Dr.(Mrs ) Mayuri B Khamar, K03100,
Dr. MamidipudiRamakrishna Praveen,
Dr. Vandana C Nath,
Dr.Vasavada Abhay kumar Raghukant
Surgical Performance and postoperative outcomes after phacoemulsification in eyes with shallow anterior chamber
Dr Mayuri B Khamar
Dr Mamidipudi R Praveen
Dr Abhay R Vasavada
Dr VandanaNath
Raghudeep Eye hospital, Gurukul Road, Memnagar, Ahmedabad, India
Corresponding author
Dr Mayuri B Khamar M.S.
Glaucoma Center,Raghudeep Eye Clinic,
Gurukul Road, Memnagar,
Ahmedabad – 380052.
India.
Phone: 91-79-27492303, 27490909
FAX: 91-79-27411200
E-mail: mayuri@abhayvasavada.com
Introduction:
A shallow anterior chamber is a challenge during cataract surgery, because it reduces the already tight confines of the anterior segment of the eye.Few authors indicated shallow anterior chamber (the reduced anterior chamber depth) and the short axial length (AL) as factors responsible for the increased rates of perioperative complications in these patients. Day and associates have shown a strong relation between shallow anterior chamber or short axial length and perioperative complications.The other parameters coexisting include narrow anterior chamber angle, a thicker than normal lens with steeper curvature of the anterior surface, a more anterior lens position. Further in these eyes a narrow anterior chamber angle is thought to be important because a long-standing narrow angle or appositional closure may predispose to peripheral anterior synechiae formation, which may lead to uncontrollable rise in intraocular pressure (IOP).
A shallow anterior chamber may be associated with a spectrum encompassing a short axial length with or without a coexisting small corneal diameter.Auffarth et alhave documented that the small anterior segment, especially the shallow anterior chamber, is responsible for the high incidence of glaucoma and postoperative complications after cataract surgery while evaluating the anatomic parameters of relative anterior microphthalmos (RAM) after cataract surgery.Bharti and coauthors documented that eyes with RAM “pose a significant challenge” during phacoemulsification and after post cataract surgery a transient corneal edema because of the shallow anterior chamber and a smaller working space created by the small corneal diameter.However, the evidence on shallow anterior chamber and its association is very limited, and mainly formed by small case series.Soshould a shallow and narrow anterior segment determine or induce in some ways higher rates of complications, and any eye with a shallow anterior chamber should be more prone to intraoperative complications.To test this hypothesis, we designed this prospective study to compare whether performing cataract surgery in eyes with coexisting shallow anterior chamber in eyes with RAM is at increased risk (intraoperative surgical difficulties and complications and postoperative outcomes) of developing complications post cataract surgery when compared against eyes with isolated shallow anterior chamber with no other abnormalities.So the present study focuses to compare surgical difficulties and the impact of cataract surgery postoperatively on central corneal thickness, anterior segment inflammation and corneal endothelium morphology between the RAM and shallow anterior chamber.
Material & Methods:
This prospective, observational study comprised 120 consecutiveeyes with shallow anterior chambers undergoing phacoemulsification.at the Iladevi Cataract and IOL Research Center from June 2014 to June 2015. The Institutional Review Board approved the study and informed consent was obtained from all the patients before enrolling them.Of the 120 eyes with shallow anterior chambersthe following inclusion criteria were utilized to identify:Group I Shallow anterior chamber (n = 70eyes) had anterior chamber depth (ACD) ≤2.5 mm with no other morphologic malformation. Group II RAM (n = 50 eyes) defined as horizontal corneal diameter (HCD)< or =11 mm, ACD ≤2.2 mm, and axial length (AL)>20 mm.We used the following exclusion criteria: the presence of glaucoma, traumatic cataract, subluxated cataract, previous ocular surgeries, and allergy to dilating drops.A slit lamp biomicroscopy was done. Intraocular pressure (IOP) was measured with a Goldman applanation tonometer. Initially, the eye was anesthetized with 0.5% Proparacaineeye drops (Sunways, India). The central corneal thickness (CCT) was then assessed by ultrasonic pachymetry (Ocuscan, Alcon). Axial length (AL) and anterior chamber depth (ACD) were measured with optical coherence biometry (IOL Master, Zeiss) or an ultrasound A-Scan using the immersion technique (Ocuscan, Alcon).After a routine ophthalmic examination, all the subjects underwent specular microscopy with a noncontact specular microscope (SP2000: Topcon corporation, Japan) being used to calculate, the mean endothelial cell density (ECD) (cell/mm2), coefficient of variation (CV) in cell size, and percentage of six-sided cells (6A).
