Dr. Shroff Ashok
Pranjivandas, S02064, Dr. Hardik Shroff, Dr.
Dishita Shroff
Chief Author : Dr. Ashok P. Shroff
Co-Authors : Dr. Hardik A. Shroff
Dr. Dishita H. Shroff
Introduction
Intraocular pressure reduces after uneventful phaco surgery with IOL implantation. The possible explanations are
1Thicker senile cataractous lens is replaced by thinner IOL, which makes anterior chamber deep and opens the angle of anterior chamber. This allows aqueous to flow through trabecular meshwork little freely.
2.During this procedure, glycosaminoglicon deposition is believed to be washed out leading to opening up of trabecular meshwork.
3.Another possibility is that it induces phagocytosis of meshwork debris.
4.One hypothesis is that it releases endogenous prostaglandin which in turn, increases uveoscleral outflow causing drop in IOP.
5.One more explanation given by workers is that Aqueous production is decreased due to increased traction on ciliary body. The sequence of occurrence is as follow. There is postoperative shrinkage of capsular bag which leads to increased traction on zonular fibres and ciliary body which causes less secretion of aqueous.
It is now possible to measure more accurately anterior chamber depth and angle of AC by anterior segment OCT, We decided to compare changes in angle of AC in relation with drop in IOP after cataract surgery in normotensive patients.
Material
80 eyes of 80patients with senile cataract and normal IOP were included in this study. 35 were male while 45 were female. RE was 47 and LE was 43. Their age varied from 41 to 74 years, mean being 63.5 years, Mean IOP was 15.7 mm of Hg (Range was from 13.50 to 17.0 mm of Hg). (Table – 1).
All patients had no other ocular or systemic diseases. During preoperative workup apart from routine biometry, IOP was carefully measured and recorded. Angle of AC and anterior chamber depth were measured by anterior segment OCT. This gives measurement of nasal and temporal angles only. Gonioscopy was performed in all cases for comparison purpose and to exclude closed angle cases.
Routine phaco surgery was done with foldable IOLs in the Bag. There was no intra or postoperative complication. All cases were again examined for IOP, ACD and angle of AC at the end of one month.
Results
All IOLs were properly placed in the Bag. Mean preoperative IOP was 14.61 mm of Hg, (range from 10 to 18 mm of Hg). It decreased to 11.62 mm of Hg (range from 8 to 13 mm of Hg). In all cases IOP reduced. The difference in reduction of IOP between pre and post was mean 2.99 mm of Hg (ranging from 1 mm of Hg to 6 mm of Hg – i.e. 20.46%).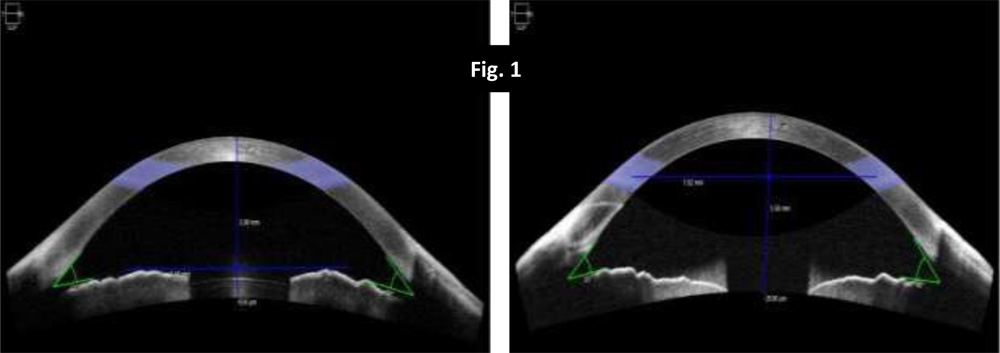
Similarly there was significant widening of angle of AC. Preoperative angle of AC on nasal side was mean 30.750 (range from 100 to 410), while temporal side was 32.380 (range from 200 to 400); Postoperative angle of AC on nasal side became 43.120 mean, (ranging from 320 to 520), while on temporal side it became mean 41.5, (ranging from 300 to 520). In all cases angle on both sides became wide.
And the difference between pre and post operation was mean 12.370, (range from 10 to 240) (40.22%) on nasal side and mean 9.120, (range from 10 to 280) (28.16%) on temporal side. (Fig. 1 & 2).
Preoperative anterior chamber depth was 3.31 mm mean, (ranging from 3.06 mm to 3.82 mm), which became 3.86 mm mean, (ranging from 3.56 mm to 4.32 mm). It suggests AC became more deep by 0.55 mm mean (16.61%), (ranging from 0.16 to 1.08 mm). (Table – 2 ). (Fig. 1).
