Dr. SapanaMohan, S19266, Dr. Anthrayos C V Kakkanatt, Dr.Anu F Anand, Dr. Anu Paul
ABSTRACT
BACKGROUND:
Many surgical techniques and modifications have failed to prevent recurrent pterygium. We did a prospective observational clinical study of 205 patients with primary pterygiumwho were treated with different surgical techniques. The patients were followed up for a period of 2-5 years withtheaim of studying the incidence of recurrences and complications.
RESULT:
The patients were managed with different surgical techniques and were grouped into four categories. Group 1 were patients who were managed with simple excision. Group 2patientswere treated with excision with conjunctival rotation pedicle graft. Group 3patients were treated with excision followed by conjunctivalautograft. Group 4 patients were treated with excision followed with postoperative instillation of mitomycin c drops 0.02%. Age varied from 22-58 years, average age was 34 years. Male and female distribution was kept equal in all 4 groups.Complications noted were hemorrhage, astigmatism, symblepharon, foreign body sensation andcorneoscleral ulcer. Complication rate noted in the groups were 12% in group 1, 16% in group 2, 6% in group 3 and 8% in group 4. A cosmetic blemish or regrowth of fibrovascular tissue was considered as recurrence. Recurrence rate in group 1-30%, group 2- 14%,group 3- 9% and group 4- 8%.
CONCLUSION
Patients in Group 4 who underwent pterygium excision with mitomycin c instillation post operatively had minimum recurrence and patients in group 3who hadpterygium excision with conjunctivalautograft had the least incidence of complications.
AIM OF STUDY:
To study the rate of recurrence of pterygium and complications of pterygium surgeryin patients managed with different modes of treatment for pterygium.
INTRODUCTION:
Pterygium, a triangular sheet of fibrovascular tissue that invades the cornea, is primarily a lesion of the tropical and subtropical regions. The lesion usually begins in the conjunctiva in response to damage from ultraviolet light ( UV-B 320 nm to 286nm).The histological and epidemiological characteristics of pterygium suggest thatUV. radiations play a role in pathogenesis by producing a chronic inflammatory cellular infiltration with inflammatory edema and cell-induced angiogenesis(1). The pathophysiology of pterygium is characterised by elastotic degeneration of collagen and fibrovascular proliferation with an overlying covering of epithelium(2). Regrowth after surgical removal of primary pterygium resemble the primary lesion, but the pathogenesis is different. Many surgical techniques and modifications have been used to remove pterygium but these have failed to prevent recurrence(4-11) . Excision with autograft has the advantage of placing the stem cells of limbal conjunctiva along the limbus of the required scleral bed(10). Excision with conjunctival rotation pedicle flap has the advantage of preserving the blood supplyof the graft at the cost of loss of the limbal stem cells(5).Mitomycin c is an anti-metabolite produced by Streptomyces caespitosus. It has been used as an adjunctive treatment due to its ability to inhibit fibroblasts(3-6).
MATERIALS AND METHODS:
Patients with primary pterygium with symptoms were examined in detail using slit lamp. Surgical treatment was indicated when fleshy pterygia actively grew and produced clinical symptoms. Mode of treatment studied were grouped into 4. Group 1 – simple excision. Group 2 – excision with conjunctival rotation pedicle graft. Group 3- excision with conjunctivalautograft. Group 4 – excision with postoperative instillation of mitomycin 0.02%, twice a day for 5 days. Out of 350 patients with primary pterygia treated by one of these methods 205 patients (331eyes ) were followed up for a period of 2-5 years and were selected for this study. Complication and recurrence rates were noted in follow up visits. Commonly noted complications were hemorrhage, foreign body sensation astigmatism, symblepharonandcorneo- scleral ulcer.
