Barile GR, Schiff WM, Akar Y, Vidne-Hay O, Chang S. Influence of relaxing retinotomy on surgical outcomes in proliferative vitreoretinopathy. American journal of ophthalmology. 2005;140(4):628. e1-. e10.
- Mancino R, Aiello F, Ciuffoletti E, Di Carlo E, Cerulli A, Nucci C. Inferior retinotomy and silicone oil tamponade for recurrent inferior retinal detachment and grade C PVR in eyes previously treated with pars plana vitrectomy or scleral buckle. BMC ophthalmology. 2015;15(1):1.
- Shalaby KA. Relaxing retinotomies and retinectomies in the management of retinal detachment with severe proliferative vitreoretinopathy (PVR). Clin Ophthalmol. 2010;4:1107-14.