Dr. Shraddha Pandey.S19417, Dr. Sujit Abhaykumar Deshmukh, Dr. KiranSingh, Dr.Shrikant
Introduction
Diabetes is fast gaining the status of a potential epidemic in India with more than 62 million diabetic individuals currently diagnosed with the disease.
Diabetic retinopathy is one of the most severe complications that can cause blindness in patients. Blindness in diabetic patients is 25 times higher than non-diabetics.These complications could be due to the cellular metabolism leading to hyperglycemia and to the production of free radicals which combined with vital molecules result in various diseases.
The human glutathione S-transferases (GSTs) are a family of enzymes known to act in the body as the defense systems to neutralize free radicals. They play an important role in the detoxification of electrophiles by glutathione conjugation.
Several GST polymorphisms have been associated with an increased or decreased susceptibility to several diseases. Two of the important members of the GST family, named glutathione-S-transferase mu 1 (GSTM1) and glutathione-s-transferase theta 1 (GSTT1) have polymorphic homozygous deletion or null genotypes. Persons with homozygous deletions of either the GSTM1 or the GSTT1 locus have no enzymatic functional activity of the respective enzyme
The GSTM1 locus has been mapped on chromosome 1p13.3, while the GSTT1 locus exists on chromosome 22q11.2.
Various studies have showed that an increased risk of DR was associated with the null polymorphism of GSTT1 and GSTM1 respectively.
The present work aimed to study the genetic polymorphisms of the GSTM1 and GSTT1 gene as risk factor of development of diabetic retinopathy and macular edema in T2DM in order to add to the existing knowledge of the genetic basis of the disease in the North Indian population.
Material And Method
This study was done at Department of Ophthalmology, Sir Sunder Lal Hospital, BHU and Department of Molecular and Human Genetics, BHU between August 2013 and July 2015.
It was a case-control study.
Total no. of cases were 100
Total no. of controls were 200 (T2DM =100, Non Diabetic =100)
- Inclusion criteria
Clinical evidence of diabetic retinopathy with clinically significant macular edema, as defined by the Early Treatment Diabetic Retinopathy Study, and OCT retinal thickness of at least of 250 μm in the central subfield. Patients able to cooperate with the protocol
- Exclusion Criteria
Patients having other ocular disease like hypertensive retinopathy, CRVO, BRVO etc.
Patients with any other ocular disorders like uveitis , glaucoma etc.
Unwilling patients
Patients with peripheral arterial disease will be excluded from the study, also those with a history of filariasis, HIV and hepatitis B virus infection, or chronic renal failure.
DNA was extracted from peripheral white blood cells by a salting out method. The DNA purity and concentration will be determined by spectrophotometer measurement of absorbance at 260 and 280 nm. The GSTM1 and GSTT1 genotypes was identified by polymerase chain reaction (PCR) of blood DNA samples using positive/null allele approach. Analysis of data was done by using Chi-square test and ANNOVA using Graph Pad prism for association study and sensitivity calculations.
All patients underwent refraction, and BCVA was measured using the snellen visual acuity chart. In addition to other routine ophthalmic examinations, spectral-domain OCT (Cirrus HD-OCT, Carl Zeiss Meditec, Dublin, CA) was performed in all eyes with a 6-mm line scan, which comprises 1,024 axial scans, through the central fovea in both the horizontal and vertical directions.
We also obtained images using the currently available Cirrus-OCT software (Carl Zeiss Meditec, Dublin, CA) for a macular cube of 512×128, in which a 6×6-mm area of the macula is scanned with 128 horizontal lines, each consisting of 512 A-scans per line.
We defined the central subfield thickness (CST) as the average retinal thickness of the 1-mm central scanned area and cystic changes as intraretinal cystoid spaces in the fovea (1.8 mm in diameter).