RESULTS:
1.AGE DISTRIBUTION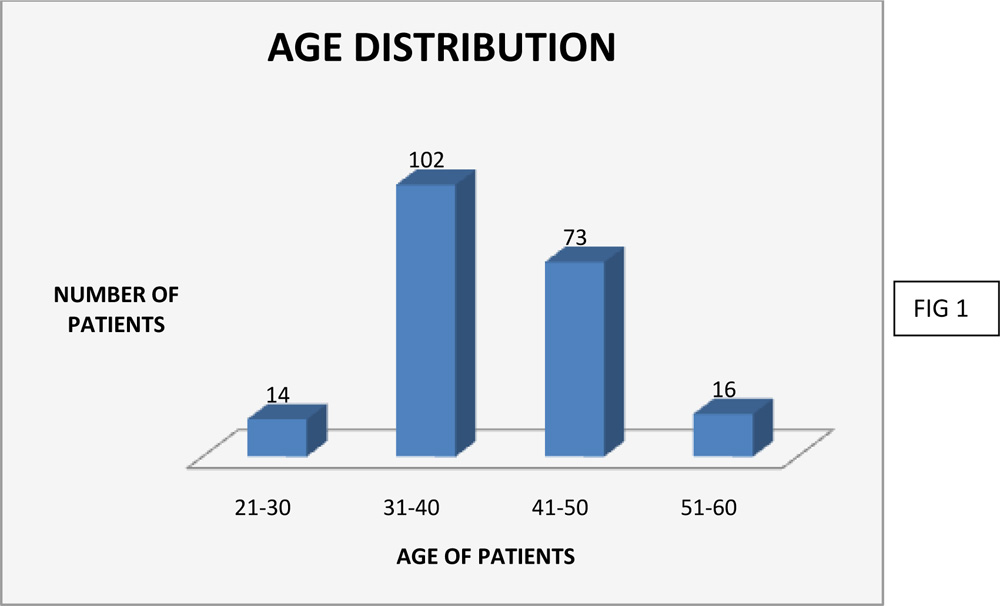
Age of patients ranged from 22 to 58years.Among the total of 205 patients included in the study, 102 were between 31-40 years, 73 were between were between 41 – 50 , 16 were aged between 51 – to 60 and 14 were aged between 21 – 30 years. Average age of patients was 34years.
2.GENDER DISTRIBUTION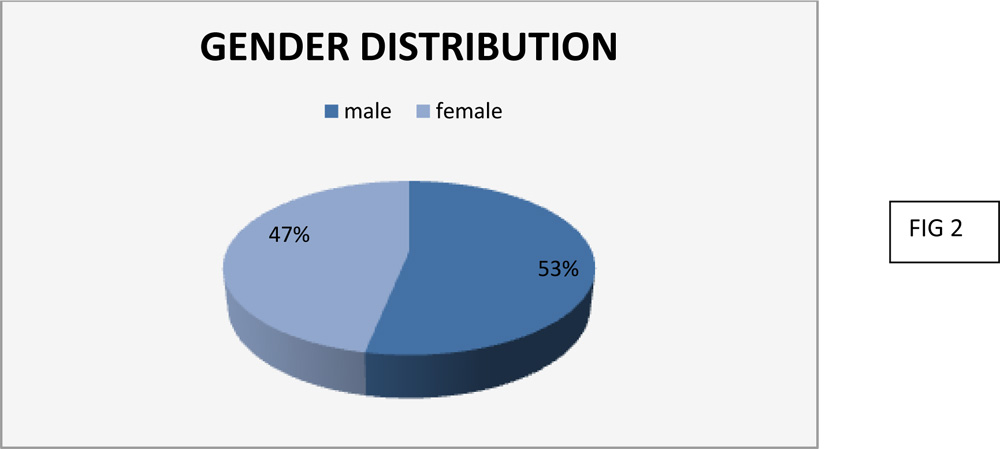
There were 109(53%) male patients and 96(47%) female patients.
3.TREATMENT GIVEN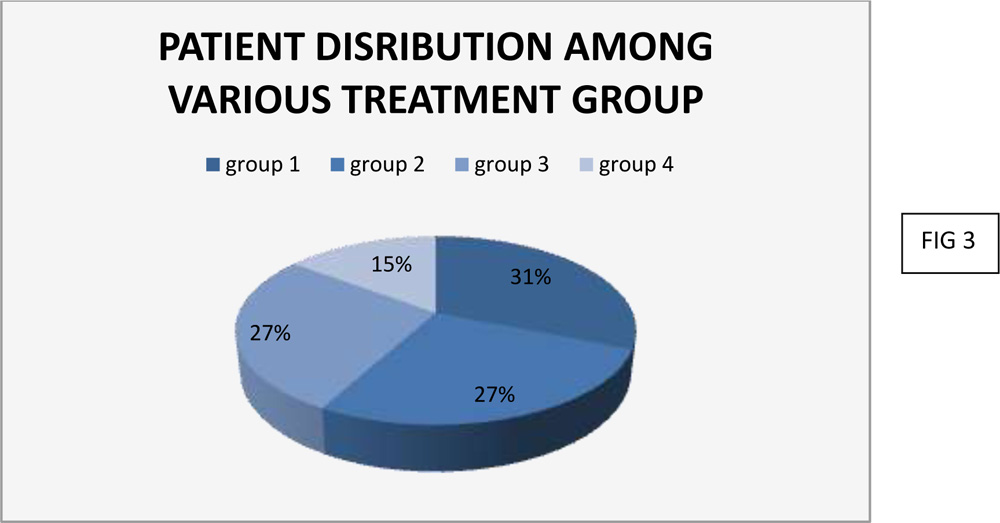
Group 1 was treated with simple excision of the pterygium. Group 2 was treated with excision of pterygium with conjunctival rotation pedicle graft. Group 3 was treated with excision of pterygium with conjunctival autografts. Group 4 was treated with pterygium excision with post operative instillation of Mitomycin C 0.02% twice a day for 5 days.