The AS-OCT was done by 2 experienced operators preoperative using a Visante AS-OCT device (Carl Zeiss Meditec AG);Standard resolution scans captured temporal and nasal quadrants (nasal–temporal 0 to 180 degrees) in 1 image with patients looking straight ahead and with a good central corneal reflex. All images were taken under the same dark conditions with the patient seated. Images in which the scleral spur could not be clearly detected were removed from analysis because quantitative evaluation of the anterior chamber parameters by AS-OCT depends on correctly identifying the scleral spur as the landmark.The SS was determined as the point where there was a change in curvature of the inner surface of the angle wall, often appearing as an inward protrusion of the sclera. The best image was selected and analyzed using custom software (Irido-corneal Module; Carl Zeiss Meditec). The angle opening distance(AOD) at 500 μm (AOD500) was defined as the perpendicular distance measured from the trabecular meshwork at 500 μm anterior to the scleral spur to the anterior iris surface; AOD750 parameters have similar definitions but with their respective distances from the scleral spur.Trabecular iris space area (TISA) up to 500 μm (TISA500) or 750 μm (TISA750) was defined as the area bounded by the corneal endothelium, trabecular meshwork, and anterior iris surface out to a distance of 500 μm or 750 μm from the scleral spur. The anterior chamber depth (ACD) was defined as the axial distance from theposterior corneal surface to the lens surface measured at the pupil center. After pupillary dilatationcataract was categorized as nuclear, cortical, posterior subcapsular (PSC), and mixed cataract or a combination of the above according to the zone of opacification. The hardness (density) of cataract was graded according to Emery’s and Little classification.
All surgeries were performed by a single, experienced surgeon (ARV) using a standardized technique of phacoemulsification on the Infiniti Vision System (Alcon Labs, USA). Multiquadrant, cortical-cleaving hydrodissection was performed. Phacoemulsification was performed using a standardized technique3,8,9. Standardized fluidic and ultrasound parameters were used in both groups for emulsification, depending on the grade of nuclear sclerosis. Torsional ultrasound was used in the burst mode with a minimum ultrasound off time of 200 milliseconds and a linear foot pedal control. Dispersive OVD (Viscoat®) was re-injected prior to beginning nuclear fragment removal, and subsequently halfway through fragment removal to protect the corneal endothelium. Bimanual irrigation / aspiration (I/A) was performed for cortex removal. In all eyes, a single-piece foldable aspheric, monofocalintraocular lens (AcrySof SN60WF IOL, Alcon Labs, USA) was injected in the bag using a motorized injector system and compatible cartridge (D cartridge). The OVD was aspirated using bimanual I/A with a linear vacuum of 500mmHg and a linear aspiration flow rate (AFR) of 30cc/min. Postoperatively, all patients used topical steroid eye drops 4 times a day for 2 weeks, after which the regimen was tapered by 1 drop for 3 weeks.
Corneal edema and uveal inflammation (cells, flare) were noted at each of the follow-up postoperativevisits at first day, 15 days, and 1 month respectively. Corneal edema was recorded as presence of Descemet’s folds. The uveal inflammatory response was noted in the form of flare and/or cells graded by Hogan’s criteria.ACD was performed preoperative, 15 days and 3 months postoperative.The CCT was performed postoperative 1 and 15 days, and 1 and 3 months respectively after cataract surgery.The AS-OCT was done 1 month after cataract surgery; the operators were masked to the results of the clinical ophthalmic examinations.
