Dr. Sharad Bhomaj, B07421
AUTHOR : Dr Sharad Bhomaj
INTRODUCTION
We owe our patients a scientific answer about the outcome of the surgery we propose to do . Anatomical closure may not always result in visual success in macular hole surgery. Vision loss can also occur. International literature reports show hole closure rates vary from 80-92%, visual success in 40-83% & visual loss in 8-26% cases.
- Idiopathic macular holes (MH) are defects of retinal tissue involving the anatomic fovea , causing central visual loss and /or metamorphopsia .
- A meta‐analysis on 1654 eyes treated using different techniques reported that 87.5% of eyes achieved anatomic success, with 12.5% failing to close.5
- As the number of macular hole surgeries has been on the rise , analysis of predictive factors determining the anatomical and functional success of the surgery has assumed great importance to aid both the surgeon and the patient to take evidence based ,informed decisions prior to the surgery
Based on a detailed , multiple logistic regression analysis of various OCT parameters in 44 cases of macular hole surgery,we found that using multiple OCT indices and parameters in unision is the only way to reliably predict outcomes .Using MLD( Minimum linear diameter),ELM integrity , grading the cystic edema of hole edges , MHI ( Macular hole index) ,HFF ( Hole form factor) & THI (Tractional hole index) ,we present a nomogram to reliably predict both anatomical and visual outcomes .To avoid time spent on manual calculations of OCT indices , this online nomogram does all calculations and gives a numerical score for hole closure & visual success .
MATERIALS AND METHODS
- STUDY DESIGN : Retrospective ,consecutive ,interventional case series between April 2011- April 2015
- SETTING : Private vitreo retinal practice , single surgeon
- INTERVENTION : 23 G PPV for macular hole surgery
- MAIN OUTCOME MEASURE : Predictive value of pre-op OCT parameters with respect to anatomic closure and visual outcome after macular hole surgery
- INCLUSION CRITERIA :Cases undergoing 23G PPV for idiopathic macular holes Minimum follow up of 3 months after surgery
- EXCLUSION CRITERIA :Co-existing macular or optic nerve pathology which could affect the visual outcomes of surgery
- All eyes underwent a comprehensive clinical evaluation including
- Presenting best corrected visual acuity
- Laterality
- Anterior segment bio-microscopic examination to look for lens changes
- Direct and indirect fundus examination.
- Pre operative OCT
- At the baseline examination, OCT scan was registered and saved as a reference image
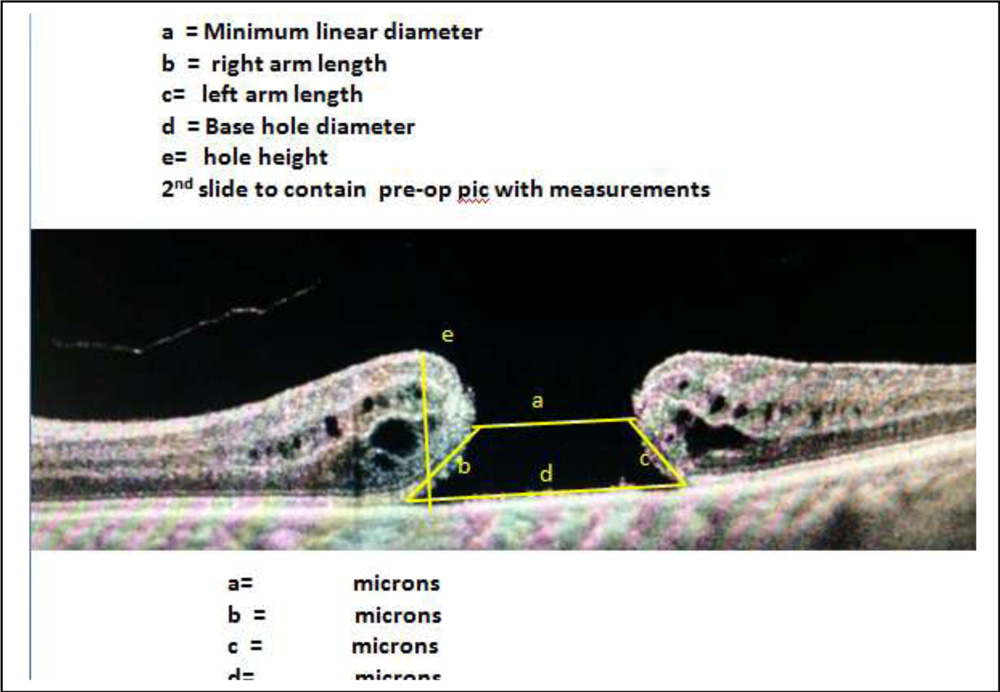
Macular hole indices were calculated from images
- Macular hole minimum linear diameter (MLD) – Minimal horizontal extent of the hole (Measurement b- Fig 1)
- Macular hole Base Diameter(BD) – distance measured at the level of retinal pigment epithelium (Measurement a-Fig 1)
- Tractional Hole Index(THI) – e / b (e= Vertical distance between the RPE and the highest portion of macular hole(Height -MHH , b= MLD)
- Macular Hole Index(MHI) – e / a (e= MHH, a= BD)
- Surgery consisted of standard three port pars plana vitrectomy, peeling of the epiretinal membranes if present and the inner limiting membrane with subsequent instillation of a gas tamponade (C3F8 ).
