Dr. Prabhav Bansal, B17194,Dr. Rakesh Maggon, Dr. Brig (Mrs ) SagarikaPatyal, Dr. (Lt Col ) Anirudh Singh
Type of article : Original
Author :DrPrabhavBansal
Co authors :Col RakeshMaggon, Brig SagarikaPatyal, Col Anirudh Singh
Co authors : Col Rakesh Maggon, Brig Sagarika Patyal, Col Anirudh Singh
Purpose :To find the correlation between myopiaandage,sex,axial length, pachymetry and anterior chamber depth in young adults.
Keywords : Myopia, Axial length, Pachymetry
Keywords : Myopia, Axial length, Pachymetry
INTRODUCTION
Myopia or short-sightedness is a refractory state of the eye in which parallel rays coming from infinity tend to fall in front of retina with accommodation at rest. It is a complex trait including both genetic and environmental factors as well as gene-environment interactions[1],[2]. High myopia is associated with an increased risk of pathological ocular complications and may lead to blinding disorders such as premature cataracts,glaucoma,retinaldetachment,and macular degeneration[3]. Thus,high myopia is a major cause of legal blindness in many developed countries[4].
Prevalence of myopia varies across populations of different regions and ethnicities. Prevalence of myopia is significantly higher in Asian populations than in populations of European descent, especially in the younger generations in recent decades[5],[6].
The aim of this paper is to evaluate and determine if there is any co relation between myopia and age, sex, axial length (AL), pachymetry and anterior chamber depth (ACD) in young Indians between age group 18 to 30 years.
MATERIALS AND METHODS
MATERIALS AND METHODS
This was an observational, prospective, relational study conducted at Army Hospital Research and Referral. Patients between age group of 18 to 30 years who were referred to the Dept of ophthalmology for refraction were included in the study and were subjected to comprehensive ophthalmological examination including best corrected visual acuity of 6/6, AL, pachymetry and ACD.Inclusion criteria included age between 18 – 30 years, no history of any refractive surgery or trauma to the eye, no associated maculopathy and no history of any other coexisting ocular pathology or any neurological disorder. On the basis of spherical equivalent (SE) of refractive error measured in spherical diopters (DS), subjects were divided in 3 groups:
- Low Myopia ( 1 – 3 DS)
- Moderate Myopia ( 3 – 6 DS)
- High Myopia ( > 6 DS)
DATA ACQUISITION
Best corrected visual acuity of 6/6 was checked with Snellen’s Chart and SE to achieve that was noted. Pachymetry was measured with Ultrasound pachymeter and AL and ACD were measured with IOL Master(Carl Zeiss Meditec, Dublin, CA, USA).
For calculation of pachymetry, the subject was comfortably seated with the head upright and eyes in the primary position of gaze. The probe was sterilized with 70% alcohol and allowed to air-dry. A drop of topical anaesthetic (Proparacaine 0.1%) was instilled in subject’s eyes. The probe was carefully aligned perpendicularly to and cornea was lightly applanated. At least twenty five readings were continually taken and the average calculated as the measured pachymetry (expressed in microns).
For calculation of AL and ACD, the subject was asked to place his chin on the chin rest, and press his forehead against the forehead strap of the IOL Master. The subject’s eyewas aligned to the visual axis by a central fixation light or target. Minimum of 5 readings were taken and their average calculated for both AL and ACD.A single trained operator performedall of the examinations using both devices to avoid inter-observer bias.
STATISTICAL ANALYSIS
SPSS ver., 16.0 was used for data analyses and preparation of figures. The measured variables were tested for correlation with the Pearson co-relation factor (r). Gender-related differences in measured variables were tested with Student’s t-test (unpaired). The relationship between variables was tested with regression analysis. Statistical significance was declared when p-value was ≤0.05. Statistical analysis was done separately for all the 3 groups i.e Low, Moderate and High myopia.
RESULTS
176 eyes of 88 patients were included in the study. 47 of them were females and 41 were males. Various parameters varied as shown in Table 1.
