Dr.Sheetal Brar, B15612, Dr. Sri Ganesh
Type of article: Original
Contributors
- Dr. Sri Ganesh , MS, DNB
- Dr. Sheetal Brar, MS
Department(s) and institution(s) affiliation of all authors : Nethradhama Superspeciality Eye Hospital, Bengaluru, Karnataka, India
Corresponding Author:
Name : Dr. Sheetal Brar
Address: Nethradhama Superspeciality Eye Hospital, 256/14, Kanakapura main road, 7th Block, Jayanagar, Bengaluru, Karnataka, India-560070
Phone numbers: +919591002092
E-mail address: brar_sheetal@yahoo.co.in
Total number of pages: 19
Source(s) of support:Nil
Conflict of interest and financial disclosure- Nil
Title: Incidence and results of cyclotorsion compensation in patients undergoing myopic SMILE correction
Purpose:To study the incidence of intraoperative cyclotorsion and the safety, efficacy and outcomes of manual cyclotorsion compensation in SMILE for myopic astigmatism.
Methods: Eligible patients with myopia from -1 to -10 D spherical equivalent (SE) with a minimum astigmatism of -0.75 D undergoing SMILE were included. Intraoperative cyclotorsion compensation was performed by gently rotating the cone and aligning the 0º-180º limbal marks with the horizontal axis of the reticule of the right eye piece of the femtosecond laser after activating the suction.
Results: 81 left eyes from 81 patients were analysed for vector analysis of astigmatism.The mean cyclotorsion was 5.64 ± 2.55(range 2-12)degrees.No significant differences were found for surgically induced astigmatism (SIA),difference vector(DV), angle of error(AE), correction index(CI), magnitude of error(ME), index of success(IOS) and flattening index(FI) between 2 weeks and 3 months (p>0.05)
The eyes were categorised into low(≤ -1.5 D, n=37) and high(>1.51 D, n=44) cylinder groups. At 3 months, intergroup analysis showed a comparable CI of 0.97 for low and 0.93 for high cylinder group, suggesting a slight undercorrection of 3 % and 7% respectively (p=0.14).However, the AE and IOS was significantly lower in high compared to the low cylinder group(p=0.032, p=0.024 for AE and IOS respectively),suggesting better alignment of the treatment in high cylinder group. However, the mean UCVA of both groups was comparable (p=0.21),suggesting good visual outcomes in the low cylinder group despite a less favourable IOS.
Conclusion: Manual compensation may be a safe, feasible and effective approach to refine the results of astigmatism with SMILE,especially in higher degrees of cylinders.
Key words: Cyclotorsion, SMILE, Myopic Astigmatism
Trial registration number: CTRI/2014/04/004570
Precise-The study reports the outcomes in myopic astigmatism with manual compensation of cyclotorsion using preoperative limbal marking as a guide in SMILE. The results suggest better predictablility of astigmatism correction with the technique described.
Introduction
The refractive outcome of astigmatism correction has been shown to depend upon the accuracy of the axis treatment .Any rotational movement of the eye(cyclotorsion) during treatment may cause shift in the treatment axis leading to undesirable results like undercorrection and induction of aberrations(1,2,3). Most of the currently available excimer laser platforms have the ability to detect and compensate for the static and dynamic cyclotorsion due to positional changes and treatment by advanced softwares and eye tracking(1,4).
It was found in LASIK that active cyclotorsion error correction improved the accuracy of cylinder correction(4,5,6).While there are numerous studies on cyclotorsion and its compensation in LASIK, significant data lacks in this regard for the all femtosecond , flapless small incision lenticule extraction (SMILE) procedure for correction of myopic astigmatism. Studies on FLEx and SMILE have shown significant undercorrection of astigmatism over time (7,8,9). The probable explanation of these results could be the non-availability of an active eye tracking software in the VisuMax femtolaser system used to perform these procedures. Since no definite method of cyclotorsion compensation exists for SMILE, this may also be considered a potential limitation of this procedure at present.