The data were expressed as mean with considering standard error of mean as error bars. Statistical significance (P < 0.05) was determined with Student’s t test (two-tailed) and / or nonparametric ANOVA followed by Bonferroni’s multiple comparison test. Statistical analysis of data was performed using Graph Pad Prism
Genotype characteristics of DR cases and controls for GSTM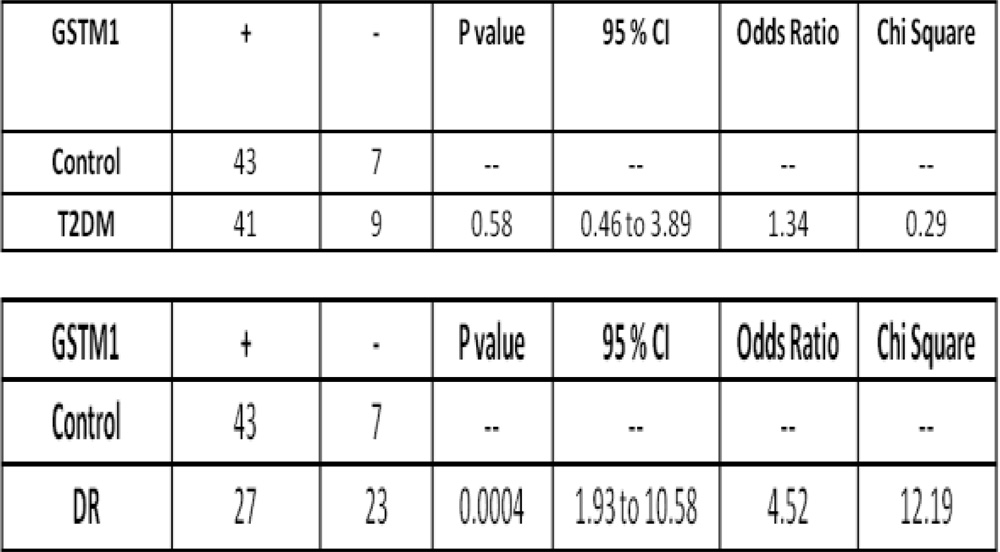
1Representative gel electrophoresis picture showing different genotypic polymorphism of GSTM1 gene :
- PCR products analyzed on 2% agarose gel. The presence or absence (null) of GSTM1 was detected by the presence or absence of a band at 230bp (corresponding to GSTM1).
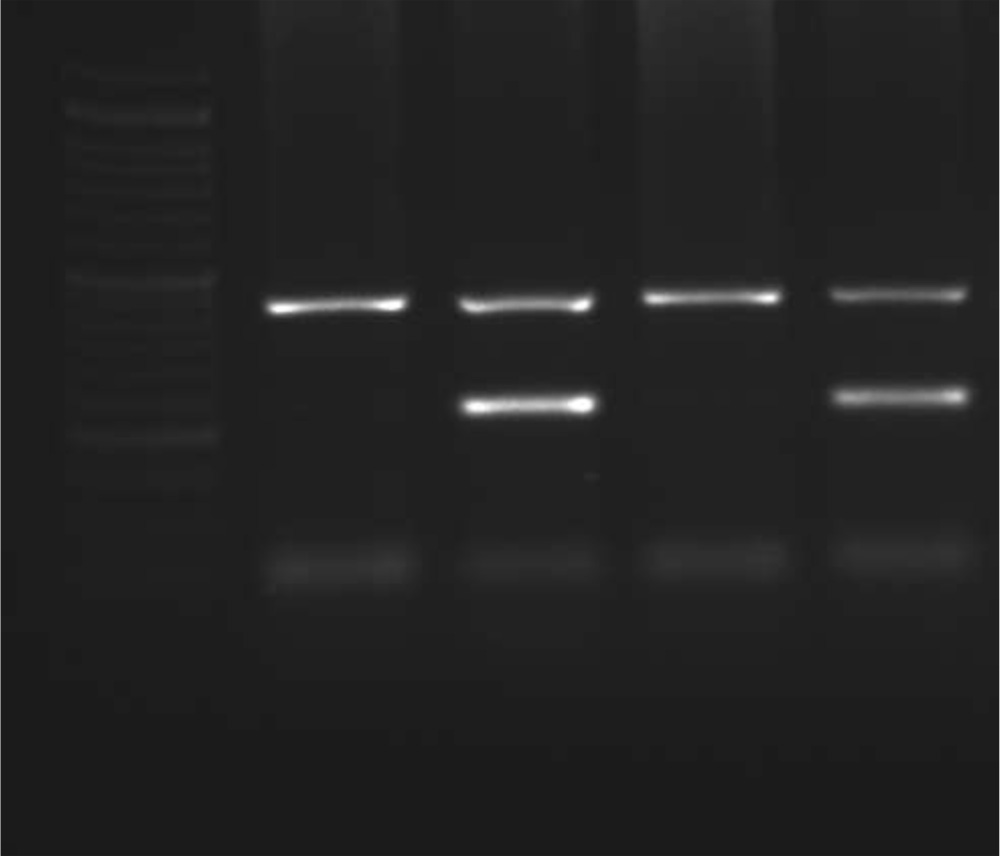
Above gel picture shows
- Lane 2,4= PRESENT
- Lane 1,3= NULL
- Table showing genotype characteristics of DR cases and controls for GSTT
| GSTT 1 | +
(present) |
—
(null) |
p value | Odds Ratio | 95% CI | Chi square |
| CONTROL | 49 | 2 | __ | __ | __ | __ |
| DR | 45 | 6 | 0.14 | 2.92 | 0.7 to 12.31 | 2.17 |
| GSTT 1 | +
(present) |
—
(null) |
p value | Odds Ratio | 95% CI | Chi square |
| T2DM | 45 | 5 | __ | __ | __ | __ |
| DR | 45 | 6 | 0.77 | 1.19 | 0.34 to 4.16 | 0.081 |