TABLE 1
| PARAMETERS | MIN VALUE | MAX VALUE |
| AGE (yrs) | 18 | 30 |
| SE (DS) | -1.5 | -24.5 |
| PACHYMETRY (microns) | 419 | 570 |
| A L (mm) | 23.09 | 32.12 |
| A.C.D (mm) | 3.06 | 4.36 |
LOW MYOPIA
Refractive error considered in this group was 1 – 3 DS. There were 46 eyes which comprised this group. In this group, axial length showed an insignificant positive co-relation with refractive error, anterior chamber depth showed a significant positive co-relation whereas pachymetry showed an insignificant negative co-relation with refractory error. Pearson co-relation factor with p values are shown in Table 2.
TABLE 2
| LOW MYOPIA, n = 46 | |||||
| AL | ACD | PACHY | |||
| SE (1- 3DS) | r | 0.106 | 0.387** | -0.124 | |
| p value | 0.482 | 0.008 | 0.412 | ||
| *. Correlation is significant at the 0.05 level (p value). | |||||
| **. Correlation is significant at the 0.01 level (p value). | |||||
MODERATE MYOPIA
Refractive error considered in this group ranged from 3 – 6 DS. There were 92 eyes which were included in this group. In this group, both axial length and anterior chamber depth showed an insignificant positive co-relation with refractive error whereas pachymetry showed an insignificant negative co-relation with refractive error. Pearson co-relation factor with p values are shown in Table 3.
TABLE 3
| MODERATE MYOPIA, n = 92 | |||||
| AL | ACD | PACHY | |||
| SE ( 3 – 6 DS) | r | 0.122 | 0.141 | -0.194 | |