Previous studies on LASIK suggested that manual markings were equally safe and effective as the automated dynamic eye trackers for cyclotorsion compensation during surgery(10).Based on these observations, we attempted to investigate the feasibility of manual compensation of the intraoperative torsional error by using limbal markings as a guide, in patients with clinically significant myopic astigmatism undergoing the SMILE procedure.
In this study, we describe a simple and practical method for the manual compensation of cyclotorsion during ReLEx SMILE procedure in patients with significant myopic astigmatism (>0.75 D). We also evaluate the safety, efficacy and reliability of this technique in terms of cylindrical correction and post- operative refractive outcome in a 3 month follow-up prospective, interventional study.
Materials and Methods
This prospective, non- randomised study was approved by institutional ethics committee and adhered to the tenets of the Declaration of Helsinki. Written informed consent was obtained from all patients participating in the study.
Inclusion criteria were- age between 21- 40 years, myopic astigmatism within the range upto -10 D spherical equivalent (SE) with a minimum astigmatism of -0.75 D, stable refraction (<0.5 D change in past 12 months), corrected distant visual acuity(CDVA) of 20/30 or better, healthy tear film and ocular surface, absence of corneal ectatic diseases such as keratoconus, corneal scars , absence of any retinal pathology likely to affect visual outcomes and assured follow-ups
Eyes with thin corneas (central pachymetry <480 µm), diagnosed or suspicious cases of corneal ectatic conditions, severe dry eyes (Schirmers 1 <10 mm), severe contact lens induced allergy, patients on systemic steroids, immune suppresants, oral contraceptives, antidepressants and pregnant females were excluded from the study.
Preoperative evaluation
All patients underwent a thorough preoperative evaluation including anterior and posterior segment examination, assessment of uncorrected and corrected distance visual acuity, corneal topography using Pentacam HR (Oculus Optikgeräte GmbH, Wetzlar, Germany) and Orbscan II (Bausch and lomb, Rochester, NY), contrast sensitivity using Functional Acuity Contrast Test.(F.A.C.T. STEREO OPTICAL CO., INC. Chicago), abberometry(Hoya iTrace, surgical workstation, Japan), specular microscopy ( Tomey, Japan) and dry eye evaluation (Schirmer 1 and tear film break up time).
Patients using soft and rigid contact lenses were instructed to discontinue their lenses at least one and 3 weeks respectively, prior to the topographic evaluation.
Treatment planning: On all eyes, irrespective of the degree of myopia, a 10% overcorrection nomogram was applied to both the spherical and cylindrical components of the refractive error.
Surgical technique
All surgeries were performed by a single experienced refractive surgeon(S.G.)under topical anesthesia. The procedure was performed using the VisuMax femtosecond laser (Carl Zeiss Meditec, Jena, Germany), with a pulse repitition rate of 500 KHz, cut energy of 160 nj , 6.5- to 7-mm optical zone, cap thickness of 120 µm and a 2 mm superior incision following the standard surgical technique(ref our paper). The treatment was centered on the visual axis. Mean optical zone used was 6.5±0.23 mm.
