Dr. Pranav Ranjan, R06641, Dr. Devesh Kumawat, Dr. Pranita Sahay
Free Paper Topic-
Evidence based approach to Posterior Polar Cataract Surgery
Introduction
Posterior polar cataract has an autosomal dominant inheritance pattern. However, it has also been noted as a result of gene mutation.
It consists of dysplastic lens fibers, which, in their migration posteriorly from the lens equator, exhibit progressive lens opacity with the formation of a characteristic discoid posterior polar plaque like cataract which sometimes is adherent to the posterior capsule.
The occurrence of posterior polar cataracts is rare; in fact, little is published on the specific incidence of posterior polar cataracts. Further, no standardized subtype specific study on this type of cataract has been conducted. In the Framingham Eye Study, little prevalence data for posterior polar cataracts are presented. However, it is well accepted that this is an infrequently encountered form of cataract and that the prevalence is very low. When seen, it is often as an inherited trait and is present in several members of the same family.
One population-based analysis of posterior polar cataract prevalence has been studied. In summary, 111 cases of posterior polar cataracts were found against 37,837 population controls without ocular defects. Even among congenital cataracts, posterior polar cataracts are rare.
Other population studies have not focused on the incidence of posterior polar cataracts. Most studies based data on the incidence of all types of cataracts, which were part of the focus of the Framingham Eye Study, but found mainly age-related cataracts, although posterior subcapsular opacities were reported to occur in the younger subjects of the group studies. The Framingham Eye Study did not specifically address the incidence of posterior polar cataracts as a separate group. Other studies focused on incidence and etiology and nutrition.
Posterior polar cataract presents as a distinctive discoid lens opacity situated posteriorly, adjacent to the posterior capsule. Duke-Elder mentions stationary as well as progressive cataracts.
It is easily seen and often clearly delineated. In its early stages, it can be seen interfering with the normal light reflex. Fully formed, it presents as a dense, circular plaque in the central posterior part of the lens. It can be surrounded by vacuoles and smaller areas of degenerated lens material.
Posterior polar cataract presents a challenging situation for the anterior segment surgeon. The condition, a dominantly inherited disorder with variable expressivity, may be associated with intraoperative defects in the posterior capsule. Because the condition is dominantly inherited, typically both eyes are involved and there is no gender preference. Previous publications indicate as high as a 26% likelihood for a defective capsule at the time of cataract surgery.It is unclear whether the defect in the capsule is pre-existent or develops iatrogenically because of marked thinning.
