Dr. S Anand Prada, S19222, Dr. Narendra Patidar, Dr. Rahul Maheshwari
AIM:
To report AS OCT imaging results of normal lower proximal lacrimal system
METHODS:
Prospective interventional institutional study of 80 punctae of 40 asymptomatic adults. AS OCT of lower punctum and vertical canaliculus was done to record shape, content, angle of medial and lateral wall of punctum, maximal outer and inner punctal diameter and depth.
RESULTS:
Lower punctum and junction with vertical canaliculus could be imaged in all cases. Mean maximum outer punctal diameter, inner punctal diameter and depth was recorded as 700.1±424.09µ(median=584.5µ),245.5±127.54µ(median=199.5µ), 390.85±229.7µ(median=287µ) respectively with insignificant correlation between them. Angle between lateral and medial wall and inner punctum was obtuse in 60% cases.Tear film with debris was present in 10% punctate.No contents were seen in 2%. Horizontal canaliculus could not be imaged
Conclusion:
AS OCT provides non invasive normative morphological baseline assessment of lower proximal lacrimal system
No financial interests to disclose.
INTRODUCTION
Lacrimal apparatus anomalies are routinely evaluated by invasive methods as probing and syringing. A base line evaluation of the morphology of the lacrimal system and serial monitoring of changes that appear after surgical intervention guide the outcome of lacrimal surgeries. Ultrasound biomicroscopy has been used for imaging of proximal lacrimal system by Hurwitz etal, Tao et al and Tostet al.1-3 But its usefulness is limited by lack of high resolution images and a necessary contact with eyelids which is uncomfortable for some patients. OCT is a non contact and noninvasive high resolution imaging modality which depends on infrared waves to produce cross sectional images in vivo. It is routinely used for acquisition of retinal scans and anterior segment scans. Application of anterior segment OCT for evaluation of lacrimal system is limited till date.
Wawrzynski et al 4 first demonstrated the use of SD OCT in imaging of punctum and proximal canaliculus in 2014. Allam et al5described seven different morphological punctal shapes in Egyptian subjects. Variability in methodology, OCT machines and interpretation of inner punctal diameter as opposed to vertical canalicular end have provided conflicting results towards establishment of a morphological database. The present study reports SD ASOCT imaging results of lower proximal lacrimal system in central Indian subjects using RTveu system.
METHODS
This prospective cross sectional interventional study was carried out from a period of December 2015 to April 2016 at a tertiary care center in Central India. It included 40 asymptomatic healthy adults with no complaints of epiphora. ( Munk score 0, Munk et al6) . Informed consent was obtained from all subjects. Data was collected regarding the age and gender of subjects.
A detailed slit lamp examination was done to assess the postion of lid margin and puncta in relation to the globe, lid laxity using snap back and lid distraction test, visibility of puncta, ocular surface health using tear film break up time and corneal fluorescein staining test.
Patients with invisible puncta, history of chronic use of antiglaucoma medications, presence of lid margin and punctual anamolies as entropion, ectropion, masses over lid or puncta, positive regurgitation, dry eye with TBUT < 5s, history of ocular or lacrimal surgeries and trauma were excluded from the study.
SD ASOCT imaging of lower proximal lacrimal system was done for all subjects by a single physician. RTVue model-RT100 CAM system (OptovueInc) was used. Cornea/anterior segment module lens (CAM-S) add on lenswas additionly attached. A wavelength of 840± 10 nm was used for scanning. Images were acquired at a 12mm working distance.
Subjects were positioned at the ASOCT machine and lower lid was gently everted to align the punctum against the light source . Additional illumination was provided by two external cables with red LED lights. A cross line scan was chosen for imaging and 6mm×6mm cross lines were positioned at the punctum.(Fig 1). Three sequential images were taken and the image with maximum extent and depth of visible punctum and vertical canaliculus was selected for measurements.
