Dr. Manisha Chhabra
Acharya, A09526, Dr. Umang Mathur, Mr. Lokesh
Chauhan, Dr. Dubey Suneeta
Improvement in Eye bank Tissue utilisation through Quality Assurance Initiatives
Manisha Acharya, Animesh Das, Suneeta Dubey, Umang Mathur, A K Singh, Lokesh, Prem Singh
ABSTRACT
Objective: To assess the impact of implementation of quality assurance program on corneal tissue utilisation in Eye bank.
Design: Quality intervention study
Methods: A Quality Assurance (QA) program was implemented in phased manner in the eye bank. This included the development of leadership, protocol development for all eye bank processes and an upgrade of infrastructure. Gap analysis was done to identify areas of improvement. The processes were updated according to the report of gap analysis. New standard operating procedures (SOP) were made. Training of eye bank staff was done on these new SOPs and good documentation practices. The QA program also included ongoing monitoring and evaluation of activities, identification of problems and development of plans for corrective actions. Indicators were identified to monitor and measure the improvement. The indicators included per month utilisation rate of corneas and mean transplants per year. Internal audits were conducted to measure the compliance with regulatory requirement. Pre-intervention and post-intervention data were collected and analysed.
Results: The quality assurance commenced in 2011 at the Eye bank. To assess the impact, data from 2005-2012 was compared with data from 2013-2015. Utilisation of collected corneas was increased from 53% to 68% after implementation of QA. Average collection per year was increased from 274cornea to 983 (3.7 times). Mean transplant per year was increased from 154 corneas to 658 corneas (4.2 times). Mean hospital cornea retrieval program (HCRP) collection per year was increased from 187 to 566. The mean utilisation of HCRP collection was increased from 46% to 73%
Conclusion: Implementation of QA program increases utilisation of corneal tissue facilitating a sustained increase in total transplants each year thereby contributing towards eradication of treatable corneal blindness
Introduction
Dr. R Townley Paton realised the importance and need of eye bank for procurement of corneal tissues and established the first eye bank in 1944 in New York. From its nascent stage, eye banking has evolved since then all over the world. Improvement in corneal storage, use of good quality corneal tissue, good network of communication and transportation among eye banks have contributed to increasing the utilisation of donor tissue.
The eye bank association of India (EBAI) with the collaboration of National Programme of Control of Blindness(NPCB) and other government and non-government organisations have made various amendments to improve the corneal procurement rate in India.(2014 amendment ) They have promoted various programmes for certification of eye bank technicians and counselors, developed written guidelines and policy for the operation of eye banks (Eye bank SOP 2013) to improve standards of eye banking in India.
There are 700 eye banks and collection centres in our country. The total corneal donation was 50,000 in the year 2015 and approximately 25,000 transplants were performed in this year. With an utilisation rate of 50%. (Verbal communication EBAI) the goal of EBAI is 1 lakh corneal transplant per year to decrease corneal blindness in India. This goal can be achieved by enhancing the corneal donations and its utilisation which can be achieved by increasing quality assurance for safety of corneal tissue for transplantation.
The last few years have seen Eye banking reinventing itself and are getting transformed where Quality is the foremost guiding principles.
It’s not all about numbers anymore. Maintenance of integrated quality assurance programme for eye bank is mandatory. Quality Assurance is needed for equitable distribution and timely availability of corneal tissue to the corneal surgeons, effectiveness and efficiency, safe utilisation of tissue and infection control. An Integrated quality assurance programme includes improving medical equipment and facilities in eye bank, risk management, proper record maintenance and documentation, safe utilisation of tissue and infection control and external regulations.
Aim:
To assess the impact of implementation of quality assurance programme on corneal tissue utilization in Eye bank
Design: Quality intervention study
Materials and Methods:
This Quality intervention study was conducted at Dr Shroff’s charity Eye Hospital Eye bank after approval from the institutional research committee.
A Quality Assurance (QA) programme was initiated in a phased manner in the eye bank in 2011. Gap analysis was done to identify areas of improvement. The areas of improvement identified were leadership development, capacity building and protocol development for all eye bank processes. A need to upgrade the infrastructure was realized which was done in due course.
After review of gap analysis report, the QA programme was initiated with timelines and monitoring .A focused group was involved in the preparation of policies and up gradation of processes. The changes were discussed and reviewed by all stake holders and were in compliance with Regulatory Requirements of NPCB Guidelines. A new standard operating procedures (SOP) manual was formulated. Training of eye bank staff was done on these new SOPs and good documentation practices were implemented.