- After surgery patients were asked to maintain a prone position for at least 1 week .
- Postoperatively patients were viewed at the end of one week and assessed for postoperative Visual acuity and underwent repeat OCT .
- Anatomical success was defined as closure of the hole with restoration of anatomical continuity
RESULTS :
a = Minimum linear diameter
b = right arm length
c= left arm length
d = Base hole diameter
e= hole height
| OCT INDEX | VALUE | n= number | VA IMPROVED | P value | HOLE CLOSED | P value |
| MLD | <400 | 19 | 10 (52.63%) | 0.625 | 18 (94.73%) | 0.004* |
| >400 | 25 | 15 (60%) | 0.438 | 21 (84 %) | 0.03 | |
| BD | <800 | 10 | 5 (50%) | 0.598 | 9 (90 %) | 0.02 |
| >800 | 34 | 20 (58.82%) | 0.422 | 30 (88.23%) | 0.0031* | |
| THI
>1.4 better |
<1.41 | 35 | 21 (60 %) | 0.396 | 31 (88.57%) | 0.0012* |
| >1.41 | 9 | 4 (44.44%) | 0.723 | 8 (88.88%) | 0.004* | |
| MHI
>0.5 better |
<0.5 | 30 | 17 (56.66%) | 0.062 | 28 (93.33%) | 0.002* |
| >0.5 | 14 | 8 (57.14%) | 0.615 | 11 (78.57%) | 0.004* | |
| HFF
> 0.5 better |
<0.5 | 4 | 3 (75%)* | 0.023 | 3(75%) | 0.005* |
| >0.5 | 40 | 22(55%)* | 0.042 | 36(90%) | 0.003* | |
| ELM formed | 32 | 22(68.75%) | 0.728 | 30(93.75%) | 0.004* | |
| Cystic edema of hole edges | 34 | 20(58.82%) | 0.637 | 31(91.18%) | 0.001* | |
| Atrophic hole edges | 10 | 5 (50%) | 0.701 | 8 (80%) | 0.004* |
| Prognostic parameter | |||||
| Hole closure rate prediction | MLD < 400 94.73%
ELM formed 93.75% Cystic edema 91.18% BD < 800 90% MHI<0.5 90% |
||||
| Hole non -closure predictor | Co-exising retinal pathology
BRVO Absence of cystic edema |
||||
| Visual improvement prediction | ELM formed 68.75%
THI <1.4 60% Cystic edema 58.82% MHI >0.5 57.14% |
||||
| Poor visual outcome predictor | Atrophic hole edges –Absence of cystic edema
Co-existing retinal pathology – BRVO ,Dry AMD , Diabetic retinopathy |
||||
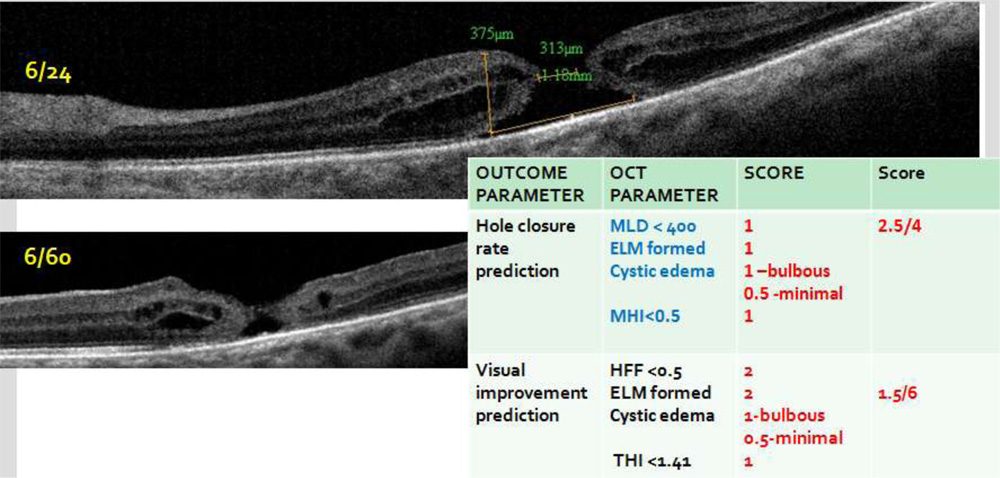