Results:
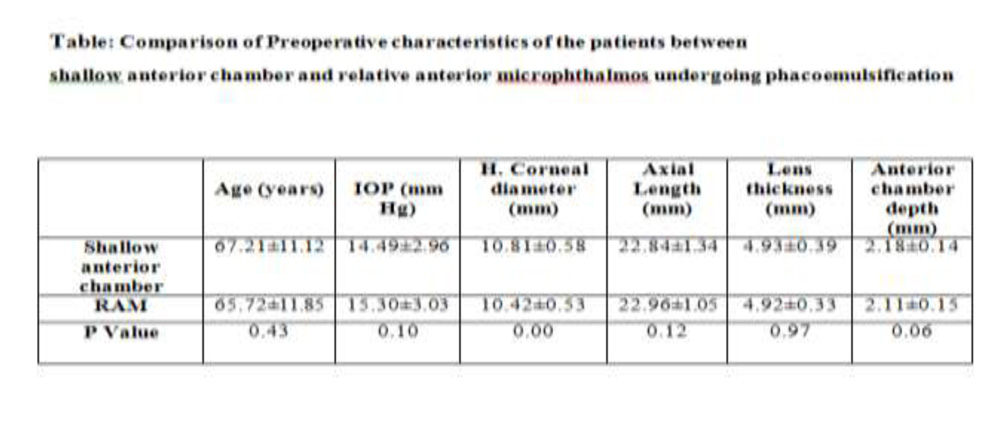
Table 2 shows comparison of the patients’ demographics and baseline data.Between Groups I and II the mean age, the mean axial length and the mean lens thickness was similar with no statistical significant difference.However, there was significant difference observed in the horizontal corneal diameter and anterior chamber depth between 2 groups.There was no significant difference in the distribution of grade of cataract according to Emery’s and Little classification.(Group1Vs Group 2: density of cataract ≤ Grade 3: 53 Vs 42 eyes P=0.236; > Grade 3: 17 Vs 8 eyes P=0.236).
Intraoperative performance:
Between the 2 groups there was no significant difference in total fluid used (Group I Vs Group II:100.02±23.2 Vs 103.83±30.5 ml, P=0.834), cumulative dissipated energy (Group I Vs Group II:17.52±8.28 Vs 21.65±10.22, P=0.177) and surgical clock time (Group I Vs Group II: 16.64±6.51 Vs 17.92±7.46, P=0.594).
While evaluating capsulorhexis, we observed in eyes with shallow anterior chamberanterior chamber dome maintained significantly morewhen compared against eyes with RAM (Group I Vs Group II: 20(40%Vs 8(11.4%) eyes P<0.001), while working space was maintained significantly more in eyes with shallow anterior chamber when compared against RAM (Group I Vs Group II: 52(74.3%) Vs 26 (52%) P<0.01) and full chamber maintenance was observed in equal number between the 2 groups.(Group I Vs Group II: 10(14.3%) Vs 4(8%) P=NS) eyes. In the present study while evaluating the plane of emulsification during fragment removal the surgeon could perform posterior plane emulsification in significantly more eyes with shallow anterior chamber when compared against RAM (Group I Vs Group II: 16(22.9%) Vs 4(4.2%) P=0.005). However the surgeon had to perform anterior plane phacoemulsification closer to the corneal endothelium more in eyes with RAM when compared against eyes with shallow anterior chamber.(Group I Vs Group II: 5(7.1% Vs 10 (20.8%) P=0.004). While in both the groups the surgeon performed phacoemulsification at iris plane in equal number of eyes between 2 groups.(Group I Vs Group II: 49(70%) Vs 36(75%) P=NS).There was no significant difference observed with the uveal trauma (iris prolapse during phacoemulsification between 2 groups. (Group I Vs Group II: 3(4.4%) Vs 6(12.5%) P=0.106). Only 1 eye in RAM developed posterior capsule rupture with intact anterior vitreous face and no vitrectomy was performed. There was no significant difference observed with the incidence of descemets detachment between the 2 groups. (Group I Vs Group II: 4(5.71%) Vs 4(8%) P=0.529). (Table 3).
