Dr. Sunil
Brijendra Jain, J07729, Dr. Ashutosh Khandelwal,
Miss. Gargi Saxena, Dr. Rajnish Gourh
Chief and Presenting author – Dr.Sunil Brijendra Jain
(AIOS No. 07729)
Co-authors -Dr.Ashutosh Khandelwal,
Dr.Rajnish Gourh and Miss Gargi Saxena
Cataract has been documented to be the most significant cause of bilateral blindness in India where vision <20/200 in the better eye on presentation is defined as blindness. In India cataract has been reported to be responsible for 50-80% of the bilaterally blind in the country.1-6 Recent data from the World Health Organization (WHO) shows that there is a 25% decrease in blindness prevalence in India.7 India is committed to the goal of elimination of avoidable blindness by 2020 in line with the Global Vision 2020: the right to sight Initiative.
An important step towards this goal has been the Lifeline Express (the world’s first hospital on a train) an initiative by Impact India Foundation. Impact India – Lifeline Express commenced its adventurous journey with three coaches on 16th July 1991. Subsequently, on 12th July 2007, a custom- built, five coach, new Lifeline Express was inaugurated...8
Thus, it has been 25 glorious years of combating cataract blindness in rural India and has proved a role model for the rest of the world.( Silver Jubilee was celebrated in 2016 ) .
Thus, it has been 25 glorious years of combating cataract blindness in rural India and has proved a role model for the rest of the world. (Silver Jubilee was celebrated in 2016).
The purpose of this mobile hospital is to offer on-the-spot surgical treatment free of cost for curative interventions to the disabled poor in rural India using the entire Indian railway network in a fully equipped and administered hospital train. As disabled and poor people cannot reach a hospital, the hospital should reach them. The mobile hospital also creates awareness among people.
MATERIALS AND METHODS: Cataract surgeries are performed in the Lifeline express launched by Impact India Foundation. It consists of five coaches.
- 1- Generator cum staff car.
- 2- Office/Store/Sterilizer car.
- 3- Operation Theater car 1.
- 4- Operation Theater car 2 &
- 5- Conference/Auditorium car.
Out Patients Department and post-operative ward are arranged separately close to the train.
Preparation of site: Cleaning, leveling of land.
Planning: Use of public buildings if available or tents to be erected.
Permission for:
- Movement of LLE to station.
- Parking of LLE
- Provision of water and electricity.
- Sanitation
- Use of railway’s: 1- Communication system 2- Maintenance Set up
- Preparation of project site.
Publicity Is done via media, announcements, distribution of handbills, display of banners/posters/flags, cable TV and radio broadcast. The LLE is parked at a railway siding for the entire period. Primary screening of patients by medical officer and then by Ophthalmic surgeon. IOL power calculation by optometrist. Rule out Diabetes mellitus and hypertension.
Routine fumigation of OT and sterlization of instruments are done. Pre-operative antibiotic drops are instilled and pupillary dilatation is done.Peribulbar block is given. Small Incision Cataract Surgery with IOL Implantation is performed. Patient are shifted to Post-operative ward. Eye patch is removed next day. Uncorrected Visual Acuity and pinhole vision is tested. Post-operative steroid antibiotic and cycloplegic drops are started.
Project Profile: On an average, the LLE provides medical relief including surgeries to about 5000 people per project, lasting for about 3-4 weeks, 10 projects a year. There are two fully equipped Operation Theatres on the train with a total of five Operating tables. The following types of corrective surgeries, other medical services and health education are provided to the rural poor, totally free-of-cost, on the Lifeline Express:
1.Orthopaedic: Correction of post-Polio contractures, correction of Club-Foot deformities, lower limbs, generally up to the age of 15 years, barring Cerebral Palsy.
2.Ophthalmic: Cataracts, Intra Ocular Lens implants.
3.Middle ear operations: Tympanoplasty / Myringoplasty /Mastoid surgeries
4.Plastic Surgery: Cleft lips, Burn contracture release and tongue tie release.
5.Dental and Oral Health Hygiene services- Scaling, filling and extractions
6.Epilepsy treatment.