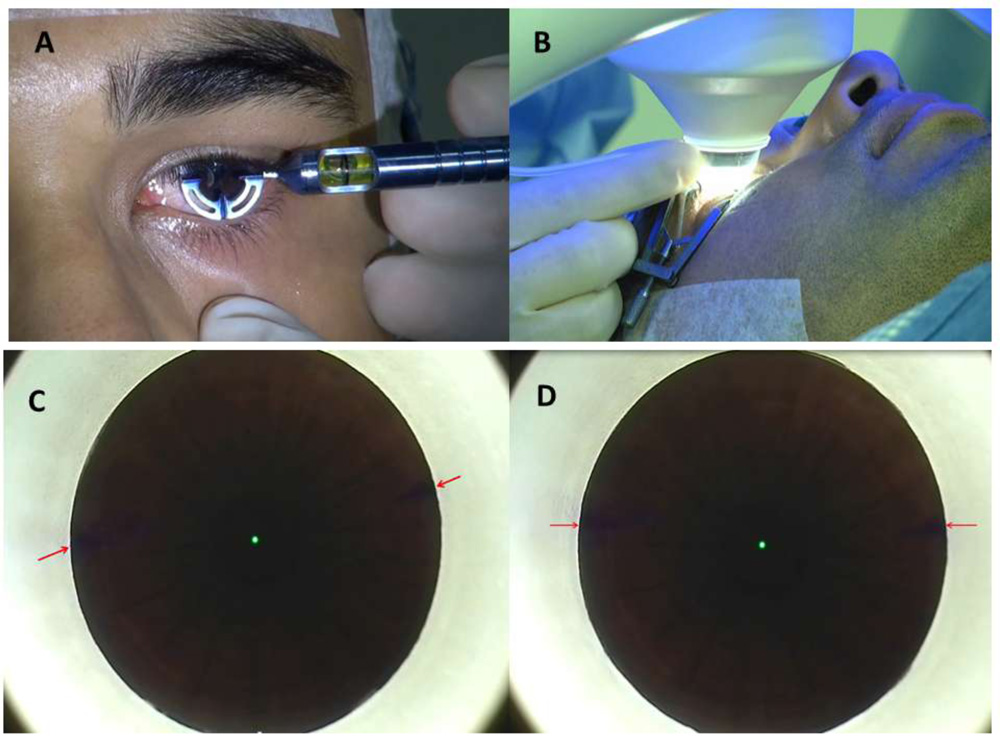
Pre-operatively, the limbus was marked in the 0º to 180º axis with an infrared transmitting dye (Viscot surgical skin marker 1436; Viscot Medical) using either a marker pen or Ganesh bubble marker (Epsilon Surgicals; Figure 1A,) in the upright position. The patient was then positioned under the VisuMax FS laser and instructed to look into the green flashing fixation light. Once proper centration was achieved, the eye was docked to the patient interface followed by application of suction. At this point, the extent of cyclotorsion if any, was determined using the reticule(present in the right eyepiece) and any cyclotorsion( incyclo/excyclo) was manually compensated by gently rotating the contact glass to align the horizontal marks on the eye to 0º to 180º axis of the reticule ( Figure 1B,C,D)(Supplementary video, available in the online version). Once both were aligned, the active laser process was started to create the refractive lenticule. After the lenticule creation by the femtosecond laser, the anterior and posterior lenticule planes were dissected using a blunt dissector followed by lenticule extraction through the side cut. Interface was washed with balanced salt solution.
Postoperative medications included topical 0.3% Ofloxacin (Exocin®, Allergan, Irvine, U.S.A.) 4 times for 3 days, 0.1% prednisolone acetate eye drops (Pred Forte®, Allergan, Irvine, U.S.A.) in tapering dosage for 4 weeks, and lubricants 4 times for 4 weeks or more.
All surgeries were uneventful and no complications such as suction loss, black spots, difficult dissection or incomplete separation of lenticule due to the ink marks blocking the laser occurred in any of the eyes.
Patients were followed up on postoperative day 1, 2 weeks and 3 months. At every visit, slit lamp examination for corneal state, NCT and uncorrected distant visual acuity (UDVA) was evaluated.At each follow-up visit from 2 week onwards, assessment of UDVA, manifest refraction, corrected distant visual acuity (CDVA) and topography was also performed.
Statistical Analysis: SPSS software for Windows version 17.0.0 (IBM Corp., Armonk, NY) was used for statistical analysis .All values were expressed as mean ± standard deviation (SD). Independent sample t test was carried out for intergroup comparison and paired t test was used for intragroup comparison of means. A p-value of 0.05 or less was considered statistically significant.
Vector analysis of astigmatism
Only the left eyes were included in the analysis. Astigmatism outcomes were reported according to standardised format(11,12,13).