The influence of cataract surgery on anterior chamber cells according to Hogan’s criteria was statistically significantly more in eyes with RAM when evaluated on the 15 days and 1 month postoperative days when compared against eyes with shallow anterior chamber. While there was no significant difference observed between the two groups when evaluatedon first postoperative day. Similarly analyzed, the influence of cataract surgery on anterior chamber flare according to Hogan’s criteria was statistically significantly more in eyes with RAM when evaluated on the 15 days and 1 month postoperative days when compared against eyes with shallow anterior chamber. While there was no significant difference observed between the two groups when evaluated 1 month post cataract surgery.
When we evaluated the corneal clarityon postoperative day 1slit lamp examination revealed that there were more number of eyes in shallow anterior chamber with clear cornea when compared against RAMattaining statistically significant difference between 2 groups. (Clear Cornea:Group I Vs Group II: 47(67.1%) Vs 24 (48%).However there was no significant difference in eyes who developed stromal edema with Descemet’s membrane folds between the 2 groups on the postoperative day 1.(Group I Vs Group II: 23(32.9%) Vs 26(52.0%).At 15 days post cataract surgery there were more number of eyes in shallow anterior chamber with clear cornea when compared against RAMattaining statistically significant difference.(Clear Cornea:Group I Vs Group II: 55(88.5%) Vs32 (66.7%) eyes P=0.03). However, there were more number of eyes still in RAM persistingstromal edema with Descemet’s membrane folds even at 15 days post cataract surgery when compared against eyes with shallow anterior chamber (Group I Vs Group II: 8(12.7%) Vs 16 (33.4%) eyes P=0.03. At 1 month follow up all eyes in both the groups achieved clear cornea.
Preoperatively, the mean CCT in Group I was 531.24±42.61µ, while in Group II, it was 521.00±28.07µ with no statistically significant difference between the two groups (P =0.15). Postoperatively, in all the eyes there was a definitive increase in CCT postoperatively. On the first postoperative day and 15 days the mean CCT was significantly more in eyes with RAM when compared against eyes with shallow anterior chamber (1st postoperative day CCT: Group I Vs Group II: 539.42 ± 49.3 µ versus 561.40 ± 40.09 µ P< 0.014, 15 days postoperative Group I Vs Group II: 536.57 ± 44.30 µ versus 554.62 ±40.8 µ, P<0.04). After 1 and 3 months post cataract surgery there was no difference observed between the two groups. (postoperative 1 month CCT:Group I Vs Group II: 546.81±52.3µ Vs 553.38±46.9 µ P=0.84,postoperative 3 months CCT:Group I Vs Group II: 524.47±24.96µ Vs 531.78±41.2µ P=0.338) respectively. Preoperatively, the mean ECD in Group I was2351.85±405.38 cells/mm2, while in Group II, it was 2493.48±394.83cells/mm2. Three months postoperatively, the mean ECD in Group I was 2157.84±392.74± cells/mm2, and in Group II, it was 2246.61±570.29cells/mm2 (Table7). Thus there was no statistically significant difference in ECD from preoperative to postoperative periods when the two groups were compared (P =0.480, Table). Similarly there was no statistically significant difference in CV and 6A observed from preoperative to postoperative periods when the two groups were compared.