7.Health Education Programme: Educating Health Workers/Adolescent girl students about Reproductive, Maternal & Child Health, Puberty, Menstruation Cycles, Anaemia, Marriage & pregnancy etc..
8.Oral, Breast & Cervical Cancer Detection & Control Programme
Each type of surgery is carried out by the donated services of 3-5 Surgeons, 2-3 Anaesthetists, 6 Operation Theatre Technicians, 8 Medical Assistants or nursing staff (for Pre, Intra and Post operative care) and some support staff. Availability of state-of-the-art equipment in the train which facilitates efficient surgeries is one of the major success factors of the LLE and is well appreciated by the volunteer surgeons.
Team from INDIRA GANDHI EYE HOSPITAL AND RESEARCH CENTER (IGEHRC), a tertiary care Hospital in Lucknow, U.P.,India has contributed in ten of these projects from 2005-2016.
This hospital sends a team of Ophthalmologists, Optometrists, Nurses, Organizers, and other Volunteers. This is an example of an Institute offering voluntary services to LLE in a symbiotic relationship.
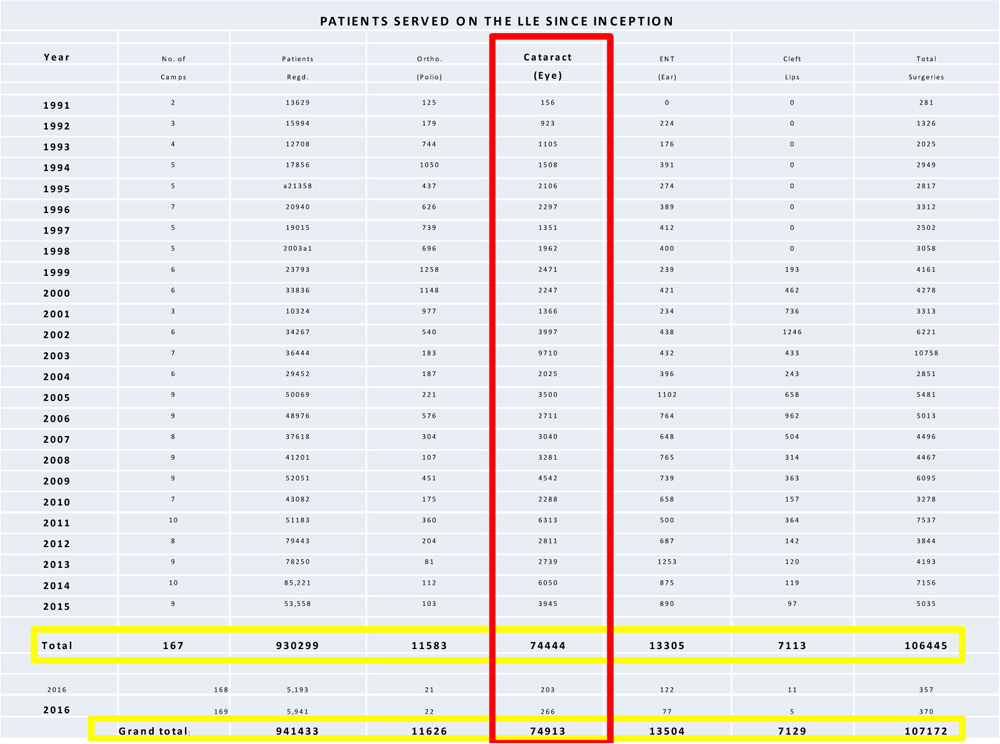
RESULTS: Until 8th march 2016, 170 projects have been completed since July 1991.100 districts in 19 states of India have been covered. Total number of cataract surgeries performed from 1991 until February 2016 is 74,913(169 projects).Data of the last project is not included as it was completed few days before submitting the abstract.