Results
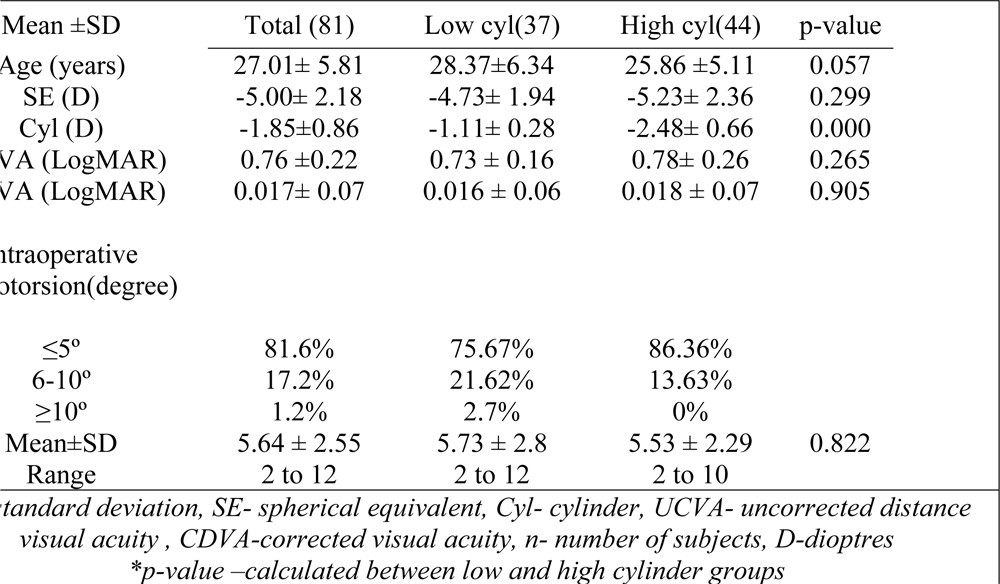
A total of 81 left eyes from 81 patients with an attempted astigmatic correction of 0.75 D were analysed for visual and refractive results and vector analysis of astigmatism. The eyes were categorised into low (≤ -1.50 D, n=37) and high (-1.51 D and above, n=44) cylinder groups, based upon the magnitude of preoperative astigmatism .The preoperative patient characteristics are given in Table 1.
For the left eyes, incyclotorsion was defined as clockwise, and excyclotorsion was defined as anticlockwise rotation of the limbal marks in relation to the 0º-180º of the eye piece reticule. Incyclotorsion was more commonly observed (44% eyes) compared to excyclotorsion(38% eyes), while 18% eyes did not show any cyclotorsion. However, for the purpose of convenience of analysis, both incyclo and excyclotorsion were considered broadly as “cyclotorsion” and separate results were not analysed for incyclo and excyclotorsion.
Overall, the average cyclotorsion observed was 5.64 ± 2.55 (range 2-12 )degrees. The magnitude of cyclotorsion was ≤5º in 81% , between 6-10º in 17.6% and ≥ 10 degrees in 1.2% of eyes .The mean cyclotorsion was comparable in both the low(5.73º ± 2.8º) and high cylinder group(5.53º ± 2.29º ), with no statistically significant difference between their values (p=0.822),(Table 1).