Number of eyes treated in each group
Group1 – 103
Group 2 – 89
Group 3 – 90
Group 4 – 49
4.COMPLICATION RATES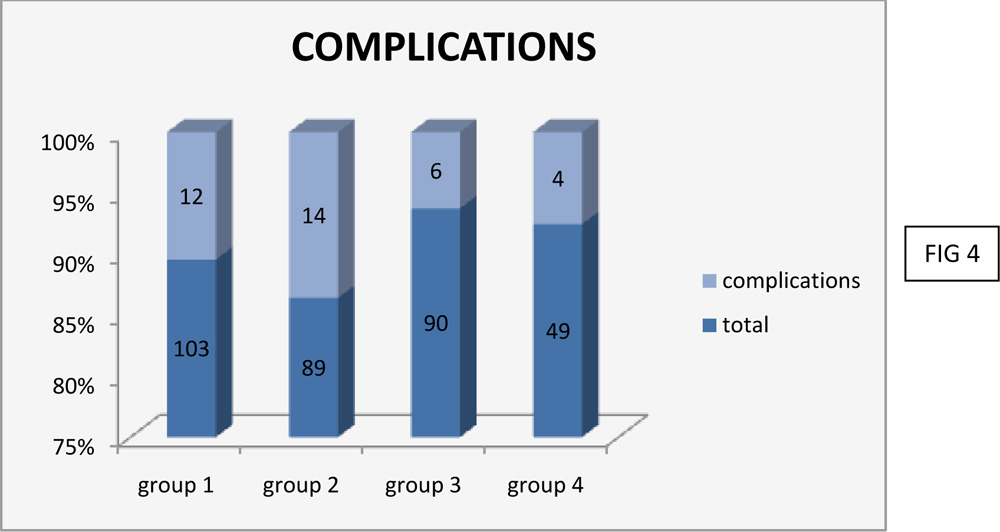
Group 1- 12 eyes had complications. Commonly noted complication were hemorrhage and symblepharon.
Group 2 – 14 eyes had complications. Complication noted were hemorrhage, foreign body sensation, chemosis and astigmatism.
Group 3 – 6 eyes had complications. Complication noted were foreign body sensation and haemorrhages
Group 4 – 4 eyes had complications. Complications noted were haemorrhages and 1 patient with a corneoscleral ulcer.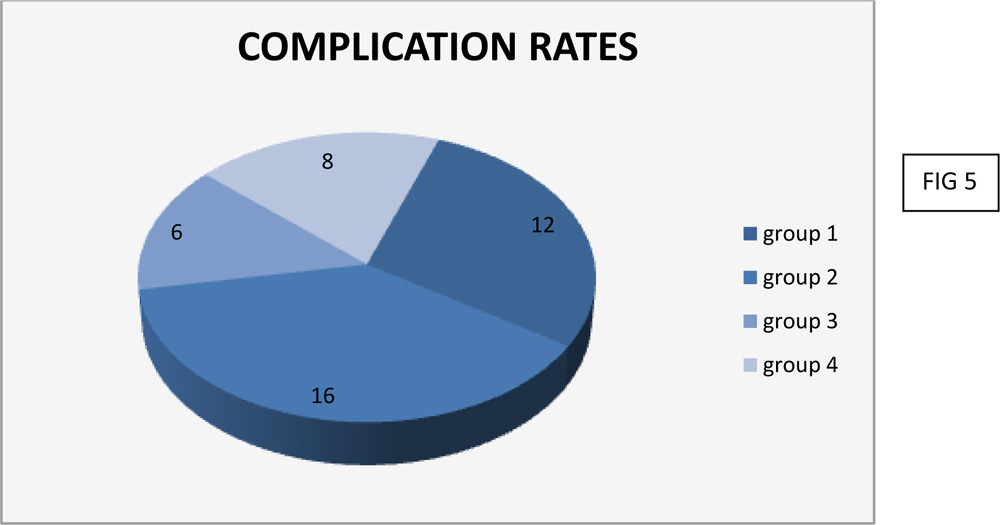
