Dr. Shanthi Priya, K16908, Dr. Manju R Pillai, Dr. Vivek P S, Dr. Avika Kanathia
Shanthipriya K, Manju R Pillai, Vivek P S
INTRODUCTION
Glaucoma is the leading cause of irreversible blindness worldwide, and the second most common cause of blindness after cataract1,2. It isresponsible for 14% of global blindness3. Treatment options include medications, laser procedures and surgical procedures to lower IOP. Trabeculectomy was originally described by Cairns in 19684 and later modified by Watson 5 and is the most commonly performed incisional surgical procedure for glaucoma. Post operative scarring at the site of the filtering bleb has limited the success of glaucoma filtering surgeries6. The use of anti-fibrotic agents in conjunction with trabeculectomy surgeries have improved the success rates by inhibiting the fibroblastic activity and modulating the wound healing process7,8,9. Owing to the toxic effects and complications of anti-fibrotic agents, the exposure time, the dose and the surface area of application has been evaluated in several studies.The use of Mitomycin C (MMC) for enhancing the outcomes of glaucoma filtration surgery was originally described by Chenin 1983, and has most commonly been administered with sponges placed under tenons and conjunctiva 7.Subconjunctival injection of MMC is a newer method of application used in trabeculectomy surgeries.7,8,9
AIMS-
To compare the outcomes of two methods of MMC application; subconjunctival injection and subconjunctival sponge method, in patients undergoing two site phacotrabeculectomy (trabeculectomy combined with phacoemulsification and PCIOL implantation) by measuring visual acuity, intraocular pressure, number of glaucoma medications required in the postoperative period and rate of complications between the two treatment groups
MATERIALS AND METHODS-
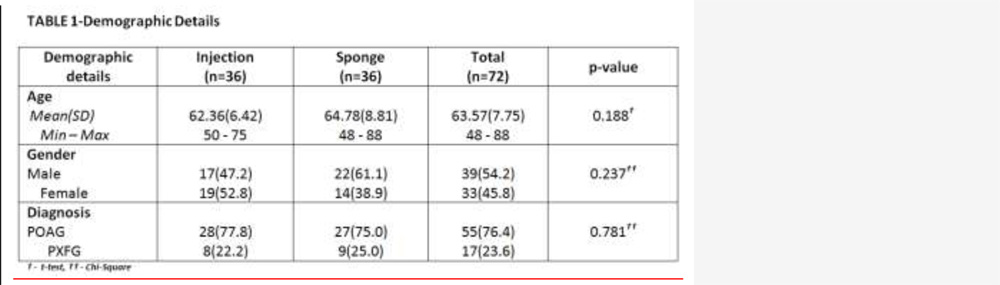
A prospective randomized clinical trial at the Glaucoma Department in tertiary eye care centre, in South India between December 2014 and November 2015.72 patients with primary open angle glaucoma (POAG) orpseudoexfoliation glaucoma(PXFG) with open angles, aged above 40 years, not controlled medically with visually significant cataract, who were willing to provide informed consent and able to comply with the study procedures, were included in the study and randomized to undergo phacotrabeculectomywith MMC injection or phacotrabeculectomy with MMC sponges (36 patients in each group).All other types of glaucoma were excluded. Patients with a history of any priorintraocular surgerieswere also excluded. Preoperative baseline evaluationincludedbest corrected visual acuity(Snellen chart), anterior segment slitlamp examination, fundus examination with slitlamp biomicroscopy using a 78D or 90D lens, IOP measurement using GoldmannApplanation Tonometry, gonioscopic examination with Goldmann 2 mirror or Zeiss 4 mirror gonio lens andvisual field assessment.
SURGICAL METHOD
PREPARATION OF MMC FOR INJECTION-
5ml of normal saline was added to 2mg MMC powder for a concentration of 0.4mg/ml. 0.5ml of this solution was mixed with 1.5ml of 2% lidocaine for a final concentration of 0.1mg/ml MMC. 0.1ml of this solution was used for subconjunctival injection.
PREPARATION OF MMC FOR SPONGES-
5ml of normal saline was added to 2mg of MMC powder for a concentration of 0.4mg/ml. 0.1 ml of this solution was used to soak the sponges.
All surgeries were performed under peribulbar anaesthesia using 5ml of 2% lidocaine with 1.5 IU of hyaluronidase. Following peribulbar injection a 4-0 silk suture was placed under the superior rectus muscle for traction.