| p value | 0.245 | 0.207 | 0.064 | ||
| *. Correlation is significant at the 0.05 level (p value). | |||||
| **. Correlation is significant at the 0.01 level (p value). | |||||
HIGH MYOPIA
Refractive error considered in this group was above 6 DS. There were 38 eyes which were included in this group. In this group, axial length showed a significant positive co-relation with refractive error whereas anterior chamber depth and pachymetry showed an insignificant negative co-relation with refractive error. Pearson co-relation factor with p values are shown in Table 4.
TABLE 4
| HIGH MYOPIA, n=38 | |||||
| AL | ACD | PACHY | |||
| SE (> 6 DS) | r | .764** | -0.273 | -0.182 | |
| p value | <0.001 | 0.102 | 0.275 | ||
| *. Correlation is significant at the 0.05 level (p value). | |||||
| **. Correlation is significant at the 0.01 level (p value). | |||||
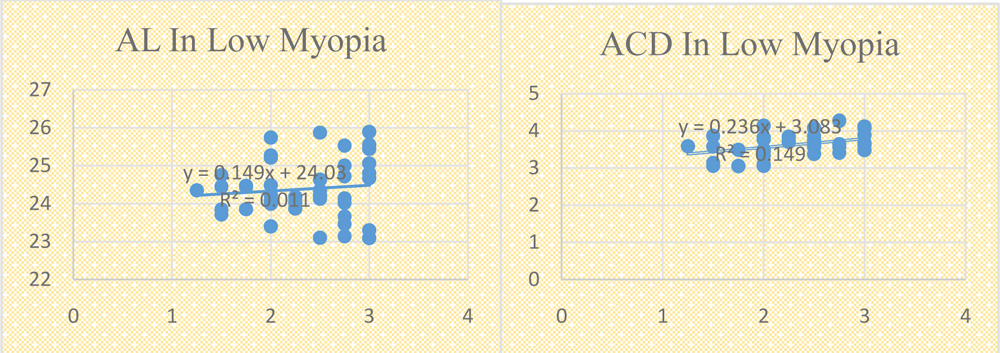
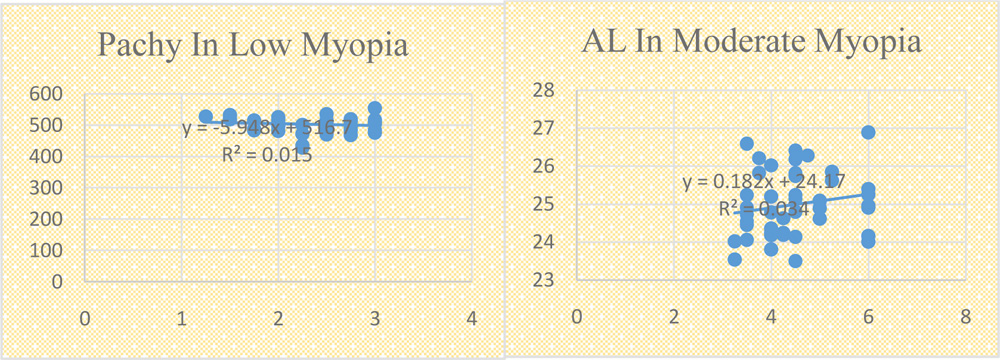
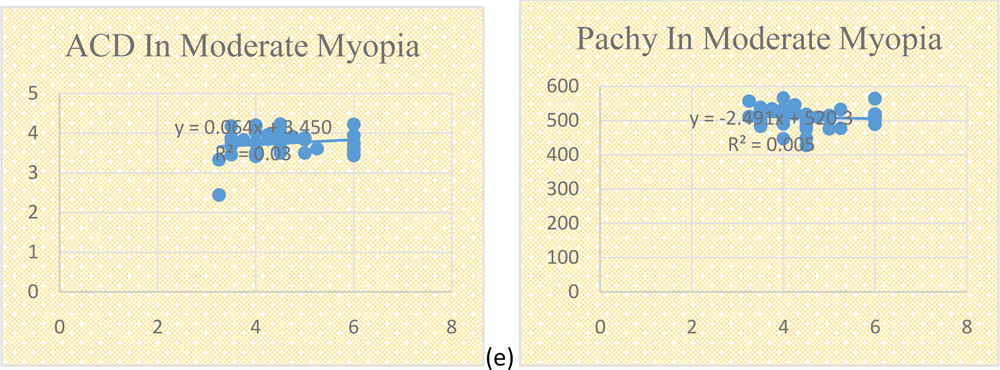
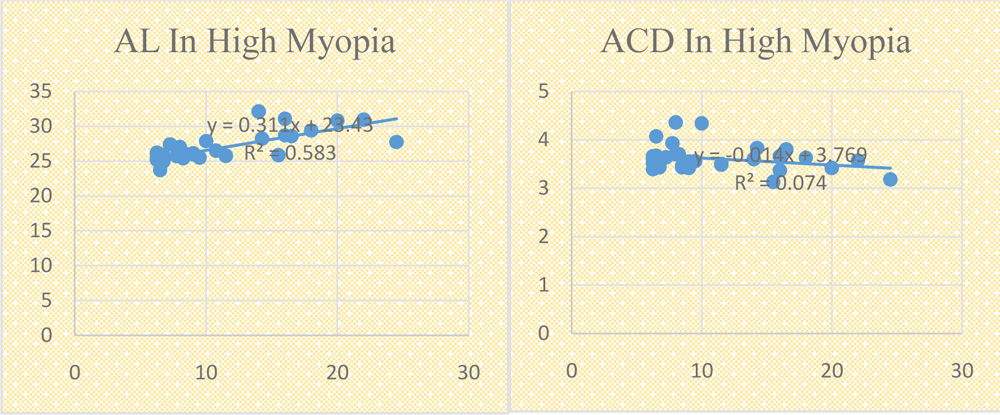
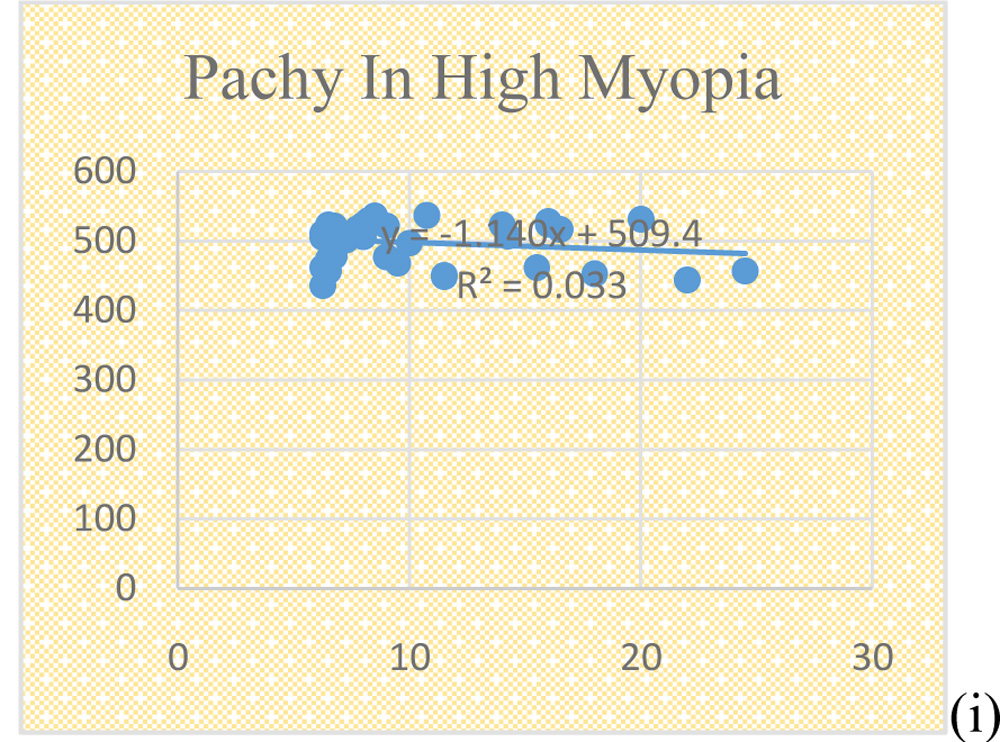
Fig 1. Scatter plots of AL, ACD and pachymetry against myopia ( SE of error) in different groups; (a , b , c) Low myopia group ; (d, e, f) Moderate myopia group ; (g, h, i) High myopia group.
OVERALL CO-RELATION
MYOPIA VS AXIAL LENGTH