Complications rates noted in each group were :
Group 1 -12%
Group 2- 16%
Group 3- 6%
Group 4 -8%
Pterygium excision with conjunctival autograft method had the least rate of complications
5.INCIDENCE OF RECURRENCE: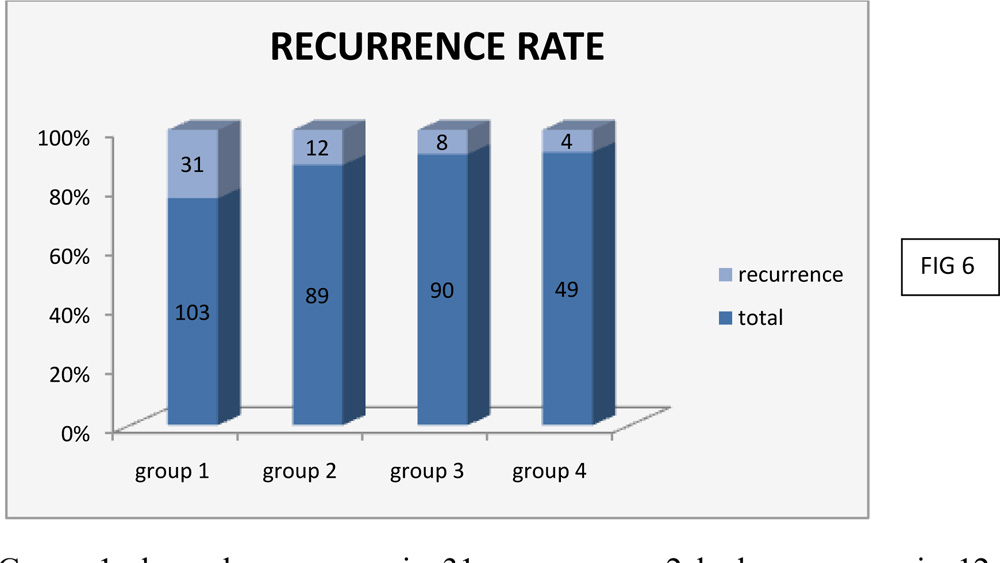
Group 1 showed recurrence in 31 eyes, group 2 had recurrence in 12 eyes, group 3 had recurrence in 8 eyes and group 4 had recurrence 4 eyes
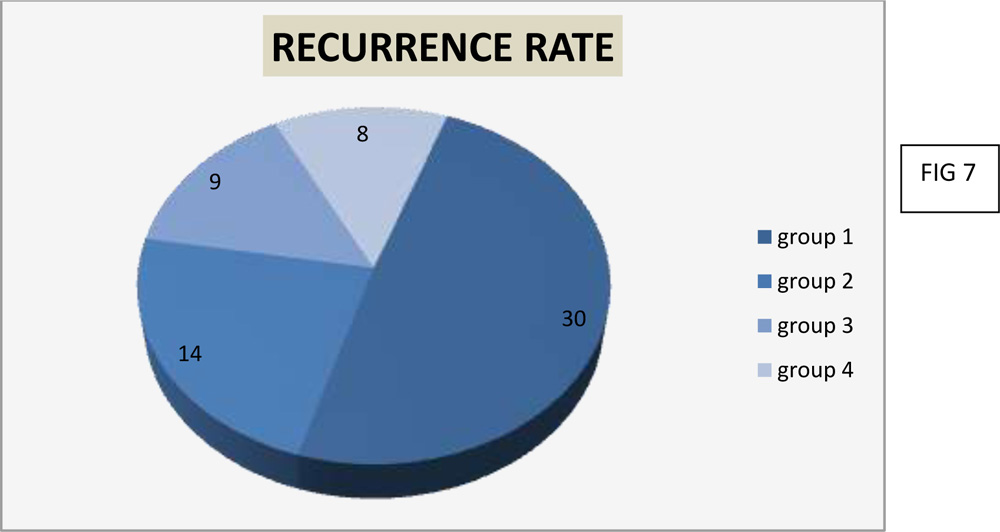
Recurrence rate noted in each group were:
Group 1 – 3o%
Group 2 – 14%
Group 3 – 9%
Group 4 – 8%
Excision with post operative instillation of Mitomycin c had the least recurrence rate of 8%.