Can one assess if the capsule is defective prior to surgery?
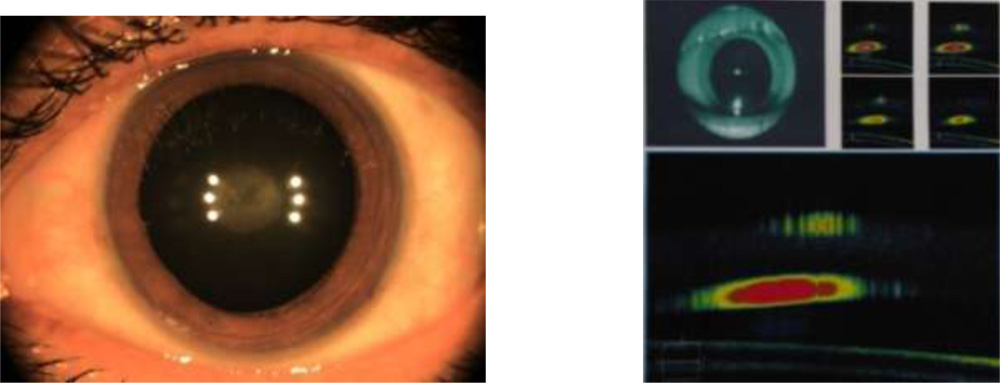
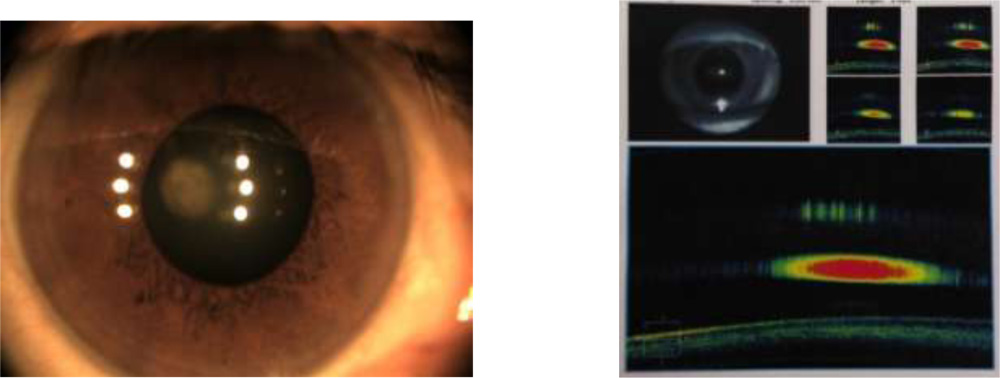
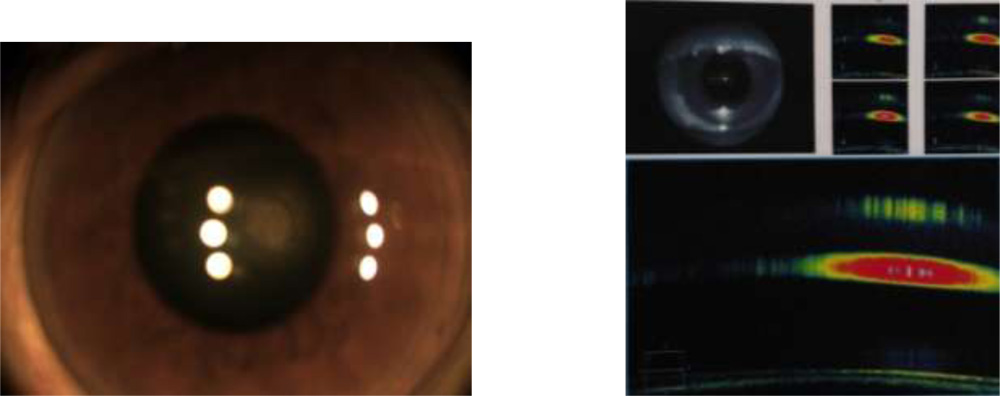
Daljit Singh, an extraordinarily prolific Indian surgeon, has described a sign that he suggests is indicative of a defect in the capsule. His sign is that of a series of satellite minicataracts surrounding the main posterior polar plaque. In his view, the congenitally defective capsule allows aqueous to permeate into the lens material and induce small secondary opacities. In my surgical experience, a defective capsule in one eye is most often met with a defective capsule in the second eye. Likewise, the earlier in life the patient presents with symptoms, the greater the likelihood for a defective capsule. Conversely, elderly patients with posterior polar cataract in addition to nuclear or other age-related cataract formation tend not to have defective capsules.
In any case, because of the proclivity for a defective posterior capsule in a significant proportion of cases, a surgical strategy must be adapted in order to preclude serious intraoperative complications should capsule rupture occur. Moreover, the strategy will prepare the surgeon for dealing with capsule rupture under other circumstances.and counseling such a patient in preparation for surgery,
Relevant Anatomy
A posterior polar cataract consists of dysplastic lens fibers, which, in their migration posteriorly from the lens equator, exhibit progressive lens opacity with the formation of a characteristic discoid posterior polar plaque like cataract.
Histology has shown that posterior polar cataracts consist of lens fibers that have developed abnormally. Further, the lens fibrils have degenerated and, in some cases, are directly attached to the posterior capsule. Often, the posterior polar opacified plaque is surrounded by a less distinct area of fibrillar degeneration as well as vacuoles filled with liquefied material.
Purpose –
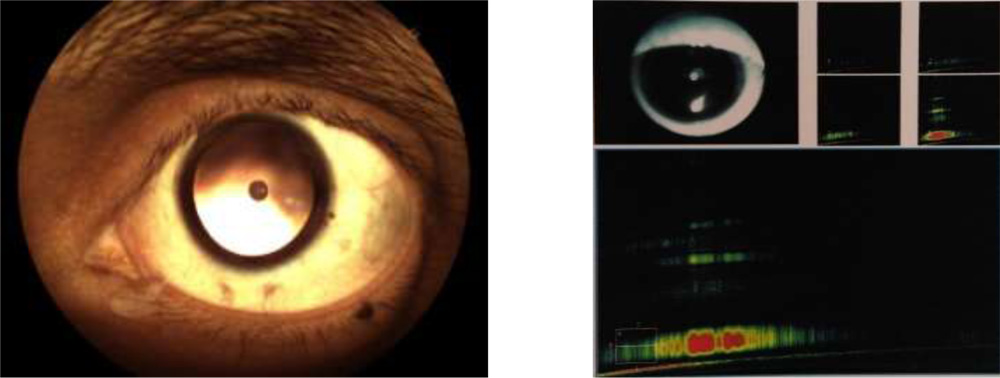
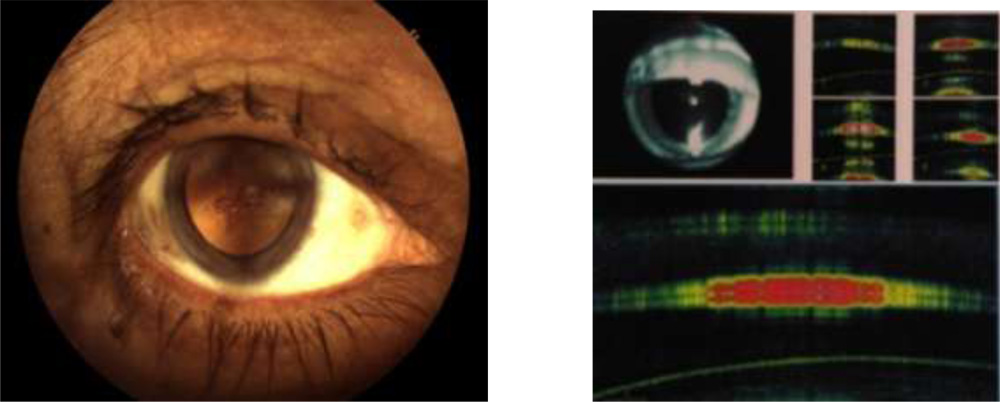
The purpose has been to come up with a evidence based tool to assess posterior capsule integrity and its relationship to plaque.The evidence can caution the surgeon of the intra operative course , so that one is prepared to handle such situations. The patients can also be counselled the same way prior to surgery. This can be done by imaging the PC–Plaque complex by HD AS OCT.