METHOD OF MMC APPLICATION-
Prior to conjunctival incisions 0.1 ml MMC was injected subconjunctivally 8 to 10mm posterior to the superior limbus using a 30 gauge needle avoiding the superior rectus muscle.A muscle hook is used to spread the subconjunctival injection diffusely. A fornix based conjunctival flap was fashioned at the superior limbus and cautery applied as needed.
In the sponge application group a fornix based conjunctival flap was created superiorly,and monopolar cautery applied as needed.The MMC soaked sponges (2 poly vinyl alcohol sponges measuring 0.5mm × 0.5mm) were placed on bare sclera covered by tenons and conjunctiva. After 2minutes the sponges were removed and the area was irrigated with 20 ml BSS to wash off the residual MMC. The remainder of the surgical procedure was the same in both groups.
POST OPERATIVE CARE AND EVALUATION-
A standard post-operative regimen to the operated eye of combination topical antibiotic steroid eye drops (gatifloxacin with prednisolone)for the first 90 days (in tapering doses every 15days) andhomatropine-2%eye drops (2 times a day for 1 month) was followed. Glaucoma medications were continued in the non operated eye. Post operatively, all patients were examined on post op days 1, 15, 30, 90 and at 6 months. Releasable suture removal and laser suture lysis were considered as a part of normal post-operative care and therefore not considered as a resurgery or failure, whereas bleb revision or needling was considered as resurgery and classified as a failure. No case was lost to follow up.The primary outcome measure was intraocular pressure. Secondary outcome measures were the MMC related complication rates, final post-operative visual acuity and number of glaucoma medications required.
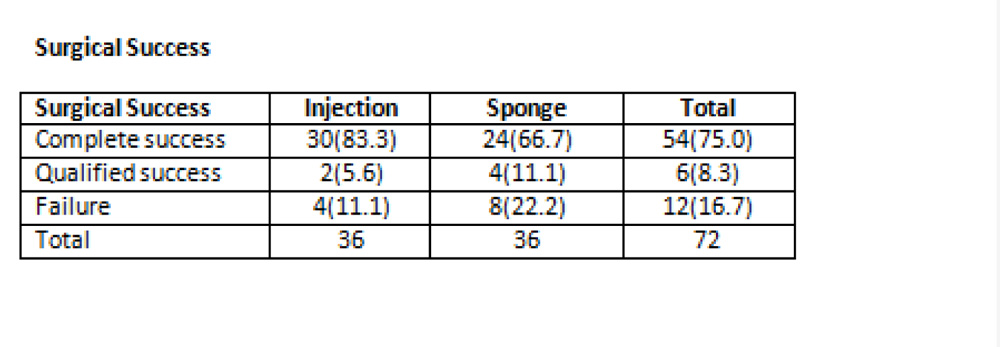
Complete success: (without medication) was defined as IOP ≤21 mmHg and >5 mmHg, without complications requiring surgical intervention or additional glaucoma surgery, and no loss of light perception.
Qualified success: (with one medication) was defined as IOP ≤ 21mmHg and > 5mmHg, without complications requiring surgical intervention or additional glaucoma surgery, and no loss of light perception.
Failure: was defined as IOP ≤21mmHg with more than one medication or IOP > 21mmHg with 2 medications, and the occurrence of any complication which required surgical intervention.
STATISTICAL METHODS-
All statistical analysis was done by STATA 11.1 (Texas, USA).