Discussion
In this study, all eyes were non-glaucomatous, means normotensive. There was no intra and postoperative complication. In all cases foldable IOLs were well placed in the Bag. Now ACD and angle of AC can be measured more accurately by anterior segment OCT. We know that senile cataractous lens has thickness of 3.5 mm to 5 mm and it increases in all individuals. This makes ACD shallow as compare to young age. Moreover, senile cataractous lens is replaced by thinner IOL which usually has thickness of 0.60 mm to 1.08 mm. Therefore our results reveal that ACD become more deep by 16.61%. Now it has caused widening of angle of AC. By anterior segment OCT, angle can be measured in nasal and temporal area only. However, nasal angle became wide by 12.370 (40.22%) and temporal angle became wide by 9.120 (28.16%). This has helped in lowering IOP by 2.99 mm of Hg mean (20.46%), which is quite significant. It will be interesting to know what happens to ACD, angle of AC and IOP after 6 months, 1 year or 2 to 3 years. It has been mentioned in the literature that IOP reduction is more in cases of glaucomatous eyes but in our series, we also noticed significant widening of angle of AC due to deepening of anterior chamber which has reduced IOP significantly.
Summary
In this series, 80 normotensive eyes having senile cataracts were subjected to routine phaco with foldable IOL. All eyes were subjected to measure angle of AC and ACD by anterior segment OCT pre and post operatively. IOP was also recorded carefully. We found that there was significant widening of nasal angle 12.370 (40.22%) and temporal angle by 9.120 (28.16%). ACD also increased by 0.55 mm (16.61%) and IOP reduction was 2.99 mm of Hg (20.46%) which is quite significant.
Table – 1 Demography
| Total Eyes | Sex | Eye | Age | ||
| 80 | Male | Female | RE | LE | |
| 35 | 45 | 47 | 43 | 41 to 74 years (mean 63.5 years | |
| Mean IOP | 15.7 mm of Hg (Range from 13.50 to 17.0 mm of Hg) | ||||
Table – 2 Results
| Particular | ACD (mm) | Angle of AC (degree) | IOP (mm of Hg) | |
| Nasal | Temporal | |||
| Pre operative | 3.31
(Range 3.06 to 3.82) |
30.75
(Range 10 to 41) |
32.38
(Range 20 to 40) |
14.61
(Range 10 to 18) |
| Post operative | 3.86
(Range 3.56 to 4.32) |
43.12
(Range 32 to 52) |
41.50
(Range 30 to 52) |
11.62
(Range 8 to 13) |
| Difference | 0.55 (16.61%)
(Range 0.16 to 1.08) |
12.37 (40.22%)
(Range 1 to 24) |
9.12 (28.16%)
(Range 1 to 28) |
2.99 (20.46%)
(Range 1 to 6) |
References
1.Steuhl KP, Marahrens P, Frohn C, Frohn A. Intraocular pressure and anterior chamber depth before and after extracapsular cataract extraction with posterior chamber lens implantation. Ophthalmic Surg 1992;23:233–7.
2.Ken Hayashi et al. Changes in Anterior Chamber Angle Width and Depth after Intraocular Lens Implantation in Eyes with Glaucoma. Ophthalmology 2000: 107:4:698-703.
3.Brooks J. Poley, MD et al; Intraocular pressure reduction after phacoemulsification with intraocular lens implantation in glaucomatous and nonglaucomatous eyes. Evaluation of a causal relationship between the Natural lens and open-angle glaucoma; J Cat. Ref. Surg. Vol. 35, Nov. 2009 : 1946-1955
4.Suzuki R, Tanaka K, Sagara T, Fukiwara N. Reduction of intraocular pressure after phacoemulsification and aspiration with intraocular lens implantation. Ophthalmologica 1994; 208:254–258.
5.Suzuki R, Kuroki S, Fujiwara N. Ten-year follow-up of intraocular pressure after phacoemulsification and aspiration with intraocular lens implantation performed by the same surgeon. Ophthalmologica 1997; 211:79–83.
6.Nurit Mathalone, MD et al ; Long-term intraocular pressure control after clear corneal phacoemulsification in glaucoma patients :J Cat. Ref. Surg. Vol. 31, Mar. 2005 : 479-483
7.Meyer MA, Savitt ML, Kopitas E. The effect of phacoemulsification on aqueous outflow facility. Ophthalmology 1997; 104:1221–1227.