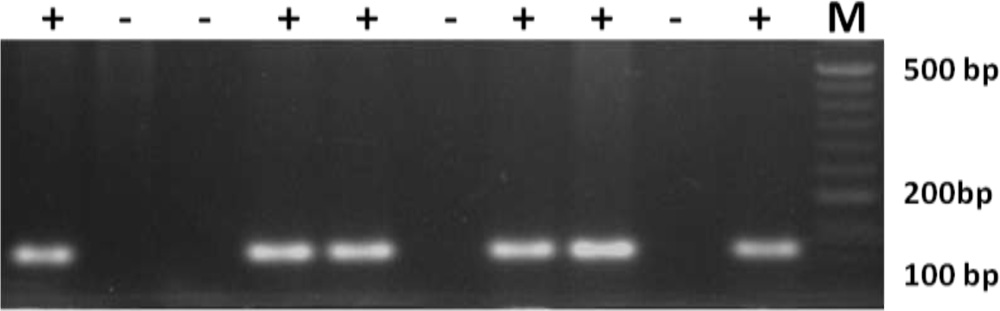
PCR products analyzed on 2% agarose gel. The presence or absence (null) of GSTT1 was detected by the presence or absence of a band at 112bp (corresponding to GSTT1)
Above gel picture shows
Lane 1,4,5,7,8,10 = PRESENT
Lane 2,3,6,9 = NULL
Discussion
Work related to genetic association of diabetic retinopathy in our department
1.Association between -1306C/Tan -1562 C/T polymorphism of MMP-2 and MMP-9 and risk of proliferative diabetic retinopathy.
Dr. Shri kant ,Dr.Kiran SinghDr.PrabhjotGoyal,Dr.Kanhaiya Singh ,Dr. N K Agrawal,.
2.VEGF C(-7)T single nucleotide polymorphism as genetic risk factor for diabetic retinopathy and its correlation to OCT.
Dr. Shri kant ,Dr.Kiran Singh Dr.Manjusingh ,Dr.Kanhaiya Singh,Dr. N.K. Agrawal .
3.Toll-like receptor 4 polymorphisms and their haplotypes modulate the risk of developing diabetic retinopathy in type 2 diabetes patients.
Singh K, Kant S, Singh VK, Agrawal NK, Gupta SK, Singh K.
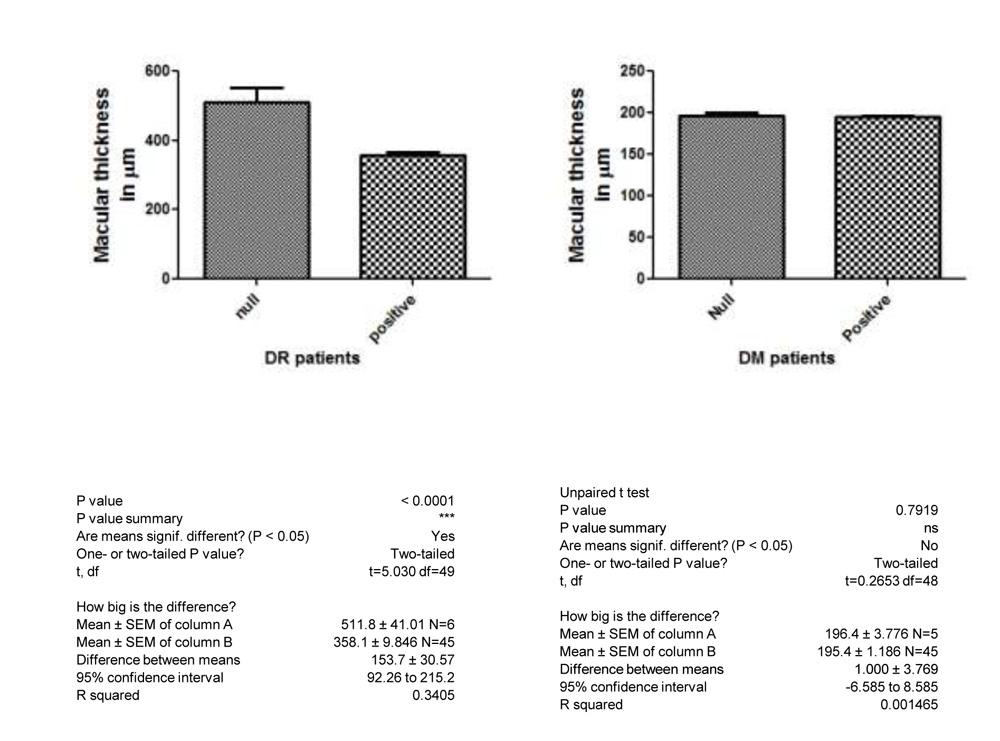
Central Subfoveal Thickness was not dependent on GSTM1 genotype and it was found that GSTM1 NULL genotypes were having statistically insignificant difference in Central Subfoveal Thickness.
