Dr. Ganesh Kalyanshetti, K18010, Dr. Satyamurthy K V, Dr.Jaysheel Nazare
Author : Satyamurthy K V membership no S06137
Co author : Jaysheel Nazare
Presenting author : Ganesh Kalyanshetti membership no K18010
AIM:
To evaluate the relation between meibomian gland dysfunction (MGD)and severity of diabetic retinopathy.METHOD:A prospective ,cross-sectional ,observational study done at a tertiary eye care centre between March 2015 andFebruary2016. Eyes of 110 diabetic patients were studied. Meibography was done with SIRIUS – 3D Rotating Scheimpflug Topography System . Results: Diabetic retinopathy (DR) was classified into no DR (30%) , mild NPDR (22.72%), moderate NPDR (12.7% ), severe NPDR (7.3%) andPDR (27.27%).Meiboscore was analysed for upper and lower lid separately.On upper lid analysis meiboscore of grade 0 in 18.18% ,grade 1 in 45.45%,grade 2 in 33.63%,grade 3 in 2.72% was noted. .On lower lid analysis meiboscore of grade 0 in 54.54% ,grade 1 in 35.45%,grade 2 in 9.09%,grade 3 in 0.91% was noted. Conclusion: changes in meibomian glands were significant in diabetic retinopathy patients compared to diabetic patients with no diabetic retinopathy and probability of meibomian gland dysfunction (MGD) increases as grade of DR increases.
INTRODUCTION :
The association of dry eye disease and diabetic retinopathy has been reported previously. Although the connection between diabetes and dry eye has been proposed, the methods used for diagnosis of dry eye are different among different studies and this might bear an influence on the reported prevalence of dry eye disease in diabetes.
Corneal sensitivity measurements, Schirmer test, tear film break-up time (TBUT) analysis, cytological analysis, Rose Bengal and fluorescein staining are the most well known objective tests used for diagnosis of dry eye disease1.Dry eye disease has been found to be more prevalent in people with proliferative diabetic retinopathy (PDR) and/or clinically significant macular edema (CSME).The prevalence of dry eye disease in people with type 2 diabetes mellitus has been measured using direct measurement of tear osmolarity by a Tear Lab Osmolarity system2.
Meibography has been used to study the meibomian glands of the normal population and the age related changes noted in various studies. As far as we know, no study has been done to correlate DR and the meibography changes.
India is now the diabetic capital in the world. We hope that this study helps in better understanding of the changes in meibomian glands in Diabetics, thus adding a new dimension in the management of dry eyes in these patients.
METHODS:
This study was carried out in the Out Patient of a large Eye hospital in Southern India
Inclusion criteria:
All patients with DM with or without dry eye symptoms .
Exclusion criteria:
Any ocular surgery within the last 1 yr.
Refusal to be part of the study.
Meibography
Introduced in 2008 by Arita et al., non-contact meibography is the latest meibographic technique.
We used the Meibography system with SIRIUS – 3D Rotating Scheimpflug Topography System. The patients were explained about the procedure. The upper and lower lids were evertedand Infra Red photos were taken with the SIRIUS topographer sequentially. The procedure caused only mild discomfort to the patient and took an average of 2 minutes per patient.

GRADING :
In the meiboscore method the meibomian gland dropout is calculated a the percentage of the total.
Officially termed the ‘‘meiboscore’’ in 2008 by Arita et al.,
(1): involved lid area is <33%;
(2): involved lid area is 33–66%;
(3): involved lid area is >66%.