Method
In a prospective study cases see in the eye OPD and also known older cases were called up and included in the study.After having been diagnosed on slit lamp examination after full mydriasis as Posterior polar cataract they were subjected to furher evaluation. Routine systemic and eye examination were carried out to rule out other coexisting anomalies. In this study 31 cases (eyes) from 23 patients of posterior polar cataract the following methodology was adopted
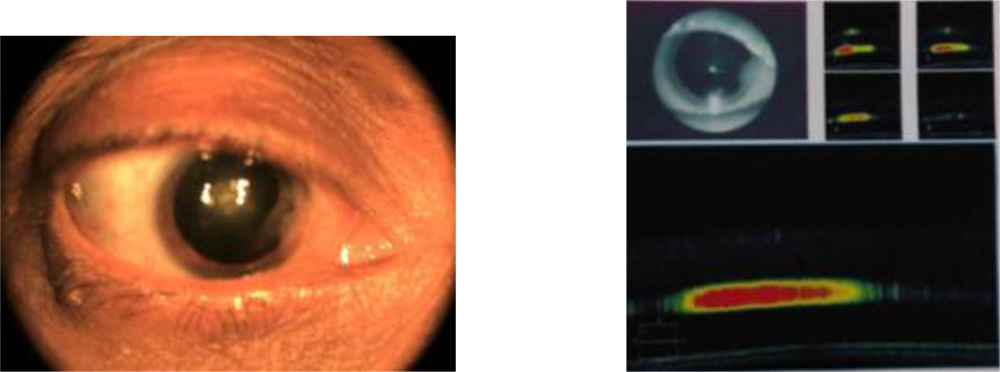
Anterior segment spectral domain anterior segmment Cirrus Zeiss OCT pictures were obtained.
Anterior segmment photograph using Trinetra capturing device was done.
Slit lamp photography was taken by mobile phone attachmment.
Surgical video of concerned cases were recorded. The intraoperative surgical precautions of smaller rhexis, multiplace hydro procedure with more hydrodelineation and careful little rotation of nucleus, lower bottle height and low parameters with slow motion phaco was carried out .
( Video clip will be attached in presentation)
Inclusion criteria- all sex and age group patients.Some known cases of PPC were called up and included in the study.
Exclusion criteria-any metabolic systemic disease, corneal pathology, advanced nuclear sclerosis.
Result
29 out of 31 cases have shown clear space between the discoid plaque and posterior capsule.
Intraoperative behaviour in 29 cases undergoing standard phacoemulsification with predetermined slow motion phaco parameters was as predicted and uneventful and none of them had posteror capsular rupture ( PCR ).
Two cases had doubtful adherance but the surgery was uneventful in one while the other had PCR which was subsequently managed with anterior vitrectomy.
Discussion
It is a easy testing strategy which can prepare the surgeon for any untoward evantuality. Result of my ongiong study is very encouraging as 100% cases undergiong surgery behaved as per the OCT finding. In this small study there was no posterior capsule defect in 29 eyes while 2 eyes had doubtful adherance of plaque to the posterior capsule of which one eye encountered PCR.
Shroff et all in 2013 at ESCRS has reported PCR in 12 / 56 eyes (21.4%)
H Siatiri and S Moghimi in 2005 have reported no PCR in 34 eyes.