Indicators were identified to monitor and measure the improvement. The major indicators were;
- Collection rate: Total number of donor corneas retrieved (per annum). Further analysis, based on our four point strategy was done
2 Utilisation rate: Total number of donor corneas used for transplantation / collection rate (per annum).
3 Discard rate: Number of donor corneas deemed unsuitable for transplantation / collection rate (per annum)
4 Adverse reaction rate: Number of keratoplasties afflicted by adverse reactions / total number of keratoplasties performed (per annum)
The indicators of collection and utilisation were analysed periodically.The reasons for discard of tissues were documented and discussed with The stake holders on a monthly basis.
The QA programme also included ongoing monitoring and evaluation of activities, identification of problems and development of plans for corrective actions. Internal audits were conducted to measure the compliance with regulatory requirements. In case of non compliance to SOP repeat training was done for the concerned staff. Then Incident management and corrective and preventive action (CAPA) were introduced. Thus system failure leading to errors was identified and preventive measures were taken. The Quality Assurance programme was implemented in 2012.
A parallel scalable strategy for improving eye bank performance and productivity was also initiated which had 4 components of:
- Hospital Cornea Retrieval Programme through Eye Donation Councilors
- Telephonic Screening by Tele-councilors
- Building up Nodal Centers in Urban Agglomeration within 3 hours of travel distance from Eye bank and
- Voluntary donations.
Transformational success was dependant on open dialogue from all members of the team, irrespective of position within the organizational hierarchy. With this approach in mind from the outset, not only did we manage to foster greater confidence and pride within our team, but we also achieved an equitable platform for critical appraisal of each new idea proposed in pursuit of our objectives.
This empowerment had a direct effect on the quality of work by each of our technicians and administration staff, with each role essential in improving the overall quality of our eye bank supply chain. Hence the QA programme was possible through the collective teamwork of our eye bank staff.
The data from 2005-2012 (pre intervention period) and from 2013 to 2015 (post intervention period) was collected and analysed.
Results:
The data from 2005-2012 (pre intervention period) was compared with the data from 2013 to 2015 (post intervention period) to analyse the effectiveness of Quality Assurance Programme.
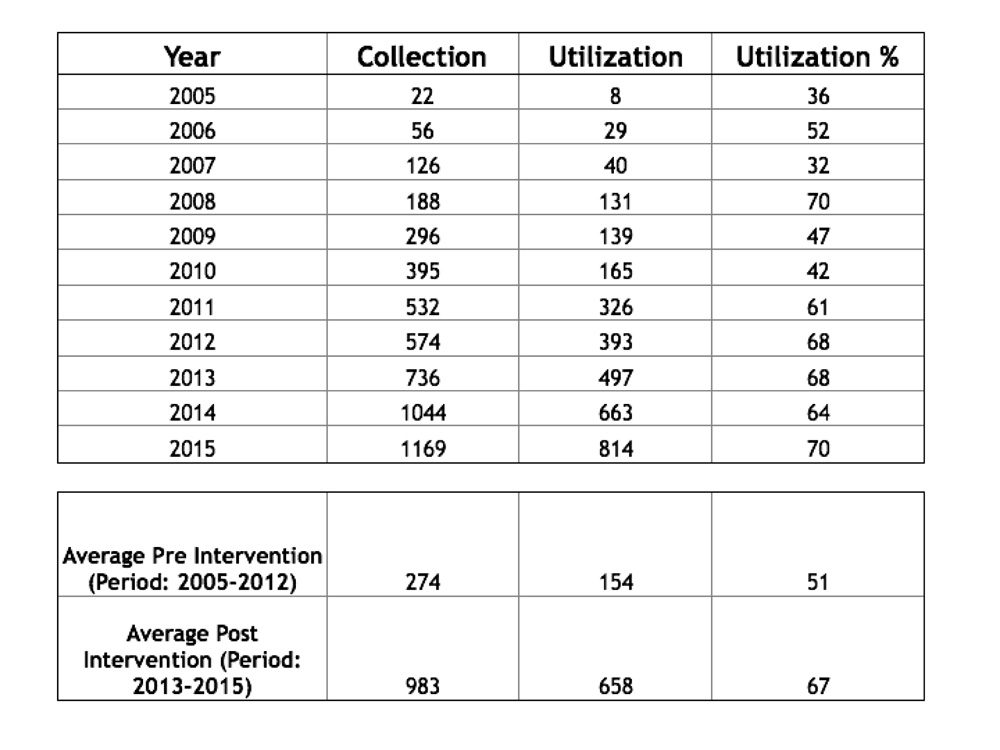
The collection of corneal tissue improved significantly in the post intervention period. (Graph-1) when compared from the pre intervention period. The average collection increased from 274 corneas in pre intervention period to 983 corneas in post intervention period, which was 3.7 times. The increase in collection was also related to the four point scalability strategy.