The number of surgeries at Zahirabad Station in September 2014 was 590. This is an example of one of the projects. Pre-operative and Post-Operative Best Corrected Visual Acuity (BCVA) of 161 out of these 590 patients were randomly selected and the data was applied in statistical analysis (paired t test- two tailed hypothesis) which showed a statistically significant improvement in BCVA. The value of p is<0.00001.The result is significant at p<0.05.
| Difference Scores Calculations |
| Mean: -1.02 |
| μ = 0 |
| S2 = SS⁄df = 40.17⁄(161-1) = 0.25 |
| S2M = S2⁄N = 0.25⁄161 = 0.00 |
| SM = √S2M = √0.00 = 0.04 |
| T-value Calculation |
| t = (M – μ)⁄SM = (-1.02 – 0)⁄0.04 = -25.82 |
| The value of t is -25.820463. The value of p is < 0.00001. The result is significant at p ≤ 0.05. |
DISCUSSION: Cataract blindness, one of the significant social issues in India with great economic impact and an annual incidence of approximately 2 million. Presenting vision is used to assess patient’s day to day social and physical functions, so community based programme is required to control blindness. Blindness due to other causes like glaucoma, demands greater challenge to public health since screening at community level is uncertain. 9
India is the first country which started blindness control programme to fight against preventable blindness .The available figures for cataract surgery in India over the period 1989-2005, show that there has been an increase of 238,000 surgeries per year over the 16 year period and LLE has contributed in its own way in increasing the number of cataract surgeries.
Imagine the plight of a patient with bilateral mature cataract, the sole breadwinner of his family with insufficient money to reach a hospital for surgical treatment from a remote area. The sight loss of an adult can rupture the household economy, whether a breadwinner becomes another dependent mouth to feed or a grandmother is no longer able to provide care for the children. This is the valuable contribution of LLE moving from one station to another and providing quality medical services to those who have no access to medical care.
CONCLUSION: The results clearly indicate that this is a unique concept in combating treatable blindness due to cataract, virtually at the doorstep of the patients. However, this is possible only by the combined efforts of the Government, voluntary agencies, voluntary medical and paramedical professionals , the sponsor or collaborator, LLE and the Indian railways The fact that this project has been replicated with four LLE trains in China, two in South Africa and Riverboat hospitals in Bangladesh and Cambodia proves its success and tremendous potential. This may be replicated by other nations where a similar need and situation exists.

LIFE LINE EXPRESS STAMPS WERE ISSUED IN 2009 IN APPRECIATION OF ITS SELFLESS SERVICE.
REFERENCES:
1-Thulasiraj RD, Nirmalan PK, Ramakrishnan R, Krishandas R, Manimekalai TK, Baburajan NP, et al . Blindness and Vision Impairment in a Rural South Indian Population: The Aravind Comprehensive Eye Survey. Ophthalmology 2003; 110:1491-8.
2-Thulasiraj RD, Rahamathulla R, Saraswati A, Selvaraj S, Ellwein LB. The Sivaganga eye survey: I, Blindness and cataract surgery. Ophthal Epidemiol 2002;9:299-312.
3-Nirmalan PK, Thulasiraj RD, Maneksha V, Rahmathullah R, Ramakrishnan R, Padmavathi A, et al . A population based eye survey of older adults in Tirunelveli district of south India: Blindness, cataract surgery and visual outcomes. Br J Ophthalmol 2002;86:505-12.
4-Murthy GV, Gupta S, Ellwein LB, Munoz SR, Bachani D, Dada VK. A Population-based Eye Survey of Older Adults in a Rural District of Rajasthan: I, Central Vision Impairment, Blindness and Cataract Surgery. Ophthalmology 2001;108:679-85.
5-Mohan M. National Survey of Blindness-India. NPCB-WHO Report. New Delhi: Ministry of Health and Family Welfare, Government of India; 1989
6-Mohan M. Collaborative Study on Blindness (1971-1974): A report. New Delhi, India: Indian Council of Medical Research; 1987. p. 1-65.
7-Resnikoff S, Pascolini D, Etyaale D, Kocur I, Pararajasegaram R, Pokharel GP, et al . Global data on visual impairment in the year 2002. Bull WHO 2004;82:844-51.
8-Operating Manual of Impact India- Lifeline Express.
9-Wormald Richard P.L., Rauf A.– Glaucoma screening. J Med Screening.2:109-114,1995.