However older reports as in Journal of cataract and refractive surgery, March 1990 by Robbert H et all had eight PCR in 31 cases (26%).with planned extracapsular or phacoemulsification.
Somshekhar Nagappa et all ( 2015 ASCRS) have reported the use of in-vivo mounted AS OCT for assessment of existing posterior capsular defec tin patients with PPC.in three cases with 100% predictibility.
Strength of study
Remarkable predictibility as seen in this study can give the surgeon precise evidence based information of posterior capsule status in dealing with such cases.
Limitation of study
Small sample size and still waiting to assess large sample corelation between a imaging defect in posterior capsule and the eventual surgical outcome.
References
1.Lee M.W., Lee Y.C. Phacoemulsification of posterior polar cataracts—a surgical challenge. Br J Ophthalmol. 2003;87:1426–1427. [PMC free article] [PubMed]
2.Masket S. Consultation section: Cataract surgical problem. J Cataract Refract Surg. 1997;23:819–824. [PubMed]
3.Vogt G., Horvath-Puho E., Czeizel E. A population-based case-control study of isolated congenital cataract. Orv Hetil. 2006;147(23):1077–1084. [PubMed]
4.Osher R.H., Yu B.C., Koch D.D. Posterior polar cataracts: a predisposition to intraoperative posterior capsular rupture. J Cataract Refract Surg. 1990;16:157–162. [PubMed]
5.Vasavada A.R., Singh R. Phacoemulsification with posterior polar cataract. J Cataract Refract Surg. 1999;25:238–245. [PubMed]
6.Gifford S.R. Congenital anomalies of the lens as seen with the slit lamp. Am J Ophthalmol. 1924;7:678–685.
7.Cordes FC. Types of congenital and juvenile cataracts. In GM, editor. Symposium on Diseases and Surgery of the lens. St. Louis, CV Mosby; 1957. p. 43–50
8.Eshaghian J., Streeten B.W. Human posterior subcapsular cataract; an ultrastructural study of the posterioly migrating cells. Arch Ophthalmol. 1980;98:134–143. [PubMed]
9.Nagata M., Matsuura H., Fujinaga Y. Ultrastucture of posterior subcapsular cataract in the human lens. Ophthalmic Res. 1986;18:180–184. [PubMed]
10.Eshajian J. Human posterior subcapsular cataracts. Trans Ophthalmol Soc UK. 1982;102:364–368. [PubMed]
11.Eshagian J. Human posterior subcapsular cataracts. Trans Ophthalmol Soc UK. 1982;102(Pt 3):364–368. [PubMed]
12.Tulloh C.G. Hereditary posterior polar cataract with report of a pedigree. Br J Ophthalmol. 1955;39(6):374–379. [PMC free article] [PubMed
13.Luntz MH. Clinical types of cataracts. Duane’s Ophthalmology. CD ROM. ed. Baltimore, M d.: Lippincott Williams & Wilkins; 2006.
14.Duke-Elder S. Congenital deformities. Part 2. Normal and Abnormal Development. System of Ophthalmology; vol. III. St. Louis: CV Mosby; 1964.
15.Singh D., Worst J., Singh R., Singh I.R. Jaypee Brothers Medical Publishers; New Delhi, India: 1993. Cataract and IOL. p. 163–5.
16.Hayashi K., Hayashi H., Nakao F. Outcomes of surgery for posterior polar cataract. J Cataract Refract Surg. 2003;29:45–49. [PubMed]
17.Das S., Khanna R., Mohiuddin S.M., Ramamurthy B. Surgical and visual outcomes for posterior polar cataract. Br J Ophthalmol. 2008;92(11):1476–1478. [PubMed]
18.Haripriya A., Aravind S., Vadi K., Natchiar G. Bimanual microphaco for posterior polar cataracts. J Cataract Refract Surg. 2006;32(6):914–917. [PubMed]
19.Pong J., Lai J. Managing the hard posterior polar cataract. J Cat Refract Surg. 2008;34:530–531. [PubMed]
20.Fine I.H., Packer M., Hoffman R.S. Management of posterior polar cataract. J Cataract Refract Surg. 2003;29:16–19. [PubMed]
21.Vasavada A.R., Raj S.M. Inside-out delineation. J Cataract Refract Surg. 2004;30:1167–1169. [PubMed]
22.Vajpayee R.B., Sinha R., Singhvi A., Sharma N., Titiyal J.S., Tandon R. ‘Layer by layer’ phacoemulsification in posterior polar cataract with pre-existing posterior capsular rent. Eye (Lond) 2008;22(8):1008–1010. [PubMed]
23.Allen D., Wood C. Minimizing risk to the capsule during surgery for posterior polar cataract. J Cataract Refract Surg. 2002;28:742–744. [PubMed]