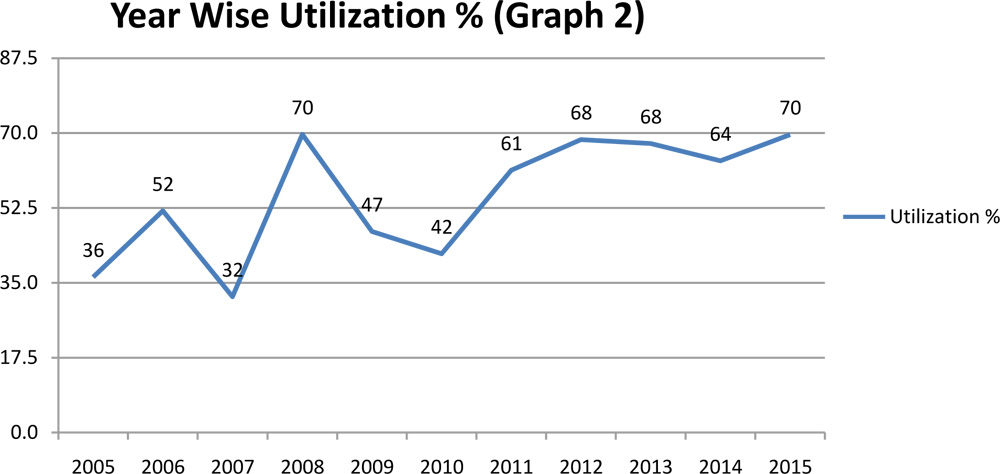
The average utilisation of corneal tissues increased from 154 corneas in the pre intervention period to 658 corneas in the post intervention period. There was 4.2 times increase in the utilisation of the corneas in the post intervention .The utilization percentage increase from 41% in pre intervention period to 73%in post intervention period (Graph 2).
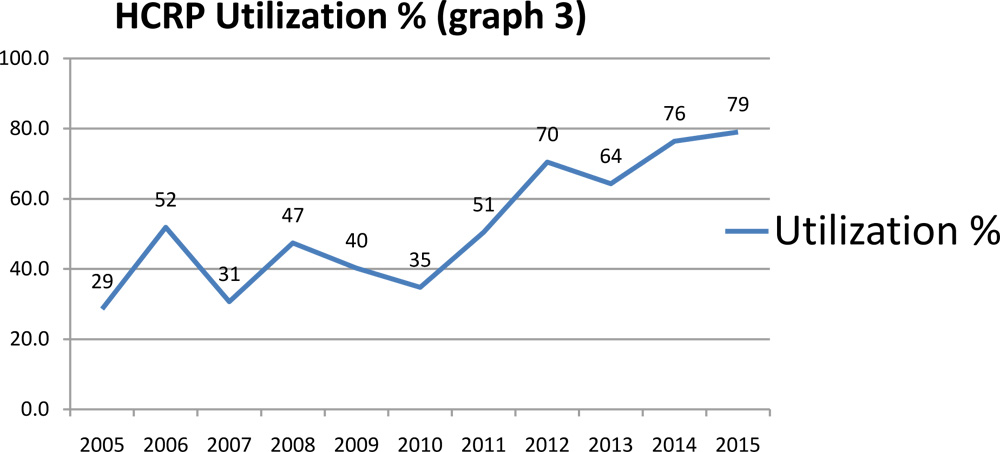
The mean collection of corneal tissue through HCRP( Hospital corneal retrieval programme ) per year increased from 187 corneas to 566 corneas .The average utilisation of the corneal tissue through HCRP collection increased from 41% in pre intervention period to 73% in post intervention period .(Graph-3)
The secondary impact of quality assurance was also seen. The creation of quality culture in eye bank stimulated the effort for continuous quality improvement. This increased the job satisfaction among the eye bank staff. The reputation among various stakeholders improved. A decrease in the cost of tissue processing and distribution was noted. Thus QA programme demonstrated the credibility and a commitment to quality and accountability which ensured patient safety leading to increased patient
satisfaction. 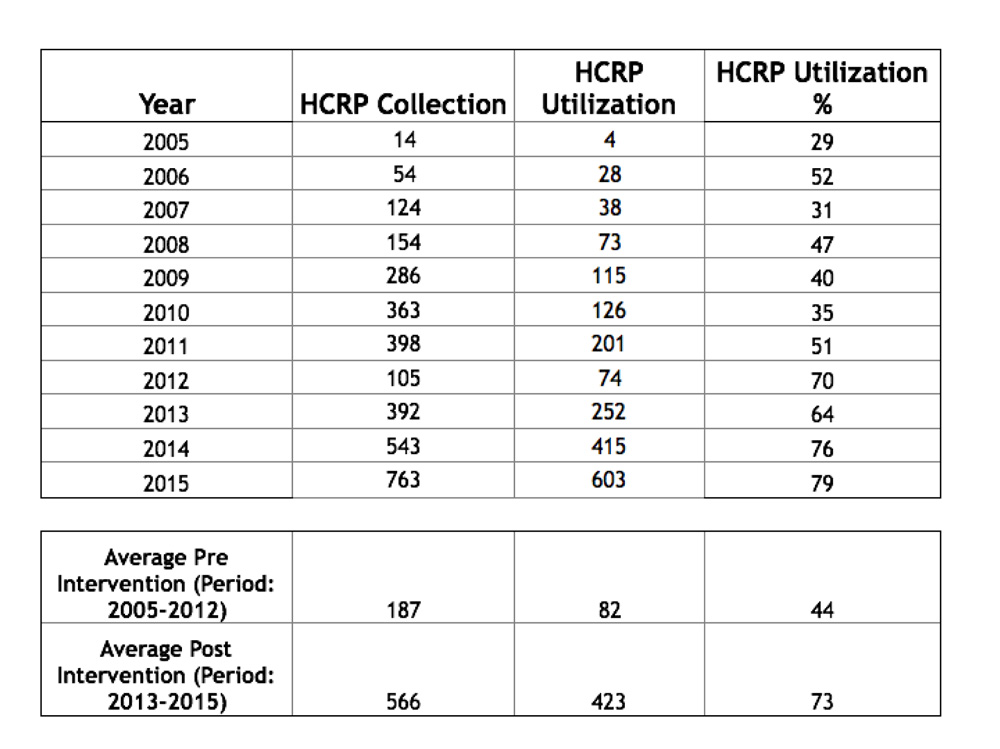
Discussion:
1.5million people in India are needlessly blind due to corneal disease. Corneal transplantation is the best available therapeutic option that can rehabilitate these patients if adequate access to this life-changing surgery is ensured. However India as a whole is able to retrieve only about 50,000donor corneas every year, of which only around 50% are usable for corneal transplants. This is not enough to meet the annual incidence of corneal related blindness, let alone tackle backlog of demand.
A study from USA by Emile Fargeet al in 1989 had revealed that the new medical standards were made and implemented in the eye banks . The eye banks were visited and compliance was checked. These efforts made a huge impact on corneal tissue collection. Data showed that in 1980 there were around 25000 corneal tissues retrieved and with all efforts number reached up to 80000 corneal tissues in year 1987.This trend is very much similar to our study wherein with improvement in quality standards, training and monitoring there was an increasing trend of corneal collection .