The percentage of loss was calculated with the help of the SIRIUS Topographer software. It is very simple to use and helps to reduce interpersonal variability and bias in the grading process. 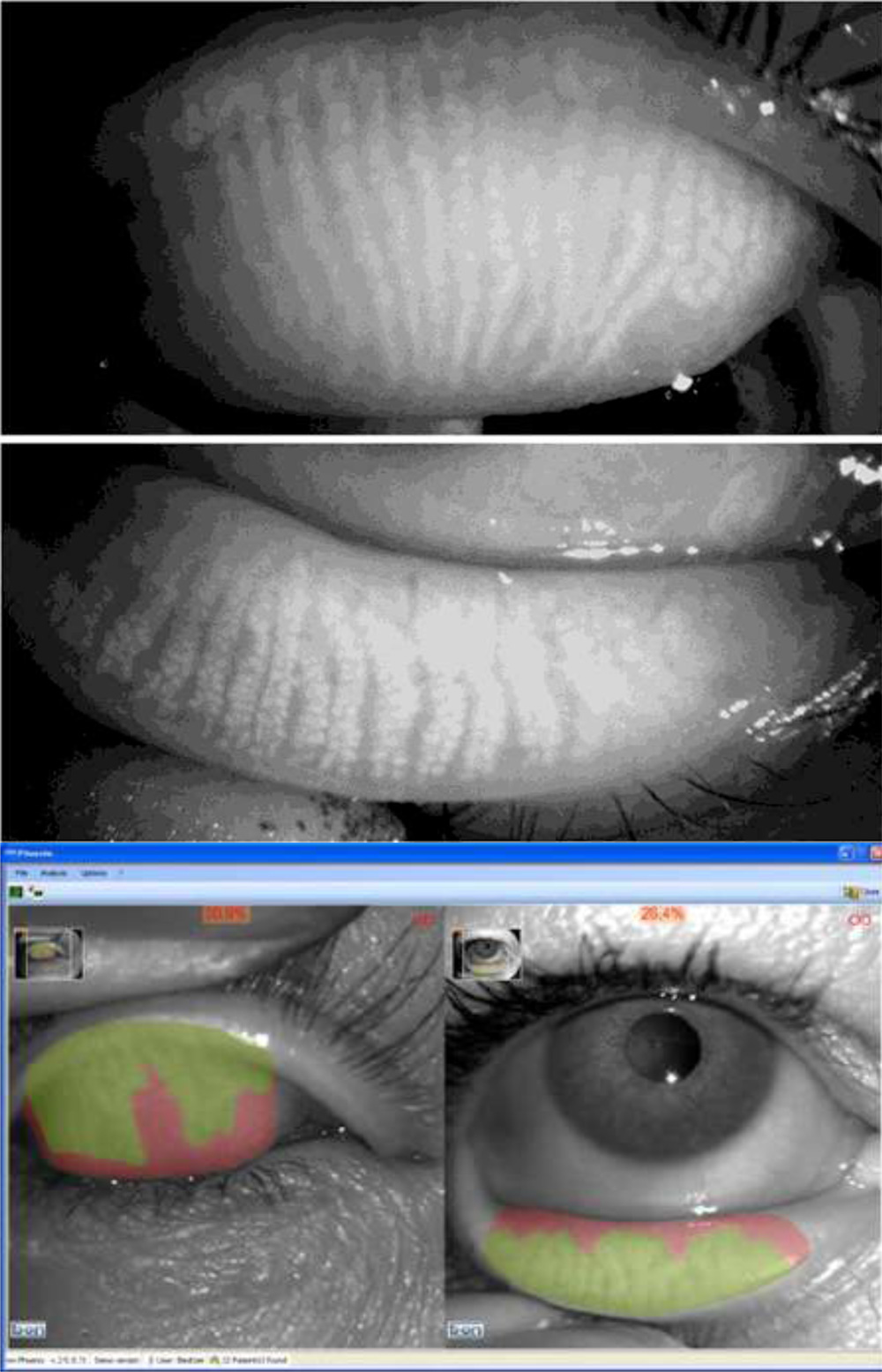
The green zone is the area with meibomian gland and the red is the dropout area. The computer gives the percentage of loss, helping us to place the eyes in one of the 3 grades.
Tear Break Up Time (TBUT), Schirmer test(ST) and staining was also done in all the patients prior to the meibography but was not taken into account in this study.
DIABETIC CLASSIFICATION:
The patients were divided into type 1 and type 2 DM.
The dry eye work up consisting of TBUT, Schirmer Test and staining wascarried outfirst, followed up by meibography.
Following the dry eye workup the patients were dilated and sent to the retina department for evaluation. The patients were divided into No DR changes, Mild Non Proliferative DR(NPDR), Moderate NPDR, Severe NPDR and PDR.
RESULTS :
Majority ofpatients in this study belonged to either the PDR group or no DR group.
It was found that out of the 27% of patients with PDR the average meiboscore grading was grade 2.
The patients with no DR changes on fundus had an average grading of grade .
The patients with mild NPDR had an average grading of grade 1.
Analysis of the moderate and severe NPDR patients could not be done as the numbers were too small to be of significance.
DISCUSSION :
Meibomian glands secrete lipids into the tear film and prevent excessive evaporation of the tear film by forming a thin oily layer on the tear film. Meibomian gland dysfunction (MGD) is a major cause of dry eye syndrome and often results in unstable tear film, damage to the ocular surface epithelium, chronic blepharitis, contact lens intolerance, and giant papillary conjunctivitis3. Despite its clinical
importance, there are no established criteria to diagnose MGD because of a large discrepancy between subjective symptoms and objective findings in patients with MGD. Existing methods for diagnosing MGD objectively include slit-lamp examination of the lid margins and ocular surface epithelium, meibometry, assessment of the volume and properties of the meibum, and meibography. Among these, meibography is the only technique that can be used to obtain information about the morphologic characteristics of
meibomian glands .