DISCUSSION:
Out of 350 patients with primary pterygia who were treated, 205 patients were available for follow up visits. 331 eyes of 205 patients were included in the study. The patients were followed up for a period of 2-5 years. Complication and recurrence rates were noted in follow up visits.
The age distribution of patients (FIG 1) was between 22 and 58 with maximum patients falling between 31 to 40 years. Average age of patients was 34 years. There were 109 male patients and 96 female patients included in our study with a total of 331 eyes(FIG2).
103 patients were treated in group 1, 89 patients in group 2, 90 patients in group 3 and 49 patients in group 4(FIG 3).
Complications noted were hemorrhage, astigmatism, symblepharon andcorneoscleral ulcer. Complication rate (FIG 4 & 5) noted in the groups were 12% in group 1, 16% in group 2, 6% in group 3 and 8% in group 4. Group 3 with conjunctivalautograft had the least incidence of complications.
A cosmetic blemish or regrowth of fibrovascular tissue was considered as recurrence. Recurrence rate (FIG 6 & 7) in group 1was30%, group 2- 14%,group 3- 9% and group 4- 8%. Group 4 pterygium excision with mitomycin c instillation post operatively had minimum recurrence. Study by Bazzazi et al, aimed at comparing the results of the conjunctivalautografttechnique and Minimally Invasive Pterygium Surgery in primary pterygium, showed a recurrence rate of 11 % in the patients treated withconjunctivalautograft(12).Kareem A A et al in his study on intraoperative instillation of MitomycinC after excision of pterygumalso shows a similar recurrence rate of 8% with minimal complications(13).Both studies suggest no major complications with either treatment modalities of pterygium excision withconjunctivalautografts or intraoperative instillation of mitomycin c.
CONCLUSION:
Post operative instillation of mitomycin c in low dose and frequency is effective and safe for the treatment of pterygium. Recurrence of pterygium commonly occurs within six months after surgery, but it can appear even 20 years after surgery. So we have to follow up the cases treated up to 20 years to give a final opinion.
REFERENCES:
- Anduze A. Pterygium. A Practical Guide to Management. New Delhi: Japee; 2009.
- Garg Atoukhy E. Surgical and Medical Management of Pterygium. New Delhi: Jaypee; 2009:8-9
- Anduze AL.Pterygium surgery with mitomycin –c:ten year results. . Ophthalmic surg Lasers. 2001;32(4):341-5
- Jain AK, Bansal R,Sukhija J. Human amniotic membrane transplantation with fibrin glue management of primary pterygia: a new tuck in technique. Cornea. Jan 2008;27(1):94-9
- Jiang J, Yang Y,Zhang M, Fu X, Bao X, Yao K. Comparison of fibrin sealant and sutures for conjunctival autograft fixation in pterygium surgery: one year follow up. Ophthtalmologica.2008;222(2):105-11
- Garg Atoukhy E. Surgical and Medical Management of Pterygium. NEW DELHI: JAYPEE; 2009
- Rocha, G.U.I.L.L.E.R.M.O., 2003. Surgical management of pterygium.Tech Ophthalmol, 1, pp.22-8.
- Marcovich, A.L., Bahar, I., Srinivasan, S. and Slomovic, A.R., 2010. Surgical management of pterygium.International ophthalmology clinics, 50(3), pp.47-61.
- Janson, B.J. and Sikder, S., 2014. Surgical management of pterygium.The ocular surface, 12(2), pp.112-119.
- Riordan-Eva, P., Kielhorn, I., Ficker, L.A., Steele, A.M. and Kirkness, C.M., 1993. Conjunctival autografting in the surgical management of pterygium.EYE-LONDON-OPHTHALMOLOGICAL SOCIETY OF THE UNITED KINGDOM THEN ROYAL COLLEGE OF OPHTHALMOLOGISTS-,7, pp.634-634.
- Assia, E., 2002. Surgical management of pterygium.IMAJ-RAMAT GAN-,4(12), pp.1138-1138.
- Bazzazi N,Ramezani A,Rabiee M.A.S. A comparative study of conjunctival autograft and minimally invasive pterygium surgery in primary pterygia. Pakistan Journal of Biologic Science.2010;13/8:409-412.
- Kareem A.A,Farhood Q.K., Alhammami H.A. Use of antimetabolites as adjunctive therapy in surgical treatment of pterygium. Clinical Ophthalmology. 2012;6/1(1849-1854).07 Nov 2012