Punctalshape , contents, angulation of the medial and lateral wall was noted.Measurement of outer and inner punctal diameter and depth was done using adjustable distance measurement tool. A tangent drawn over the punctal opening towards lid margin was used to measure outer punctal diameter. Inner punctal diameter was measured with the help of a line drawn above the abrupt narrowing of inner lumen. A perpendicular was drawn from outer punctal diameter towards the base till the inner punctal diameter to measure the depth of the punctum.(Fig 2)
Data analysis was done using SPSS v 16 software for windows. (SPSS Inc. Chicago, IL, USA)
Frequency and descriptive statistics was used for data analysis. Categorical data were described in percentages while numerical data were described in terms of mean ± SD.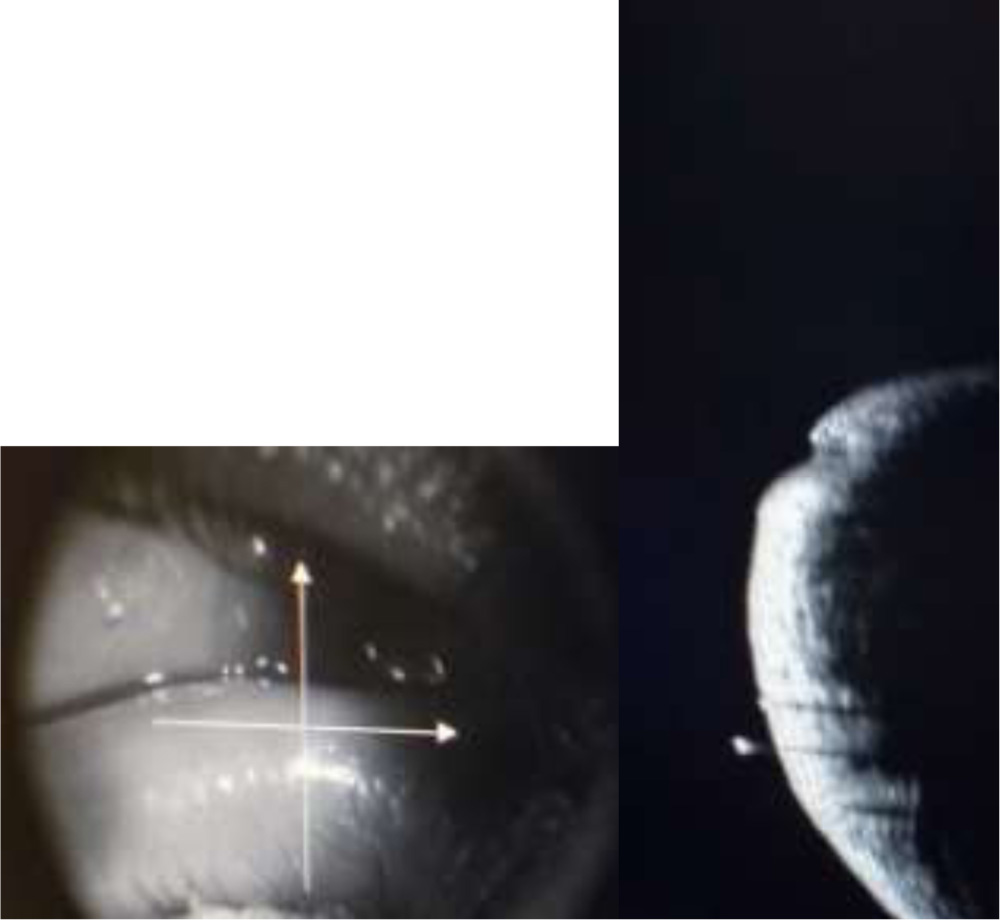

Fig 1. Horizontal and vetical cross lines centered on the punctum. Horizontal cross line measures the width of the punctum while vertical cross line measures the depth of the punctum.
