Dr. Hardik
Shroff, S10859, Dr. Shroff Ashok Pranjivandas, Dr.
Dishita Shroff
Chief Author : Dr. Hardik A. Shroff
Co-Authors : Dr. Ashok P. Shroff
Dr. Dishita H. Shroff
Introduction
Silicone oil has been extensively used to treat complex retinal detachment or severe proliferative diabetic retinopathy. Many times silicone oil is not removed and is kept for long time to prevent recurrence of retinal detachment. Sooner or later it leads to cataract formation which needs removal of cataract with IOL implantation. Now doing biometry, many times, AP length measurement is not possible due to illdefined pattern. However, with IOL master and similar latest equipments, biometry is possible and can calculate IOL power but presuming that silicone oil would be removed during cataract surgery. Moreover, at times, it is not wise to remove silicone oil to maintain the integrity of retina. In such situation, we have observed that implantation of such calculated IOL gives lots of refractive surprises. When these latest equipments were not available, we used to do intraoperative refraction after cataract removal to decide the power of IOL and were very satisfied. Therefore, we wanted to compare the IOL power calculated by IOL master and intraoperative retinoscopy to decide which was better.
Material
18 cases were selected for this study. 11 cases were male while 7 were female. Their age varied from 34 years to 73 years, mean being 64.5 years. Eyes were equally distributed between right and left. 10 eyes were operated for complex retinal detachment with silicone oil, while 8 eyes were operated for vitrectomy with silicone oil in cases of severe proliferative diabetic retinopathy. Surgeries were performed 6 months to 2.5 years prior to development of cataract) (Table – 1).
Table – 1 Demography
| Total Eyes | Sex | Eye | Age | |||
| 18 | Male | Female | RE | LE | ||
| 11 | 7 | 9 | 9 | 34 to 73 years (mean 64.5 years) | ||
| Past History of | ||||||
| RD Repair with Silicone oil | 10 eyes | |||||
| Vitrectomy for PDRP with silicone oil | 8 eyes | |||||
| Time lapsed | 6 months to 2.5 years (mean 1.1 year) | |||||
Procedure
Complete preoperative work up was done routinely. Biometry was done by IOL master. AP length was modified by 0.71 factor for calculation purpose and IOL power was calculated. Routine phaco procedure was done taking care to avoid any intraoperative complication particularly PCR. Then AC was fully formed by visco keeping the pupil well dilated. Intraoperative refraction was done by skilled refractionist using autoclaved refraction set and maintaining proper asepsis. IOL power was selected by addition of 11D (surgeon’s factor) in the refraction value. Then foldable IOL of that diopter was inserted and placed `In the Bag’. Routine postoperative treatment was advised. There was no postoperative complication. Then refraction was done after one month by the same refractionist. IOL power calculated by IOL master, intraoperative refraction and residual refraction were compiled and compared.
Results
There was no major postoperative complication in any case. By the end of one month, all eyes were quite with clear cornea, good AC depth, normal IOP range and no adverse effect on retinal status.
Table – 2 Difference between IOL power calculated by IOL Master and
Intraoperative Retinoscopy
| Difference in Diopter | No. of Eyes |
| 0 to 5 D (Range from 2.50 to 5.00D, mean 4.12D) | 04 (22.22%) |
| >5 to 10 D (Range from 5.50 to 8.00D, mean 7.00D) | 08 (44.44%) |
| > 10 to 15 D (Range from 11.00 to 12.50D, mean 11.75D) | 02 (11.11%) |
| > 15 D (Range from 15.00 to 18.00 D mean 16.25D) | 04 (22.22%) |
Here IOL power calculated by IOL master was significantly less than intraoperative retinoscopy.
Table – 3 Difference between Final Refraction and IOL Implanted
| Difference between Final Refraction | No. of Eyes |
| -3.50 D to -1.25 D | 04 (22.22%) |
| -1.00 D to +1.25 D | 10 (55.55%) |
| >+1.25 D to +2.0 D | 04 (22.22%) |
Best corrected visual acuity was 6/60 to 6/12 in 6 eyes while it was FC 2 meter to FC 6 meter in 12 eyes. In some cases BCVA was better due to better retinal condition. While it was poor due to poor retinal condition in cases of severe proliferative diabetic retinopathy (Table – 4).
