Dr. Garvit Bhutani, Dr. Mohit Dogra, Dr. Gupta Amod Kumar
INTRODUCTION
Incidence of rhegmatogenous retinal detachment has been reported as 6.3-17.9 per 100,000 populations while in Indian population it has been reported around 3.9 per 100,000 Indians. The management options for rhegmatogenous retinal detachment varies from as simple as pneumatic retinopexy to scleral buckling to primary vitrectomy with internal tamponade. There are various options available for the internal tamponade like silicone oil, sulfur hexafluoride gas (SF6), hexafluoroethane (C3F8) etc. Silicone oil study has demonstrated that anatomic outcome is better with oil than SF6 gas whereas the functional outcome (VA ≥ 5/200) was found comparable between the oil and the C3F8 gas group.
Both the types of tamponade are associated with certain disadvantages like maintenance of a specific posture after gas tamponade, contraindication for air travel and delayed recovery of ambulatory vision in cases with gas tamponade whereas associated disadvantages with oil tamponade are need of second surgery to remove the oil, corneal decompensation and raised IOP etc.
MATERIALS AND METHODS
A prospective non randomized study was conducted at the retina clinic of Advanced Eye Centre where 40 eyes of 40 patients with primary rhegmatogenous non complex retinal detachment were enrolled. Minimum follow up period for the study was 3 months. All patients underwent primary pars plana vitrectomy followed by internal tamponade with either silicone oil (1000 CS) or Gas (C3F8/SF6). Inclusion criteria for the study were primary rhegmatogenous retinal detachment with macula off and less than one month duration of retinal detachment with PVR changes < Grade C2. Exclusion criteria Giant Retinal Tears, Traumatic Retinal Detachments, previous macular lesions, history of amblyopia, exudative or tractional retinal detachment, Media opacities precluding OCT imaging and Re-RD within 3 months follow up. The study sample was divided into 2 groups based on the type of internal tamponade given, viz. OIL group and GAS group. Patients in GAS group either received C3F8 gas or SF6 gas while all patients in OIL group received 1000 CS silicone oil. Silicone Oil tamponade was preferred in one eyed patients, patients anticipated to have problem with maintenance of posture in post operative period, patients living at high altitudes and in patients planning to travel by air in near future. The primary outcome measure of the study was to assess the foveal structure on Spectral Domain Optical Coherence Tomography (SD-OCT) in both the groups at the end of 3 months. Secondary outcome measure was change in Visual acuity at the end of 3 months in the 2 groups. The best-corrected visual acuity was determined from Snellen chart and converted to the logarithm of minimal angle of resolution (logMAR) equivalents to perform the appropriate statistical manipulation. Other parameters like age, sex, duration of retinal detachment and pre-operative lens status were also noted.
SURGICAL PROCEDURE
Pars plana vitrectomy with silicone oil or SF6/C3F8 tamponade was performed under sterile conditions in the operating room. The patients accepted standard three-port pars plana vitrectomy using a Constellation vitrectomy machine (Alcon, Fort Worth, TX, USA). Initially, the vitreous was removed. A puncture retinotomy was performed using endodiathermy, and subretinal fluid was aspirated using a long extensible silicone-tipped cannula through the retinotomy. After fluid air exchange, once the retina was totally attached, laser photocoagulation/cryopexy was done, surrounding all retinal breaks and along the entire edge of the puncture retinotomy site. Finally, the silicone oil or SF6/C3F8 gas was injected into the eye for tamponade. In cases with silicone oil tamponade, silicone oil was removed as and when required after ensuring achievement of a stable retinal situation. If cataract developed in the eyes after retinal surgery that obviously affected the vision, then cataract extraction would be performed in these cases.
STATISTICAL ANALYSIS
Visual acuity was converted into logMAR for statistical analysis. Statistical analysis was done using SPSS version 20.0 (SPSS Inc., Chicago, IL, USA). Pearson’s chi square test was used to find significance level of OCT findings. Univariate analysis was applied to compare change in visual acuity between the 2 groups and the means were compared using paired and unpaired T test. A p value < 0.05 indicated statistical significance.
| Gas | Oil | |
| Phakia | 5 (20.8%) | 2 (12.5%) |
| Pseudophakia | 18 (75%) | 8 (50%) |
| Aphakia | 1 (4.2%) | 6 (37.5%) |
RESULTS
40 eyes of 40 patients with primary rhegmatogenous retinal detachment were enrolled, of which right eye was affected in 19 patients and left eye was affected in 21 patients. The mean age of the cohort was 54.69±13.77 years. The study sample comprised 14 females (35%) and 26 males (65%) and all had undergone a successful anatomical repair of
rhegmatogenous retinal detachment. Number of patients in the OIL group was 16 and in the GAS group was 24. The mean duration of RD was 20.63±8.20 days in Gas Group and 22.81±8.83 days in Oil Group. The pre-operative lens status of the two groups has been depicted in the table above. Both the groups were comparable in all the baseline characteristics.