RESULTS
The study included 80 puncta of 40 asymptomatic adults out of which 28 were males and 12 were females. Mean age ± SD was 38.9 ±12.81 years. (median =37.5years).Lower puncta and its junction with vertical canaliculus could be imaged in all cases using SD ASOCT. Three consecutive tissue layers could be identified. Outermost layer was identified as the epithelium. The second layer was hyperreflective compared to the first layer with as smooth interface in between. This layer corresponded to fibrous tissue layer. The third layer was hyporeflective compared to the second layer with an irregular interface in between. This layer corresponded to muscle of Riolan (Fig2)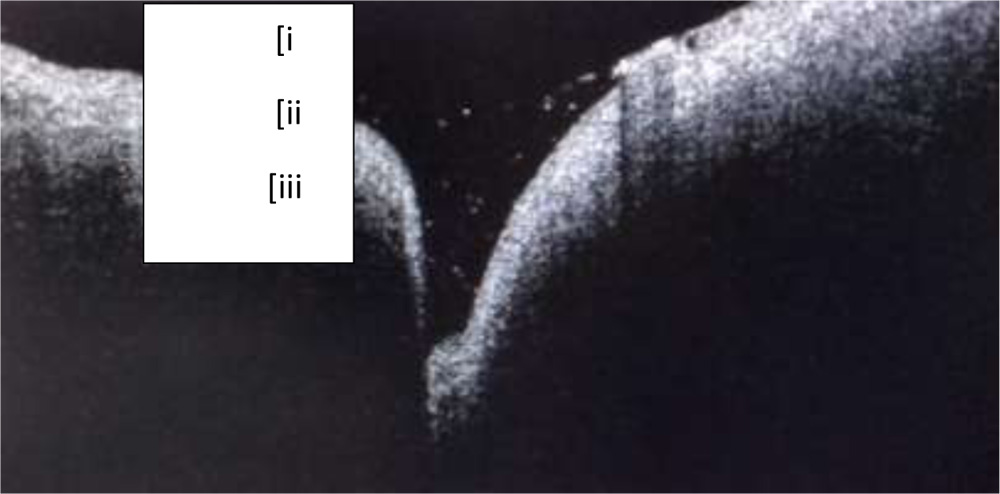
Fig 2: i) Outermost epithelial layer ii) Fibrous tissue layer hyperreflective in comparison to epithelium with a smooth interface in between iii) Muscle of Riolan hyporeflective in comparison to ii) with an irregular interface. Tear film with debris can be seen as punctal content
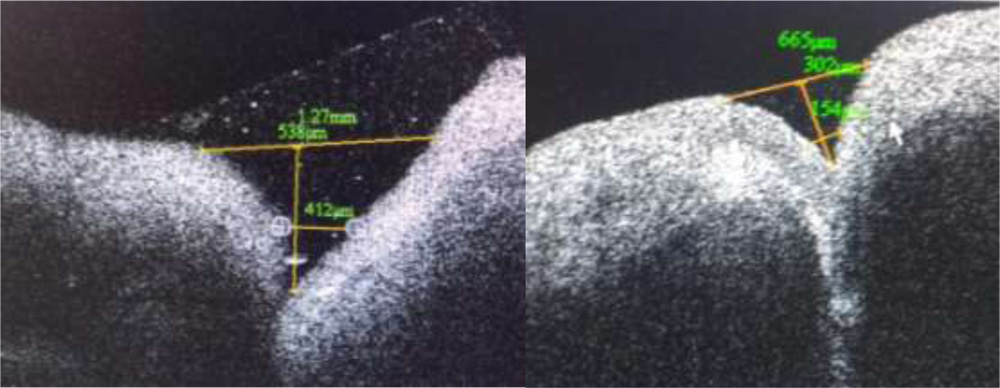
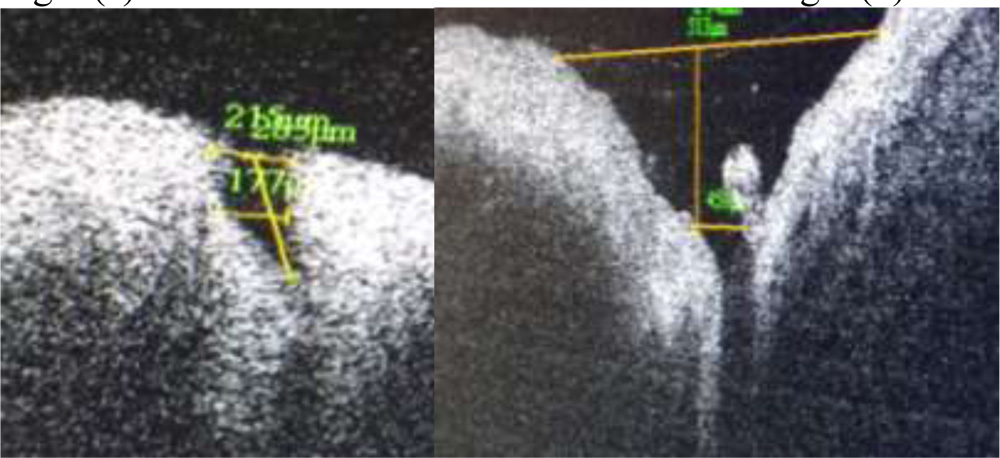
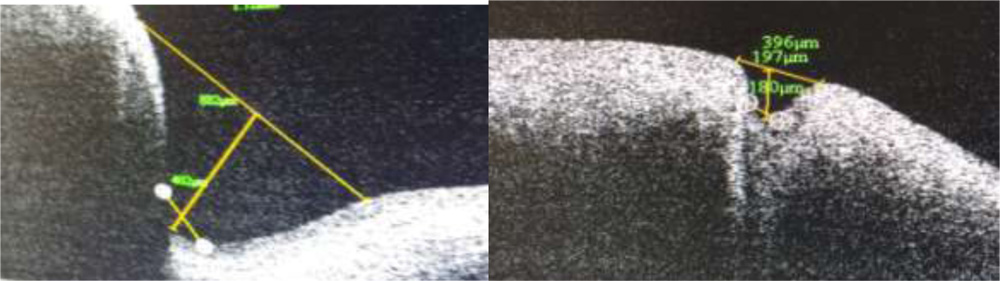
Fig 3 (e) Fig 3 (f)
Fig 3(a-f) Range of punctal morphological variation of shapes detected on SDOCT
Medial wall showed higher slope towards the punctum while lateral wall showed a gradual curvature and slope. Angulation between both medial and lateral wall and the punctum was found to be obtuse in 47 out of 80 puncta.(60%)
Mean maximum outer punctal diameter, inner punctal diameter and depth was recorded as 700.1±424.09µ (median=584.5µ), 245.5±127.54µ (median=199.5µ), 390.85±229.7µ
(median=287µ). No statistically significant difference was found between right and left eyes.
Table 1: Measurement of punctal dimensions on SD OCT
| Parameter | Result |
| No of patients/puncta | 40/80 |
| Age (years) | |
| Mean ± SD | 38.9 ±12.81 |
| Median | 37.5 |
| Range | 20 – 62 |
| Laterality | |
| Right | 40 |
| Left | 40 |
| Outer punctal diameter (microns) | |
| Mean ± SD | 700.1 ± 424.09 |
| Median | 584.5 |
| Range | 264 – 1420 |
| Inner punctal diameter (microns) | |
| Mean± SD | 245.5± 127.54 |
| Median | 199.5 |
| Range | 101- 479 |
| Punctal depth (microns) | |
| Mean ± SD | 390.85±229 |