There was a statistically significant positive correlation between myopia and AL with Pearson correlation factor ( r ) being 0.757 (p < 0.001). Although AL was found to have statistically insignificant positive co-relation with myopia in low and moderate myopia but when all the 3 groups were analysedaltogether the result came out to be statistically significant.
MYOPIA VS PACHYMETRY
There was a statistically significant negative correlation between myopia and pachymetry with Pearson correlation factor being 0.155 (p < 0.039). Although pachymetry was found to have insignificant negative co-relation in all the three groups but when all the 3 groups were analysed together the result is statistically significant and negatively co-related.
MYOPIA VS ANTERIOR CHAMBER DEPTH
There was negative correlation between myopia and anterior chamber depth with Pearson correlation factor being 0.131 but it was statistically insignificant as p = 0.094. Since ACD was positively correlated in low as well as moderate myopia but negatively correlated with high myopia, this finding seems to have been influenced by the extreme readings seen in high myopia group
MYOPIA VS AGE
No significant correlation of myopia could be found with the age of the patient (Pearson correlation factor was 0.028 and p value was 0.708).
MYOPIA VS SEX
82 eyes were of male patients as compared to 94 eyes of females. Mean SE of refractory error in males was 5.53 DS ± 4.02 DS and in females it was 4.94 ± 3.44 DS. There was no significant correlation of myopia with sex ( p = 0.296) as shown in table 5.