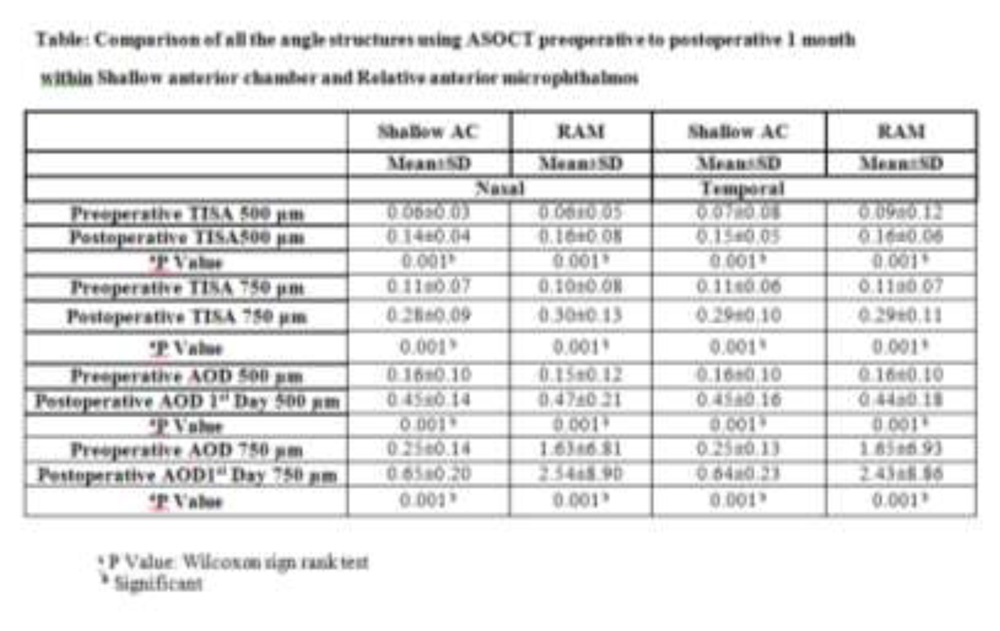
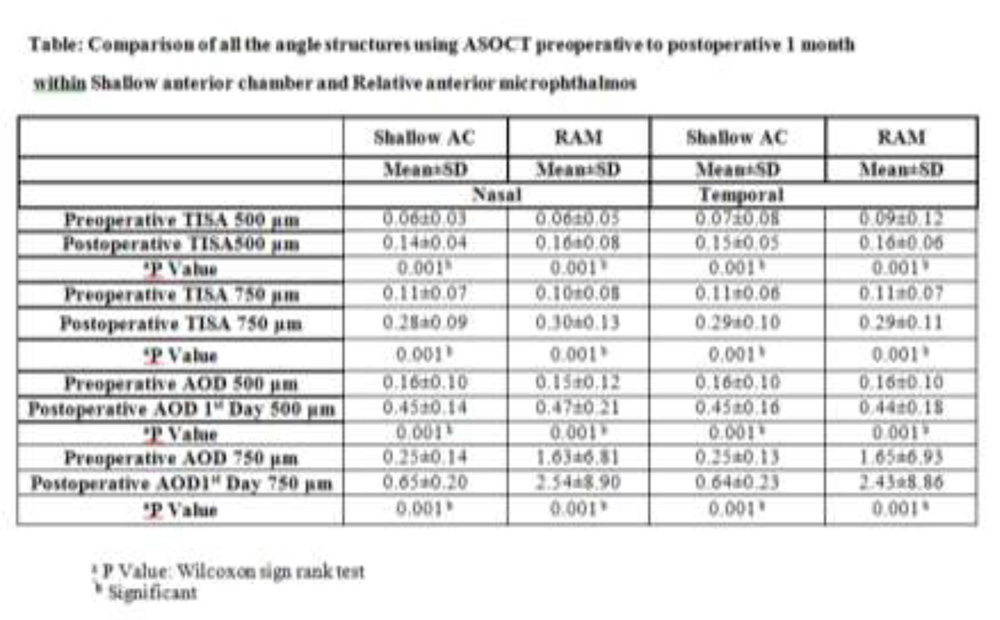
All angle parametersanalyzed with AS-OCT like ACD, AOD500μm and 750μm and TISA500μm and 750μm showed a significant increase after cataract surgery for both the nasal and temporal angles when compared within the groups.However,between the 2 groups when the same parameters analyzed for the mean difference from preoperative to postoperative 1 month showed no significant difference after cataract surgery.