| Median | 287.0 |
| Range | 132 – 866 |
SD = standard deviation
Positive linear correlation was found between outer punctal diameter and inner punctal diameter, outer punctal diameter and punctal depth and inner punctal diameter and punctal depth on SD ASOCT measurement (Pearson correlation coefficient).
Table 2: Correlation between punctal parameters measured on SD OCT
| Parameters | Pearson correlation coefficient |
| Outer and inner punctal diameter | 0.37 |
| Outer punctal diameter and punctal depth | 0.41 |
| Inner punctal diameter and punctal depth | 0.52 |
80% (64 out of 80) puncta had tears as constituent. Tear film with debris was found in 10% puncta (8 puncta). One punctum showed air bubble with tear as its content. Rest had no visible contents.
Discussion
The present study presents the morphological characteristics of punctum on SD ASOCT. While
Syringing and porbing areconventional options of lacrimal surgery high resolution accurate imaging of lacrimal apparatus could go a long way in getting an accurate information regarding the shape, size, extent, depth and contents of the punctum. Ultrasound biomicroscopy has been tried for imaging but its use has been limited due to lack of good resolution and a necessary contact with eye. Also ultrasound has limited penetration of eyelid skin. OCT is commonly used modality for retinal image acquisition available at most facilities. AS OCT can provide fast high resolution images without any discomfort to the patient.
This study recorded a mean outer punctal diameter of 700.1± 424.09 µ with a wide range of variation. The median value for outer punctal diameter was 584.5µ. This is more than previously recorded values of 214.7µ by Wawrwyznskyet al (2014), 247µ by Allam and Ahmad (2015) and 400.16 µ by Kamal et al7(2015). Timlinet al8recorded a mean outer punctal diameter of 646± 150 µ. All these values reflect a wide range of variation of punctal morphology, particularly punctal shape and depth. A saucer shaped punctum was found have a larger extent compared to a narrow v shaped punctum. A cross line method of scanning was used by Allam and Ahmed while linear scanning was done by Timlinet al and Kamal et al.