Table – 4 Best Corrected Visual Acuity
| Best Corrected Visual Acuity | No. of Eyes |
| 6/60 to 6/12 | 06 (33.33%) |
| FC 2 meter to FC 6 meter | 12 (66.66%) |
All previous retinal surgeries with silicone oil was done by one of the authors (Dr. APS), hence was very well aware about the retinal status. Therefore we decided not to remove silicone oil during surgery. But the problem came up about deciding the IOL power. Formulas are available to calculate IOL power but presuming that silicone oil would be
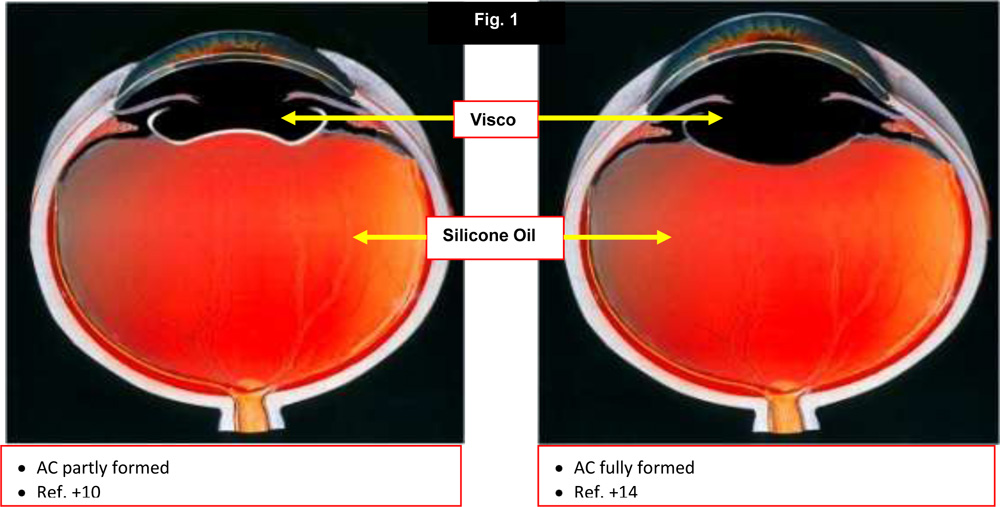
removed during cataract surgery. And as no definite formula is available, we decided to do intraoperative retinoscopy, which is our usual practice whenever IOL power cannot be decided during preoperative workup. We have also noticed that retinoscopy significantly differ when AC and Bag is not properly formed with visco (Fig.-1). Hence retinoscopy readings were taken with fully formed AC and Bag and appropriate foldable IOLs were placed 1’In the Bag’.
From postoperative refraction, one can see that there is little difference between these values and the IOL power used. However, the fluctuation in difference is on either side i.e. both hyperopic and myopic. In case if we would have used IOL power according to IOL master modified biometry readings, then the difference could have been worse. The visual acuity improved more where retina was healthy. By more careful retinoscopy and the experience, this difference can be reduced and intraoperative retinoscopy and postoperative retinoscopy can match better.
Summary
In this study, 18 eyes previously operated for vitreoretinal disorders with silicone oil, needed cataract surgery with IOL were included. As silicone oil removal was not advisable, we could not do accurate IOL power calculation from IOL master because no definite formula was available. From our experience, we calculated IOL power from intraoperative retinoscopy and we found that it was matching better with postoperative BCVA rather than with IOL power calculated from biometry.
References
- Smith RC, Smith GT, Wong D. Refractive changes in silicone filled eyes. Eye 1990; 4:230-234
- Hoffer KJ. Ultrasound velocities for axial eye length measurements. J Cataract Refract Surg 1994; 20:554-562
- Murray DC, Potamitis T, Good P, Kirkby GR, Benson MT. Biometry of the silicone oilfilled eye. Eye 1999; 13: 319–324