Visual Outcomes
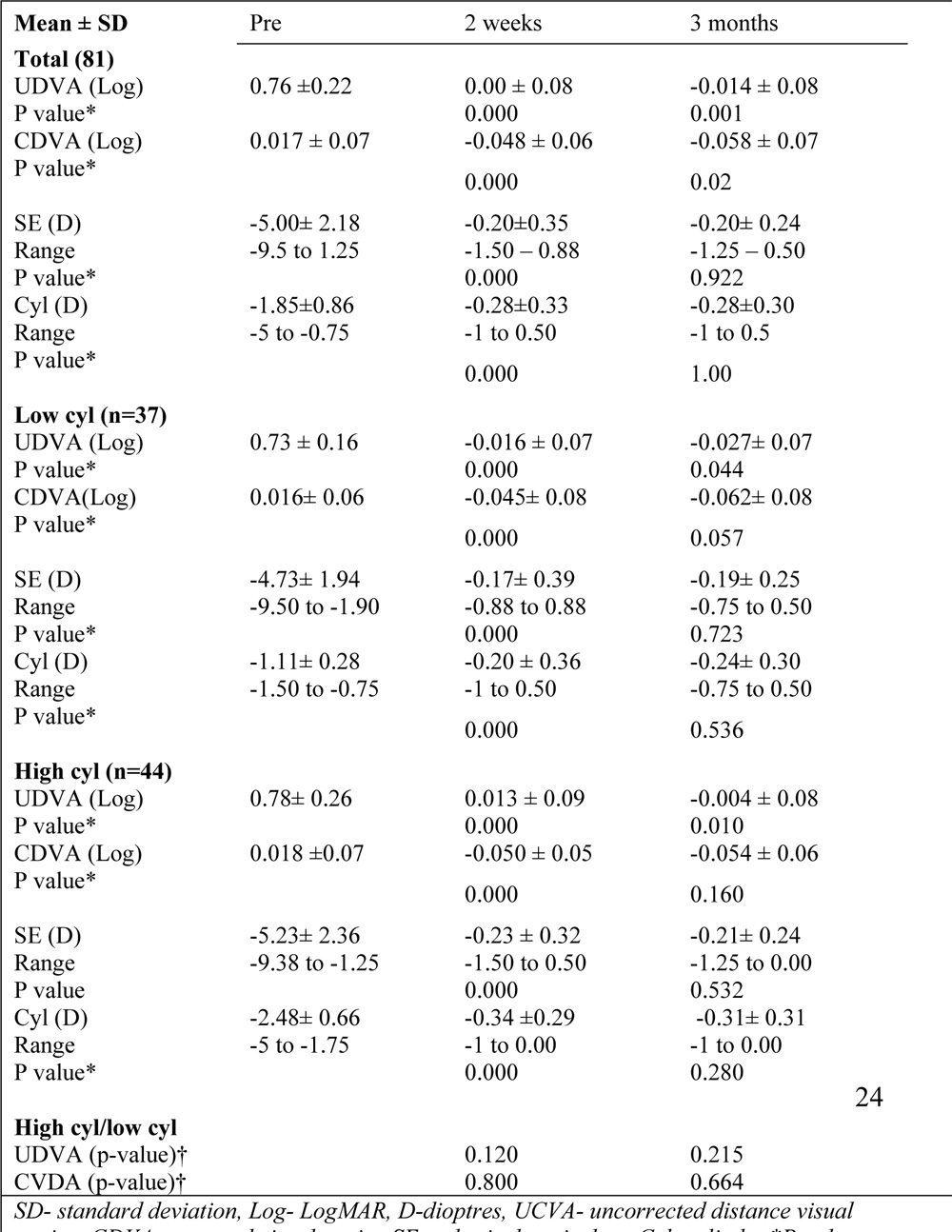
The mean UDVA showed significant improvement in both low and high cylinder groups from 2 weeks to 3 months post –op (p <0.05 for both groups).However, there was no statistically significant improvement in CDVA in either group over time (Table 2).
Efficacy (Post-operative UDVA/ Preoperative CDVA)
All eyes had UDVA 20/32 or better at 3 months, with 84% eyes with UDVA of 20/20 or better. However, the percentage of eyes achieving UDVA 20/20 or better was higher in the low (95%) versus the high cylinder group(75% )
Safety (Post-operative CDVA/ Preoperative CDVA)– Overall 56% eyes gained 1 or more lines of CDVA at the end of 3 month follow-up.In the high cylinder group, the gain in CDVA was more (60%) compared to the low cylinder group(54%).No eye in either group had loss of CDVA compared to pre-operative corrected vision.
Refractive outcomes
The mean SE reduced from -5.00 ±2.18 D preoperatively to -0.20±0.24 D, at the end of 3 months follow up (p=0.000). 95% eyes were within ±0.50 D, while all eyes were within 1.50 ± D of SE correction (Table 2).
Overall, the predictability of cylinder correction was excellent with all eyes within ±1.00 D of astigmatism correction at 3 months(Fig 4A).However, the predictability was slightly better in the low (average deviation -0.04D) versus the high cylinder group(average deviation -0.21D),indicating more under-correction of astigmatism treatment in the latter group
The post-operative SE and cylinder remained fairly stable with no significant difference between 2 weeks and 3 months (p>0.05)
Vector analysis.