Mean inner punctal diameter was recorded as 245.5± 127.54µ at the level of narrowing and change in curvature of inner walls to a vertical from a horizontal one. A definite junction between lower end of punctum and vertical canaliculus could be identified as inner punctum. Inner punctal diameters were found to range from 101µ to 479µ. Allam and Ahmad recorded a mean inner punctal diameter to be 234± 139µ at a similar level. Timlinet al recorded a value of 50 ± 104µ at a depth of 500 µ from external punctum while inner punctal size was recorded as 125± 61µ mid way between punctum and visible lower end by Kamal et al.
The inner punctal diameter recorded by present study is comparable to previous study by Allam and Ahmad. Other studies have recorded this diameter at different levels due to non identification of a separate inner punctum from the upper end of the vertical canaliculus.
The present study recorded mean punctual depth as 390.85± 229µ with a range of 132µ to 866µ. This is comparable to the mean punctal depth recorded by Allam and Ahmad et al as 252 ± 127µ In contrast Timlinet al recorded this value as 544± 327µ . Kamal et al recorded a depth of 890± 155µ. These two measurements represent the vertical canalicular depth as there is no identification of a separate inner punctum in all cases. Wawrzynskietal reported a mean depth of 753 ± 216 µ. This depth is representative of punctal and vertical canalicular depth. All studies report a depth of less than 2mm on imaging. It is difficult to identify the end point of vertical canaliculus and beginning of horizontal canaliculus by OCT imaging. Proximal lacrimal system has been easier to image and three dimensional reconstruction has been shown to be possible by Kamal et al.
Upper punctum could not be evaluated in any case in the present study. None of the previous studies have recorded upper punctal images. This forms a major limitation of AS OCT imaging. A lateral angulation of vertical canaliculus with horizontal canaliculus has been reported by Kakizakiet al9 using cadaveric dissection.. This might limit the visualization of lower end of the vertical canaliculus and contribute to variable measurements of depth.
Examination of proximal lacrimal system byAS OCT provides a base line assessment of puncta. Based on this serial changes in punctal morphology can be compared in cases of chronic topical medication use. Post operative changes following punctal and lacrimal surgeries or effectiveness of interventions for dry ocular surface can be assessed. Different punctal shapes need different punctal plug designs to prevent frequent extrusion.
Further studies may provide information regarding correlation of symptomatic assessment of patients with punctal morphology.
REFERENCES
1.Hurwitz JJ, Pavlin CJ, Hassan A. Proximal canalicular imagingutilizing ultrasound biomicroscopy A: normal canaliculi. Orbit1998;17:S27–S30.
2..Tao H, Xu LP, Han C, et al. Diagnosis of lacrimal canalicular diseasesusing ultrasound biomicroscopy: a preliminary study. Int JOphthalmol2014;7:659–62.
3.Tost F, Bruder R, Clemens S. [20-MHz ultrasound of pre-saccularlacrimal ducts]. Ophthalmologe2002;99:25–8.
4.Wawrzynski JR, Smith J, Sharma A, et al. Optical coherence tomographyimaging of the proximal lacrimal system. Orbit 2014;33:428–32.
5.Allam RS & Ahmed RA (2015): Evaluation of the lower punctum parameters and morphology usingspectral domain anterior segment optical coherencetomography. J Ophthalmol 2015: 591845.
6.Munk PL, Lin DT & Morris DC (1990): Epiphora: treatment by means of dacryocystoplasty with balloon dilation of the nasolacrimal drainage apparatus. Radiology, 177: 687–690.
7.Kamal, M. J. Ali, M. H. Ali, and M. N. Naik, “Fourierdomain optical coherence tomography with 3D and En Faceimaging of the punctumand vertical canaliculus.Astep towardsestablishing a normative database,” Ophthalmic Plastic andReconstructive Surgery, 2015.
8.Timlin, P. Keane, A. Day, M. Abdullah, and D. Ezra, “Characterizationof the lacrimal punctum using spectral domainanterior segment optical coherence tomography: an exploratorystudy,” Investigative Ophthalmology & Visual Science, vol. 55, EAbstract2792, 2014.
9..Kakizaki, Y. Takahashi, T.Nakano, K. Asamoto, S. Kinoshita,and M. Iwaki, “Course of the vertical portion of the lowerlacrimal canaliculus,” Clinical Ophthalmology, vol. 2, no. 4, pp.753–756, 2008.
.