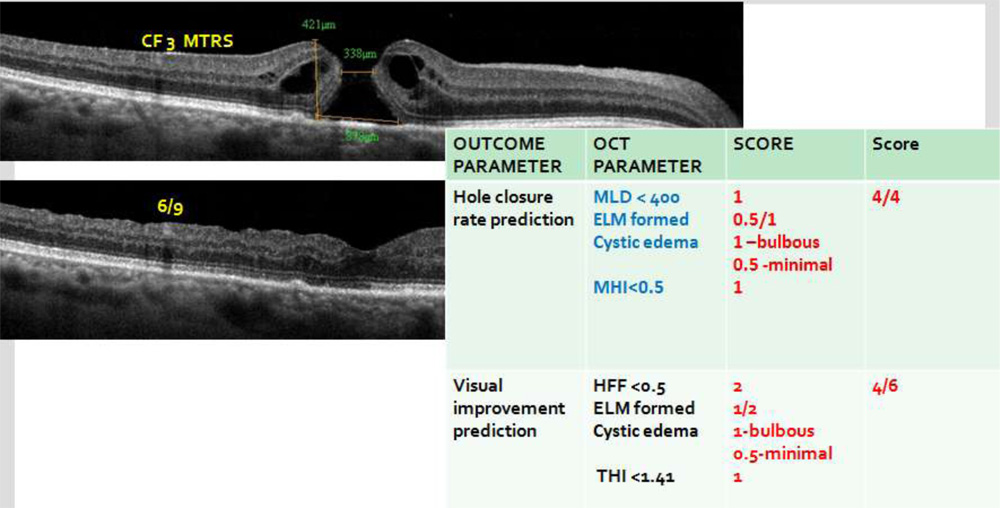
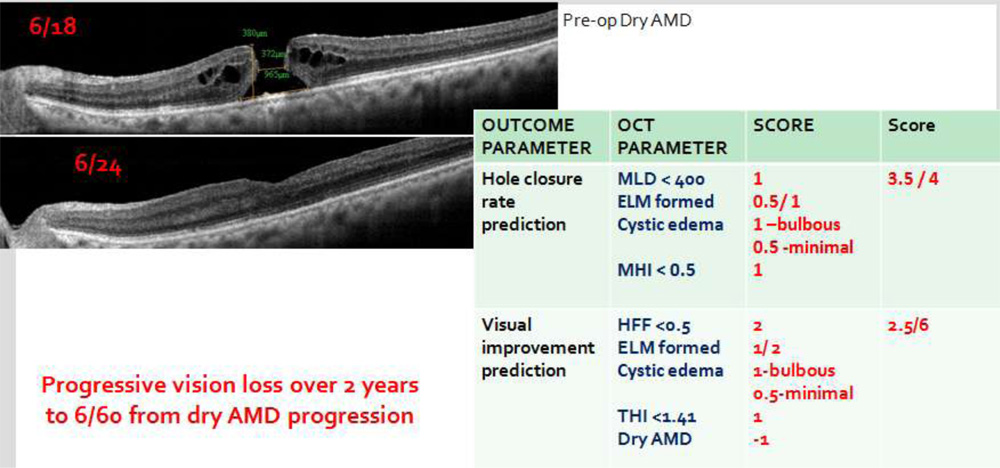
| OUTCOME PARAMETER | OCT PARAMETER | SCORE | Max score | ||
| Hole closure rate prediction
|
MLD < 400 ELM integrity
Cystic edema
MHI <0.5 |
1
1 1 –bulbous 0.5 -minimal 1 |
4 | ||
| Visual improvement prediction | HFF <0.5 ELM integrity
Cystic edema THI< 1.4 |
2
2 1- bulbous 0.5– minimal 1 |
6 | ||
| Visual loss predictor | Co-existing macular pathology | 0 Healthy macula
– 0.5 Mild disease – 1 Moderate disease – 2 Severe disease |
|||
 References :
References :
1. Wang S, Xu L, Jonas JB: Prevalence of full thickness macular holes in urban and rural adult Chinese: the Beijing Eye Study. Am J Ophthalmol 2006; 141: 589–591.
2.Jackson TL, Donachie PH, Sparrow JM, Johnston RL: United Kingdom National Ophthalmology Database study of vitreoretinal surgery: report 2, macular hole. Ophthalmology 2013 Mar;120(3):629-34.
3.McCannel CA, Ensminger JL, Diehl NN, Hodge DN: Population-based incidence of macular holes. Ophthalmology 2009; 116:1366–1369.
4.Kelly NE, Wendel RT. Vitreous surgery for idiopathic macular holes: of a pilot study. Arch Ophthalmol 1991;109:654–9.
5.Mester V, Kuhn F. Internal limiting membrane removal in the management of full‐thickness macular holes.Am J Ophthalmol 2000129769–777.777
6.Huang, D., Swanson. E.A., Lin. C.P., et al. 1991. Optical coherence tomography. Science 254:1178–81.
7.V., Williamson. T.H., 2000. Watzke‐Allen slit beam test in macular holes confirmed by optical coherence tomography. Arch Ophthalmol. Aug:118(8):1059‐63.
8.K.V., Murthy. R.K., Gupta. S.K., Brar. V.S., Grover. S., 2010. Foveal structure defined by spectral domain optical coherence tomography correlates with visual function after macular hole surgery. Eur J 249 Ophthalmol. May‐Jun:20(3):572‐7
9.Predicting Visual Outcome following Surgery for Idiopathic Macular Holes Sentaro Kusuhara Akira Negi Ophthalmologica 2014;231:125–132