Discussion:
Improvements in phacoemulsification technology have allowed cataract surgical techniques to evolve so as to obtain increased levels of efficiency in all complex ocular situations. Some of the associated collateral benefits when utilizing these optimization efforts are protecting the corneal endothelium against damage and reducing trauma to other intraocular tissues which may lead to subsequent complications such as posterior capsule rupture and vitreous loss. The crowded anterior segment presents one of the most challenging situations for phacoemulsification surgeons. Surgery in eyes with relatively small anterior segments can be hampered by the physical space constraints.
In the present series we found difficulty in performing capsulorhexis and performing phacoemulsification in eyes with RAM when compared against shallow anterior chamber. We believesmall corneal diameter and shallow anterior chamber led to “less working space” in eyes with RAM. Further in the present study the surgeon could perform posterior plane emulsification in only 4 eyes in eyes with RAM as the surgeon experienced crowding in the eye while performing surgery because of a small anterior segment when compared against shallow anterior chamber.Further owing to the perceived reduced working space, it was difficult to perform posterior plane emulsification. The fragments remained close to the endothelium during their removal. This was detrimental to intraocular structures of the eye like the corneal endothelium, iris, and posterior capsule.
In the present series there was only one eye who developed posterior capsule rupture in eyes with RAM. We observed a relatively low rate of perioperative complications as we attribute to the understanding and implementing the techniques and also improved phaco/fluidics settings we employed.Jung and associates while evaluating cataract surgery in eyes with nanophthalmos and relative anterior microphthalmos observed a PCR rate of 11%. Steijns et al reported a PCR rate of 7% with cataract surgery in patients with nanophthalmos. Day et al in their series none of the patients developed PCR in eyes undergoing phacoemulsification with microphthalmos and nanophthalmos.In another retrospective study while evaluating cataract surgery in small adult eyes the authors have not reported PCR in their series.In our previous report while evaluating intraoperative performance and surgical outcome in eyes with RAM undergoing cataract surgery we reported posterior capsule rupture in only 2 (2.38%) eyes.Intraoperatively, we noticed that using lower aspiration parameters allowed us to continue emulsifying the lens fragments either at a posterior plane or at the iris plane away from the corneal endothelium until we had removed all the fragments without risking posterior capsule rupture or uveal tissue aspirationThe advantages of using low parameters have been demonstrated previously by a few authors. Few techniques like Osher’s “slow-motion phacoemulsification” approach and Vasavada and co-authors “step down technique” demonstrated the safety of using low fluidic parameters and graded reduction in parameters during phacoemulsification without the possibility of causing posterior capsule rupture. The essence of these techniques lies in the enhanced safety they provided during the entire fragment removal procedure.
The most frequent complication after cataract surgery was temporary corneal edema, and increased anterior segment inflammation which occurred in both the groups. However, both the edema and anterior segment inflammation cleared up in all these eyes within 1 month after surgery. Corneal edema and anterior segment inflammation was significantly greater in RAM eyes even at 1 week, compared with shallow anterior chamber.We believe that RAM eyes this could be because of less working space created by a small corneal diameter and a shallow anterior chamber where the surgeon struggles to keep the fragments away from the endothelium in the posterior plane, they often end up in the anterior chamber during phacoemulsification. The intraoperative struggle and the lens fragments remain close to the endothelium during their removal owing to less working space led to corneal edema and anterior segment inflammation in RAM eyes in the immediate postoperative period. No eye developed corneal decompensation.
Jung et al.reported that anterior segment inflammation was higher in nanophthalmic eyes than in control eyes; however, the difference was not statistically significant between the nanophthalmic, relative anterior microphthalmic, and control groups. Day et al. reported severe postoperative anterior uveitis in 4 of 103 nanophthalmic eyes, which resolved with topical steroid treatment. Auffarth et al. found fibrin reactions in the anterior chamber in 3 of 62 (4.8%) relative anterior microphthalmic eyes. We did not find significant uveal inflammatory response in these eyes, presumably because of our surgical technique with emphasis on avoiding iris touch and uveal trauma during phacoemulsification. As a result of low aspiration parameters, there is reduced turbulence within the anterior chamber, and we speculate that this might lead to reduced breakdown of the blood-aqueous barrier.