Poor glycemic control increased the risk of progression of diabetic retinopathy.
Presence of GSTM1 polymorphism was a significant genetic risk factor for diabetic retinopathy in North Indian population ( Increased the risk 5 fold).
Thus close monitoring of GSTM1 Null genotype T2DM patients should be done for development of diabetic retinopathy as they are more predisposed for it. This finding will also help us in defining the treatment plan and prognosis in this group.
GSTM1 NULL genotype prevalence was more in DR cases than in Controls ( 46% vs 14%).
Statistical analysis revealed that this difference in prevalence of GSTM1 NULL genotype increases the risk of developing DR by about 5 fold (OD 4.52 ,95%CI 1.93 to 10.58).
GSTM1 NULL genotype prevalence was similar in T2DM cases and healthy Controls (18% vs 14%).
Statistical analysis revealed that this difference in prevalence of GSTM1 NULL genotype did not increases the risk of developing T2DM ( p=0.58, OD =1.34,95%CI 0.46 to 3.89)
These results need to be replicated in a larger sample size and for further substantiation of these results should be reconfirmed through studies in different cohorts.
- The results presented herein showed higher GSTT1 polymorphisms in DR case group and T2DM patients compared to healthy controls.
- Statistical analysis of results showed that genetic factors play role in DR as family history was present in 46 % cases.
- GSTT1 NULL genotype prevalence is more in DR cases than in Controls ( 13.88%vs 4.02% ).
- Statistical analysis reveals that this difference in prevalence of GSTT1 NULL genotype increases the risk of developing DR by about 3 fold ( Odds ratio of 2.92 ,95%CI 0.7 to 12.31).
- GSTT1 NULL genotype prevalence is nearby similar in DR cases and T2DM ( 13.88%vs 11.11% )( OD – 1.19 ,95%CI 0.34 to 4.16)
- GSTT1 NULL genotype prevalence is more in T2DM cases than in Controls ( 11.11%vs 4.02% )
- Statistical analysis reveals that this difference in prevalence of GSTT1 NULL genotype increases the risk of developing T2DM by about 5 fold ( OD – 2.54 ,95%CI 0.5 to 11.71)
- GSTT1 NULLgenotype prevalence is more in DM cases (DR cases + T2DM) than in Controls ( 12.22%vs 4.02% )
- Statistical analysis reveals that this difference in prevalence of GSTT1 NULL genotype increases the risk of developing T2DM and DR by about 5 fold ( OD – 2.42 ,95%CI 0.7 to 8.04)
- We also studied the relationship between Central Macular Thickness and NULL GSTT1 genotype, in which we observed that the genotype characteristics of DR vs macular edema, GSTT1 NULL genotype is more prevalent in DR group with macular edema compared to that without macular edema.
- Central Macular Thickness was dependent on GSTT1 genotype and it was found that GSTT1 NULL genotype were having statistically significant higher Central Macular Thickness in μm (511.8 +/- 41.01) compared to Positive GSTT1 genotype (358.1 +/- 9.86) and having p value < 0.001 ( 95% CI 92.26 to 215.2).
Conclusion
Presence of GSTM1 polymorphism was a significant genetic risk factor for diabetic retinopathy in North Indian population ( Increased the risk 5 fold).
- Our study suggests that the null GSTT1 genotype have an influence on the risk of having development of Diabetic Retinopathy in type 2 diabetes mellitus. ( Increased the risk 3 fold).
- Null GSTT1 genotype also have statistically significant influence on Central Macular Thickness which is seen more in NULL genotype of GSTT1 as compared to Positive GSTT1 genotype.
- Increased Central Macular Thickness has direct impact on visual acuity of patients.
- Thus close monitoring of GSTM1 Null genotype T2DM patients should be done for development of diabetic retinopathy as they are more predisposed for it. This finding will also help us in defining the treatment plan and prognosis in this group.
- These results need to be replicated in a larger sample size and for further substantiation of these results should be reconfirmed through studies in different cohorts.