TABLE 5
| SEX | N | Mean SE | Std. Deviation | t-value | p-value |
| Male | 82 | 5.53 | 4.02 | 1.048 | 0.296 |
| Female | 94 | 4.94 | 3.44 |
DISCUSSION
DISCUSSION
The introduction of laser refractive procedures (photorefractive keratectomy [PRK] and laser in situ keratomileusis [LASIK] brought about increasing interest in the determination and evaluation of differences in normal central corneal thickness (CCT). Axial length (AL) of the eyeball is the distance from the posterior corneal surface to an interference peak corresponding to retinalpigmentepithelium/Bruch’smembranes[7,8].Chenetal[9] foundnostatistically significant correlation between CCT and AL. They claimed that the eye elongates with sclera thinning but CCT may not be affected by the sclera thinning that occurs during eye elongation in myopia. However, Chang et al[10] hypothesized that there might be a stretching-related increase in corneal area associated with axial elongation and scleral thinning but could find no statistically significant relationship between AL and CCT in a Taiwan based clinical study.A previous study that examined the general population found that greater AL was significantly associated with a thicker cornea using univariate analysis; however the association was not found to besignificant using multivariate analysis.[11]
In our study, AL showed a statistically significant positive correlation with SE of refractory error and pachymetry showed a statistically significant negative correlation with increasing myopia. When subjects were divided in 3 groups on the basis of SE i.e Low, Moderate and High myopia, AL was positively correlated with myopia in all the 3 groups and pachymetry was found to be negatively correlated with the refractive error. This implies that as the eyeball elongates, there is an increase in refractive error and an associated decrease in the pachymetry.
To implant phakic intraocular lenses, ACD must be measured to avoid complications such as an attack of acute angle-closure and also associated endothelial cell loss.[12,13] Previous population-based studies have shown that ACD is associated with age, gender, body stature, AL, and lens thickness.[14–18] These studies examined the general population and focused on factors associated with reduced ACD. Jivrajka et al. reported a significant positive correlation between AL and ACD in cataractous eyes.[19] In the Jivrajka study, greater than 99% of participants had an AL < 27 mm. In a previous study, Hoffmann et al. showed that in eyes with an AL of 21.63–25.84 mm, AL was positively correlated with ACD and in eyes with an AL ≥ 25.84 mm, AL was negatively correlated with ACD.[20] They included 23,239 eyes with cataracts in the study with a mean subject age of 74 years. Hye Jin Chung and Chan Kee Park conducted a study on ocular biometers and found that ACD increased as AL increased in the moderate-myopia group (>−6 D). However, in the high-myopia group, ACD showed no association with AL, and showed a tendency to decrease with decreasing SE. [21]
In our study, ACD showed a positive correlation with refractive error in Low as well as Moderate myopia but showed a negative correlation with refractory error in High myopes (> 6 DS). This implies that upto a certain point in the AL increase, both the anterior and posterior segments of the eyeball contributed to the overall increase in the AL. After this point was reached, axial elongation was due to the elongation of the posterior part, so overall ACD seemed not to increase. This posterior elongation could aggravate the pathological myopia in the posterior segment of the eyeball leading to vitreous and retinal changes
Age and sex do not seem to have a significant correlation with myopia.
CONCLUSION
Surgical treatment of myopia is either keratorefractive where pachymetry plays an important role in determining the type of surgery keeping the residual stromal bed within safe limits or phakic IOL’s where anterior chamber depth plays a crucial role in laying down the criterias for declaring a patient fit for phakic IOL’s. Positive correlation of axial length with myopia proves that as the axial length increases refractory error also increases. Positive correlation of ACD with myopia in low to moderate myopes only indicates that phakic IOL’s can be a good option in low to moderate myopes but may not be that good an option in high myopes. Negative correlation of pachymetry with myopia indicates that pachymetry can be a restricting factor in keratorefractive surgeries as the refractory error of the patient increases.
The ocular biometric parameters we examined are closely interrelated. Understanding the changes in ocular biometric parameters as myopia increases is very important in not only interpreting the ocular data but also modeling the pathology of ocular disease and also deciding in the approach for the management of the patient.
Because the present study was performed using normal eyes, further studies on pathologic eyes would be valuable. In addition, since all the participants were Indian, the effect of race should be examined.