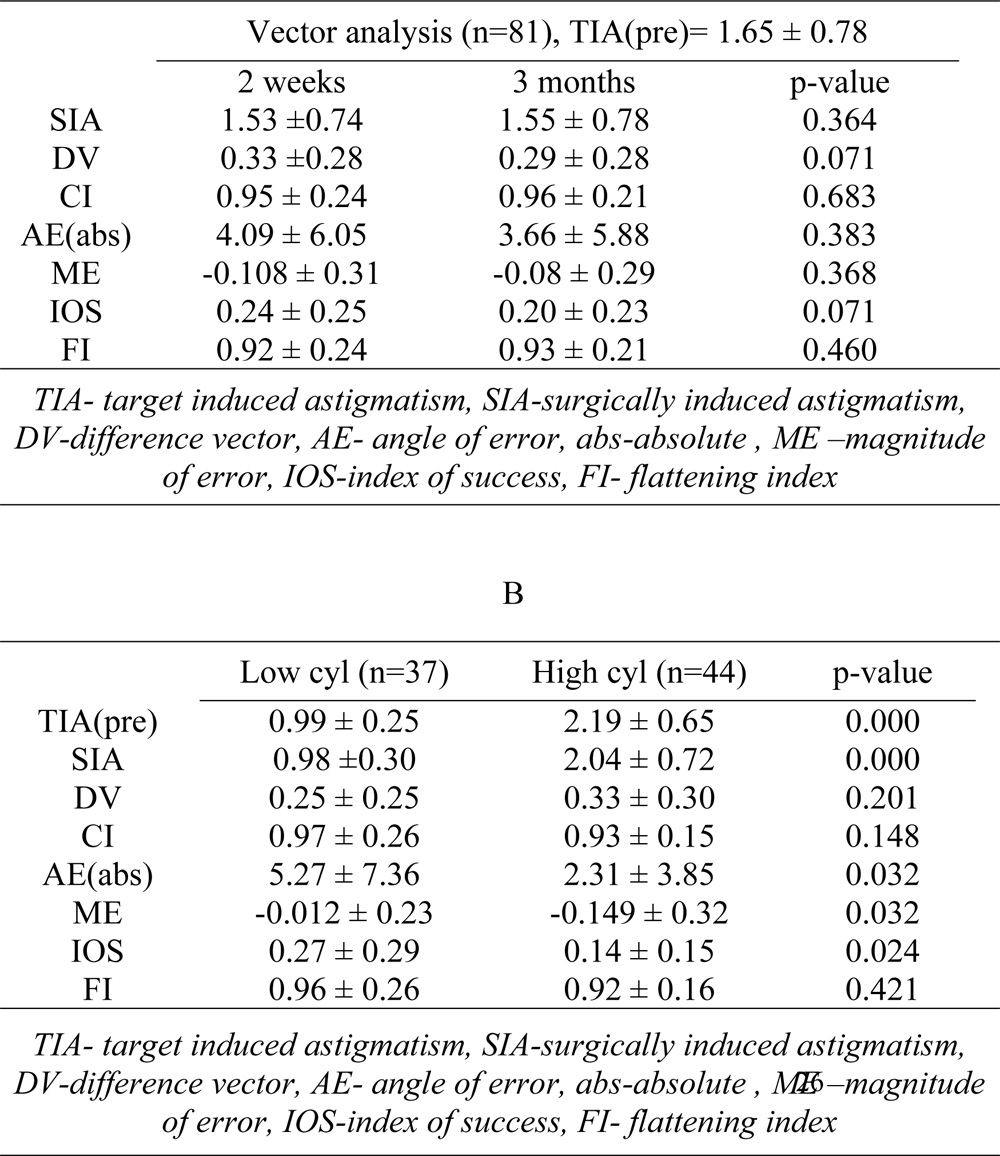
The vector analysis results of the total 81 eyes, using 2 weeks and 3 month refractive data are shown in table 3. No significant differences were found for surgically induced astigmatism (SIA), difference vector(DV), absolute angle of error(AE), correction index(CI), magnitude of error(ME), index of success(IOS) and flattening index(FI) between 2 weeks and 3 months (p>0.05).