It is well documented that corneal edema, change in CCT, and corneal endothelial cell loss are indicators of surgically induced corneal trauma. It has also been suggested that corneal thickness provides a measurement of the amount of surgically induced endothelial injury. Some authors have further suggested that an increase in CCT on the first postoperative day correlates with surgical trauma inflicted on the endothelium and it is proportional to cell loss at three months. In the present study despite using low parameters in both the groups we found significant increase in the central corneal thickness in eyes with RAM when compared against shallow anterior chamber upto 15 days post cataract surgery. We believe increase in CCT in the early postoperative period in RAM eyes could be because during phacoemulsification because of a small corneal diameter and a shallow anterior chamber the lens fragments remain close to the endothelium during their removal owing to less working space.
Further there was no significant difference in the endothelial cell density between the two groups at 3 months postoperatively. We noticed that using lower aspiration parameters allowed us to emulsify the lens fragments at a posterior plane away from the corneal endothelium as a result, the incidence of mechanical contact of the lens fragments with the corneal endothelium may also be lowered. With lowered fluid flow, there is reduced turbulence within the anterior chamber, and we speculate that this might lead to reduced endothelial damage as well as reduced breakdown of the blood-aqueous barrier. Hayashi and co-authors16 have shown that nuclear fragments coming in mechanical contact with the endothelium are the most important risk factors for intraoperative endothelial injury. Further they found that the total amount of ultrasound energy and the hydrodynamic flow in the anterior chamber may presumably cause damage to the corneal endothelial cells.
Anterior segment optical coherence tomography (AS-OCT) provides objective highresolution images of the anterior chamber angle (ACA) structures. Quantitative data about angle structures in shallow anterior chambers are very limited to date.Clinical experience has shown that cataract surgery deepens the anterior chamber of the operated-on eye and widens its angle.This study also demonstrated changes in the anterior segment configuration after phacoemulsification and IOL implantation in both the groups as measured quantitatively by AS-OCT. This study also confirmed angle widening and chamber deepening after cataract surgery, as other studies have previously demonstrated.In another case series targeting nanophthalmos, after phacoemulsification and IOL implantation authors found AOD500, and TIA increased after cataract surgery and concluded that cataract surgery deepened the anterior chamber and widened the anterior chamber angle in nanophthalmic eyes.In the same study the observation of all eyes in this study had a plateau iris configuration, and found attenuation of the plateau iris configuration by lens extraction in eyes with nanophthalmos. Sharan et alsimilarly demonstrated increased anterior chamber volume, ACD and anterior chamber angle as measured by Pentacam in a case of nanophthalmos. Kurimoto and coauthors found that the more shallow the preoperative anterior chamber was, the greater the postoperative change of the chamber was; and the more narrow the preoperative angle was, the greater the postoperative change of the angle was.We believe the forward shift of the iris caused by the lens may be greater in eyes with a shallow anterior chamber and a narrow angle than in normal eyes. Therefore, the backward shift of the iris induced by lens removal may have been greater in eyes with a shallow anterior chamber and a narrow angle, which makes the anterior chamber deeper and the angle wider.
An importantlimitation of this study lies in thesample size which we have not calculated.In conclusion relative anterior microphthalmos posed more intraoperative surgical difficulties and early postoperative complications.In eyes with RAM there was an increased anterior segment inflammation and also increase in central corneal thickness at early postoperative period when compared against eyes with shallow anterior chambers. RAM and shallow anterior chamber impacted similar changes in anterior chamber configuration after cataract surgery as measured by AS-OCT at 1 month postoperative. In the present series these results indicate that the role of cataract surgery has undergoneconsiderable evolution and that such procedures are now viable options. With optimal preoperative management, careful selection of the intraocular lens, meticulous surgical technique, and appropriate awareness of the potentialintra- and postoperative complications, cataract surgery can be successfully performed in eyes with shallow anterior chamber with acceptable postoperative results.