Eye bank association of America in another study have revealed that with proper monitoring and quality improvement there was increase in numbers of corneal transplant. Data showed that in 1997 total corneal transplant done were 11,226 which increased to 45,765 in 1999. Our study also has similar trend of increase in number of corneal transplants with QA programme.
The paucity in availability of transplantable tissues makes it relevant to increase the utilisation of collected tissues as each tissue counts. It is also important to make a qualitative shift in order to standardize eye bank activities. This study reveals the pivotal role of continuous quality improvement by QA programme in effective eye banking . This will lead to increased availability of corneal tissues for transplantation thereby contributing towards elimination of corneal blindness .
Conclusion:
The continuous quality improvement initiatives have improved the utilisation rate and quality of tissues for transplantation surgery which is a major step towards patient safety and increase patient satisfaction . This novel methodology can be replicated in other eye banks to increase the number of good quality corneal tissues for transplantation making an impact in eliminating corneal blindness.
REFERENCES
- The Past Twenty-five Years in Eye Banking Wing Chu, M.D. Cornea 19(5): 754–765, 2000.
- Eye Banking: 1944 to the Present. EMILE J. FARGE, Survey of ophthalmology volume 33. Number 4. January-February 1989
- EBAA Statistical Reports, 1990 and 1998. Washington, DC: EBAA,19
- What is Eye Banking? RaoIndianJOphthalmol1996;
44:12 - RealisticTargets andStrategiesin Eye SainiJS.IndianJOphthalmol1997;45:1412
- NPCB Guidelines for eye banking :2012
- NPCB Guidelines for eye banking :Amendments 201
- Differences in the procurement of organs and tissues by health careprofessionals. Siminoff LA, Arnold R, Miller DS ;Clin Transplant 1994, 8: 460-465