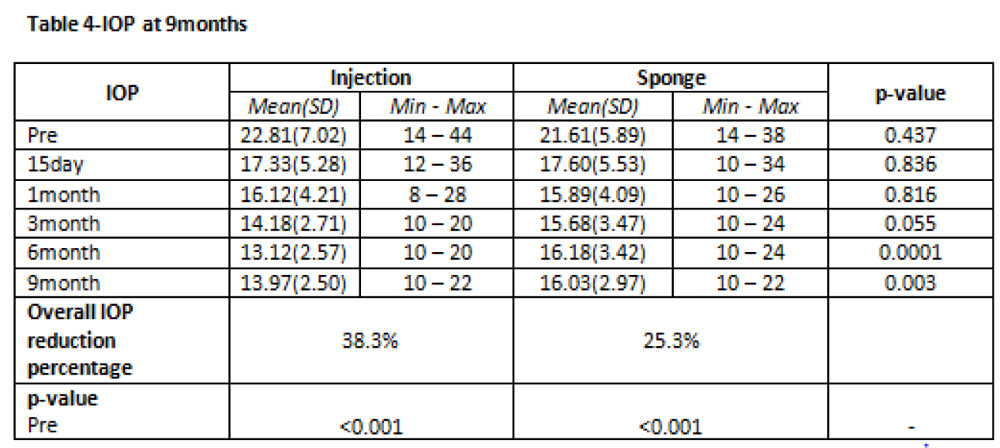
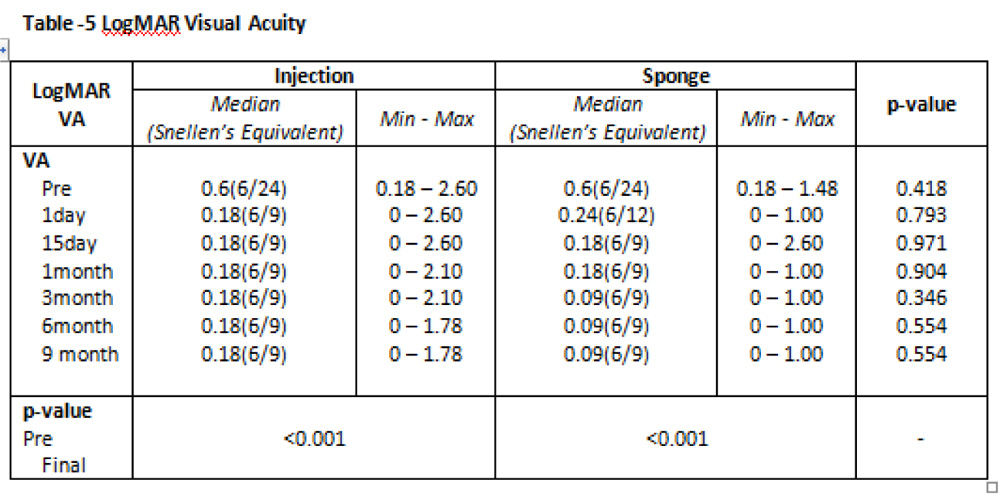
Results-The demographic characteristics were similar in both the groups. Post operatively the IOP was reduced from 22.81(±7.02) to 13.97(±2.50) (p<0.001) in injection group and 21.61(±5.89) to 16.03(±2.97) (p<0.001) in the sponge group. The difference in IOP between the two groups approached statistical significance,(p<.003) with lower IOP in the injection group. 88.9% patients in injection group achieved complete or qualified success at 6 months, and no complications in the injection group were seen . 77.8% of patients had complete or qualified success in sponge group(p<0.001).11.1% of the injection group and 30.6% of the sponge group required one or more anti glaucoma medications post operatively. Post operative vision was similar in both the groups, and improved from baseline (p<0.001). Complications included 2 cases of hyphema and a single case of endophthalmitis,all in sponge group.
CONCLUSION-Subconjunctival injection of MMC during phaco-trabeculectomy was safe and more effective than the conventional sponge application of MMC with a better control of IOP and surgical success. Longer follow up and a larger cohort is needed to further characterise the efficacy and safety of this modality.


References
1.Quigley HA, Broman AT. The number of people with glaucoma worldwide in 2010 and 2020.Br J Ophthalmol. 2006 Mar;90(3):262–7.
2.Congdon N, O’Colmain B, Klaver CCW, Klein R, Muñoz B, Friedman DS, et al. Causes and prevalence of visual impairment among adults in the United States. Arch Ophthalmol. 2004 Apr;122(4):477–85.
3.Thylefors B, Négrel AD, Pararajasegaram R, Dadzie KY. Global data on blindness. Bull World Health Organ. 1995;73(1):115–21.
4.Cairns JE. Trabeculectomy.Preliminary report of a new method.Am J Ophthalmol. 1968 Oct;66(4):673–9.
5.Watson PG. Trabeculectomy: a modified abexterno technique. Ann Ophthalmol. 1970 May;2(2):195.
6.Kitazawa Y, Suemori-Matsushita H, Yamamoto T, Kawase K. Lowdose and high-dose mitomycintrabeculectomy as an initial surgery in primary open-angle glaucoma. Ophthalmology. 1993 Nov;100(11):1624–8.
7.Chan C-W. Enhanced intraocular pressure controlling effectiveness of trabeculectomy by local application of mitomycin C. Trans Asia Pac AcadOphthalmol. 1983;9:172–7.
8.Palmer SS. Mitomycin as adjunct chemotherapy with trabeculectomy. Ophthalmology. 1991 Mar;98(3):317–21.
9.Fluorouracil Filtering Surgery Study one-year follow-up. The Fluorouracil Filtering Surgery Study Group. Am J Ophthalmol. 1989 Dec 15;108(6):625–35.