Intergroup analysis at 3 months showed that there was no significant difference between the low and high cylinder groups in terms of the DV, CI, Angle of error(AE) refractive and flattening index. However, the absolute AE and IOS was significantly higher in low compared to high cylinder group (p=0.032, p=0.024 for AE and IOS respectively) . The ME, on the other hand, was higher in high cylinder compared to low cylinder group (p=0.032) (Table 3).
Discussion
Alpins et al through vector analysis demonstrated that the proportion of loss of flattening effect is 1.5% when treatment is misaligned by 5°, 13.4% when 15° and as high as 50% when 30°(13). This emphasises the importance of treatment alignment for the successful correction of astigmatism during corneal refractive surgery.
Rotational movements during excimer laser refractive surgery have been traditionally reported as static and dynamic, the former occuring before
surgery when the patient switches from upright to the supine position and the latter occurring during the photoablation1. In SMILE, however, the potential torsional errors that can be appreciated with the naked eyes would be mainly due to static cyclotorsion. However, additional movements may occur due speculum insertion, application of suction and squeezing of the eye during treatment which may be subtle to detect.
Previous studies evaluating astigmatism correction showed superior results with femtosecond LASIK compared to SMILE(14,15). Chan et al showed that the alignment of treatment was more variable in SMILE, leading to a lower efficacy compared to LASIK at 3 months in eyes with low to moderate myopic astigmatism(13).
Ivarsen et al demonstrated a significant undercorrection of astigmatism and an increased error of treatment with higher attempted cylinder correction. The reported undercorrection was 13% per dioptre of attempted cylinder correction in low astigmatic and 16% per diopter in highly astigmatic eyes. This was mainly attributed to non-compensation of errors of cyclotorsion and non-application of nomograms during the procedure(16).
However, in contrast to the study by Ivarsen et al, excellent results for astigmatism treatment were achieved in the current study with SMILE. Since we attempted compensation of cyclotorsion manually and also applied a 10% nomogram (based on our experience and post-op results), the accuracy of astigmatism correction observed was far better compared to the results reported in previous studies(14,15,16).This was indicated by the high correction indices of 0.97 and 0.93 for low and high cylinder groups, suggesting an under correction of 3% and 7% respectively, at 3 months. One reason for more undercorrection in high group may be a lower mean age compared to the low cylinder group, hence patients in this group were younger and more susceptible to regression. Also, higher degrees of cylinders were shown to have a tendency for greater undercorrection over time16. However, from a clinical point of view, slight undercorrection would be preferred to overcorrection because a change in the direction of the cylinder axis probably may be poorly accepted by patients.
In general vector analysis, three indices that enable examination of the relationship of three separate vectors to the treatment vector (the TIA) and comprise complete approach to astigmatism analysis were described -Index of success(IOS),Flattening index(FI) and correction index(CI)17. It was emphasized that a CI of 1.0 does not ensure complete success of the astigmatism surgery since any misalignment between the actual treatment (SIA)and the intended treatment(TIA) may result in an angle of error(AE), leaving a remaining DV and an IOS both greater than zero, despite the magnitude of error being zero17.This would reasonably explain the observations in the low astigmatism group in our study ,wherein the CI although was close to 1 (0.97), but IOS had higher and thus a less favourable numerical value than the high cylinder group, indicating greater misalignment in the low cylinder group.
Although, the absolute Angle of Error(AE) and Index of success(IOS) was significantly higher in low compared to high cylinder group, indicating a suboptimal correction of astigmatism, the visual outcomes in terms of uncorrected visual acuity were similar in both groups at 3 months. This may suggest that it may not be compulsary to manually correct for cyclotorsion in lower degrees of astigmatism in SMILE. The accuracy of treatment of lower degrees of astigmatism would be dependent upon a various factors such as the reliability of pre-operative measurement of the magnitude and axis of the cylinder and manual marking, and also assessement of extent of intra-operative cyclotorsion. Due to these reasons, the advantages of manual compensation in low cylinders may not be ascertained, especially if the intra-op cyclotorsion is less(<5º). However, it may have a definite advantage in moderate to high degrees of astigmatism, as even minimal meridional errors may have significant negative refractive consequences18.