FINANCIAL DISCLOSURES
Author has no financial disclosures.
REFERENCES
- Bialasiewicz AA. Genetics of myopia. Oman J Ophthalmol. 2011;4(2):49. [PMC free article] [PubMed]
- Hornbeak DM, Young TL. Myopia genetics: a review of current research and emerging trends. Curr Opin Ophthalmol. 2009;20(5):356–362. [PMC free article] [PubMed]
- Hayashi W, Shimada N, Hayashi K, Moriyama M, Yoshida T, Tokoro T, Ohno-Matsui K. Retinal vessels and high myopia. Ophthalmology. 2011;118(4):791–791e2. [PubMed]
- Charman N. Myopia: its prevalence, origins and control. Ophthalmic Physiol Opt. 2011;31(1):3–6.[PubMed]
- He M, Zheng Y, Xiang F. Prevalence of myopia in urban and rural children in mainland China. Optom Vis Sci. 2009;86(1):40–44. [PubMed]
- Lam CS, Lam CH, Cheng SC, Chan LY. Prevalence of myopia among Hong Kong Chinese schoolchildren: changes over two decades. Ophthalmic Physiol Opt. 2012;32(1):17–24. [PubMed]
- Hitzenberger C.K. Optical measurement of axial length by laser Doppler interferometry. Invest Ophthalmol Vis Sci. 1991;32:616–620. [PubMed]
- Schmidt G.F., Papastergiou G.I., Nickla D.I. Validation of laser Doppler interferometric measurement in vivo of axial eye length and thickness of fundus layer in chicks. Curr Eye Res. 1996;15:691–696. [PubMed]
- Chen M.J., Liu Y.T., Chen Y.C., Chou C.K., Lee S.M. Relationship between central corneal thickness, refractive error, corneal curvature, anterior chamber depth and axial length. J Chin Med Assoc. 2009;72:133–137. [PubMed]
- Chang S.W., Tsai I.L., Hu F.R., Lin L.L., Shih Y.F. The cornea in young myopic adults. Br J Ophthalmol. 2001;85:961–970. [PMC free article] [PubMed]
- Hwang YH, Kim HK, Sohn YH. Central corneal thickness in a Korean population: the namil study. Invest Ophthalmol Vis Sci 2012;58:6851–6855.
- Rufer F, Schroder A, Klettner A, Frimpong-Boateng A, Roider JB, Erb C. Anterior chamber depth and iridocorneal angle in healthy White subjects: effects of age, gender and refraction. Acta Ophthalmol 2010;88:885–890.
- Saxena R, Boekhoorn SS, Mulder PG, Noordzij B, van Rij G, Luyten GP. Long-term follow-up of endothelial cell change after Artisan phakic intraocular lens implantation. Ophthalmology 2008;115:608–613 e601.
- Hashemi H, KhabazKhoob M, Mehravaran S, Yazdani K, Mohammad K, Fotouhi A. The distribution of anterior chamber depth in a Tehran population: the Tehran eye study. Ophthalmic Physiol Opt 2009;29:436–442.
- He M, Huang W, Zheng Y, Alsbirk PH, Foster PJ. Anterior chamber depth in elderly Chinese: the Liwan eye study. Ophthalmology 2008;115:1286–1290, 1290 e1281–1282.
- Xu L, Cao WF, Wang YX, Chen CX, Jonas JB. Anterior chamber depth and chamber angle and their associations with ocular and general parameters: the Beijing Eye Study. Am J Ophthalmol 2008;145:929–936.
- Sng CC, Foo LL, Cheng CY, Allen JC Jr, He M, Krishnaswamy G, et al. Determinants of anterior chamber depth: the Singapore Chinese Eye Study. Ophthalmology 2012;119:1143–1150.
- Jonas JB, Nangia V, Gupta R, Khare A, Sinha A, Agarwal S, et al. Anterior chamber depth and its associations with ocular and general parameters in adults. Clin Experiment Ophthalmol 2012;40:550–556.