Dry eye and DM go hand in hand. Diabetes mellitus is a common systemic disease characterized by chronic hyperglycemia which leads to major chronic complications such as peripheral neuropathy, nephropathyandretinopathy .
Dry eye disease (DED) is a common ocular disease among the adult population .Diabetic patients may exhibit dry eye symptoms due to several reasons such as neuropathy, metabolic dysfunction and/or abnormal lacrimal secretions. It has been shown that the composition of tear proteins in diabetic is different from healthy subjects . Damage to the microvasculature of the lacrimal gland accompanied with autonomic neuropathy might impair lacrimation in long standing diabetes mellitus4. Patients with diabetic retinopathy do not complain of dry eye symptoms, however, they have clinical and pathological manifestations of KeratoconjunctivitisSicca (KCS). Several previous studies have investigated the relationship between dry eye disease, diabetes, and diabetic retinopathy. However, the prevalence of DED varied according to the methods used for diagnosis of dry eye and it was not clear whether there is a correlation between DED and other microvascular complications of diabetes5.
In a study of Tear production and corneal sensitivity in diabetes by Pippa Cousen, Peter Cackett6 published in 2007 Journal of Diabetes and its Complications the diabetic patients demonstrated a significantly reduced Schirmer’s test result (P<.001) and significantly reduced corneal sensitivity (P<.01)
A study done by Masoud Rezain7 2008 showed that patients with diabetic retinopathy were found to be more prone to develop dry eye disease, especially those with PDR and CSME.
M Ozdemir8 showed that Tear film BUT and Schirmer test values were significantly lower in diabetic patients compared with control subjects (P<0.001). In the diabetic group, significantly more subjects had abnormal fluorescein and rose bengal staining than in the control group (P<0.001).Abnormal tear function tests were associated with poorer metabolic glucose control.
Dr.Laily Najafi9 showed that the prevalence of dry eye disease in people with type 2 diabetes mellitus was 27.7%, using direct measurement of tear osmolaritybya Tear Lab Osmolarity system.
Aritaet al10 conducted a study of meibography on normal population and found that there was a positive correlation between increasing age and loss of meibomian glands.
In our study we could notice a pattern where the progression of the diabetic fundus changes correlated with the progressive loss of meibomian glands on the meibographer . Even when compared with the patients in the same age category to take onto account the loss of glands due to age .
We are not aware of any currently available medication to increase the meibomian gland population but supplements like Omega 3 Fatty Acids may help improve quality of meibum and prevent further loss.
Conclusion
Progression of Diabetic Changes onfundoscopy may signal a concurrent loss of meibomian glands and contribute to the patients visual disturbance.
Thus ophthalmologists should take a holistic view by also addressing the issue of evaporative dry eye in these patients.
Drawbacks of the study:
This being a case series observational study more subjects will be required in each group to make positive correlations .
Loss of glands due to age or dry eye due to other factors should be taken into account.
As this is an ongoing study appropriate correlations and comparisons will be available in the near future as more data becomes available.
REFERENCES :
1 Dogru et al., 2001;Nepp et al., 2000;Yu, Chen, Qin, Xie, & Lv, 2008;Nelson, Havener, & Cameron, 1983;Yoon, Im, & Seo, 2004;Figueroa-Ortiz, Jiménez Rodríguez, García-Ben, & García-Camposa, 2011
2 Laily Najafi, Mojtaba Malek. Journal of Diabetes and Its Complications, 2013
3 Schein OD, Munoz B, Tielsch JM, et al. Prevalence of dry eyeamong the elderly. Am J Ophthalmol 1997;124:723– 8.
4 Nichols JJ, Berntsen DA, Mitchell GL, Nichols KK. An assessmentof grading scales for meibography images. Cornea2005;24:382– 8.
5 Moss SE, Klein R, Klein BE. Prevalence of and risk factorsfor dry eye syndrome. Arch Ophthalmol 2000;118:1264–8.
6 Pippa Cousen, Peter Cackett published in 2007 Journal of Diabetes and its Complications.
7 Masoud Reza Manaviat, Maryam Rashid. BMC Ophthalmology2008.
8 M Ozdemir. Diabetes Research and Clinical Practice Volume 59, Issue 3, March 2003.
9 Laily Najafi, Mojtaba Malek. Journal of Diabetes and Its Complications, 2013
10 Arita et al _ Noncontact Meibography of Age-Related Meibomian Gland Changes