On SD-OCT the findings were labeled as normal/ atrophy/LMH/ERM. Normal foveal contour was achieved in 21 out of 24 eyes (87.5%) in the GAS group while in OIL group it was achieved in only 6 eyes out of 16 (37.5%). Foveal atrophy was defined as Central Macular Thickness (CMT) <250µm and it was seen in 8 out of 16 eyes (50%) in the OIL group while it was much lower in the GAS group, 2 out of 24 eyes (8.3%). The p value for the difference in number of eyes with foveal atrophy of the 2 groups was <0.05.
| Gas | Oil | |
| Pre-Operative BCVA
(logMAR units) |
2.40±0.81 | 2.68±0.91 |
| Post-Operative BCVA
(logMAR units) |
0.77±0.46 | 1.32±0.72 |
Although the mean pre operative BCVA was comparable between the 2 groups, mean post operative BCVA in the GAS group was significantly better than the OIL group (p value < 0.05).
Mean change in visual acuity in the GAS group was 1.63±0.78 logMAR units and in the oil group it was 1.35±0.83 logMAR units.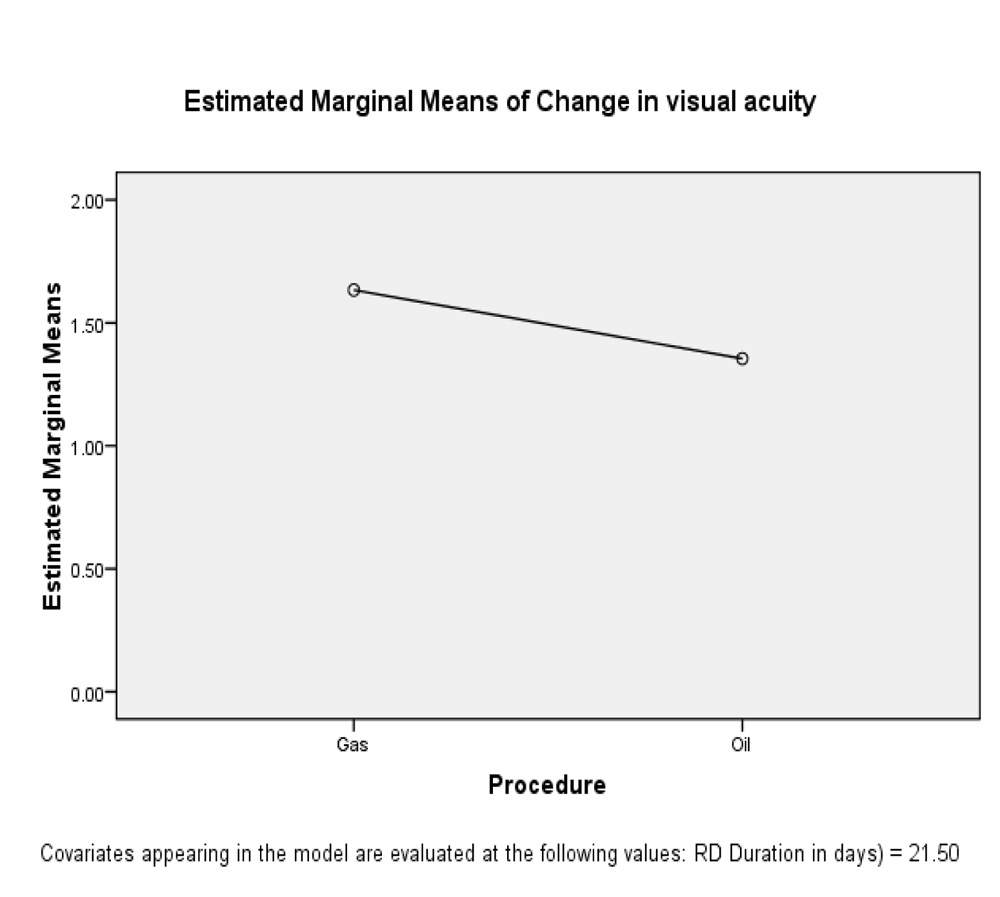
DISCUSSION
The Baseline characteristic like mean age and mean duration of RD were comparable between the two groups. But in pre-operative lens status oil was preferred more in aphakic patients (37.5%) whereas gas was preferred more in pseudophakics (75%). On SD-OCT, it was found that incidence of foveal atrophy was significantly more common in silicone oil group (50%) as compared to gas group (8.3%). [P value=0.001]. There was significant change in BCVA, 3 months post operatively when compared to pre-operative BCVA in both the groups. Although the GAS group had a significantly better mean BCVA at the end of 3 months, there was no significant difference between the two groups when compared for change in BCVA [P value=0.296]. The major limitations of our study were small sample size and a short follow up.
CONCLUSION
In primary non complex rhegmatogenous RD, Gas tamponade restores the foveal anatomy in more number of patients than silicone oil. However functional outcome may not mirror the anatomical outcome, as seen in our study with comparable improvement of visual acuity in both the oil as well as gas group. Based on our findings we would like to hypothesize that silicone oil is responsible for greater damage to the photoreceptors, thus, the foveal atrophy as compared to gas, when used as a tamponade agent. Thus we would like to suggest silicone oil should be reserved for repair of complex retinal detachments.