In this study, in the majority of eyes (81.6%), the magnitude of intra-operative cyclotorsion was ≤ 5 degrees. However, rotation of > 5 degrees was found in 18.4% of eyes and of 10 degrees or more in 1.2%.Studies have shown that rotation of 5 degrees or more can induce significant undercorrection of the astigmatic component of the refraction and that undercorrection is more noticeable as the degree of astigmatism increases(19,20).Hence, based on the results of this study, we recommend manual compensation of cyclotorsion error for all eyes with high astigmatism (>1.5 D) with any degree of cyclotorsion and low astigmatism(≤1.5D) with ≥5 degrees, using the technique described.
In terms of flattening effect achieved, our study showed better flattening index(0.93) at 3 months compared to study by Kobashi et al, which showed insufficient flattening with both FLEX and SMILE(median flattening indices of 0.79 to 0.80) (21).
The probable explanation for the constant and significant improvement in UCVA from 2 weeks to 3 months across both the low and high cylinder groups could be an improvement in visual quality due to interface healing, reduction in aberrations and decrease in post-operative dryness in the due course of time (22,23)
There were at two potential limitations to this study. Firstly, we did compare our results with a control group without cyclotorsion compensation. This was done on ethical grounds, as we had observed some cases with suboptimal outcomes with high cylinders and after using this technique our outcomes with astigmatism improved significantly. Secondly, we determined the postoperative astigmatism at 3 months, when the corneal shape was considered to have been stabilized, taking into account the wound-healing responses of the cornea. However, a longer follow-up may be desirable to evaluate the long term stability of the results obtained with this technique.
Nevertheless, to the best of our knowledge, this is the first preliminary report on the outcomes of astigmatism correction in SMILE using manual compensation. In our experience, gentle rotation of the cone does not lead to loss in suction and no complications occur due to limbal marking when performed using the infrared transmitting ink marker. Hence, it may be a safe, simple and effective approach to improve results of astigmatism with SMILE, in the absence of an active eye tracker in the current version of VisuMax FS laser. However, prospective, randomized controlled studies with a longer follow-up may be necessary to confirm the authenticity of our results.
Legends:
Figure 1.(A) -Preoperative limbal marking with the Ganesh Bubble marker under topical anesthesia in upright position.This instrument gives 3 marks on the limbus at 0, 90 and 180 degrees , extending 2 mm towards the centre of the cornea which are easy to visualize while the eye is being docked. (B)- Method of manual cyclotorsion compensation by a gentle rotation of the cone while holding the same at the attachment of the tube to the cone. (C)-Position of the limbal marks(red arrows) under suction ‘ON’condition without cyclotorsion compensation before starting the laser, showing approximately 12 degrees of cyclotorsion. (D)-Final position of the limbal marks after manual compensation of the cyclotorsion error(alignment with the horizontal axis of the eye piece reticule). Delivery of the laser follows this.
Table 1. Pre-operative baseline characteristics of patients included in the study (n=81 eyes)
Table 2. Visual and refractive results of total (n=81), low cylinder group (n=37), high cylinder group (n=44)eyes.
Table 3. Subgroup analysis of astigmatic correction based on the degree of target-induced astigmatism at 3 months after small incision lenticule extraction (SMILE)for myopic astigmatism
References
- Febbraro JL, Koch D. Detection of static cyclotorsion and compensation for dynamic cyclotorsion in laser in situ keratomileusis, J Cataract Refract Surg 2010; 36:1718–1723 Q 2010.
- Swami AU, Steinert RF, Osborne WE,White AA. Rotational malposition during laser in situ keratomileusis. Am J Ophthalmol 2002;133:561–2.Vogt A. Textbook and Atlas of Slit Lamp Microscopy of the Living Eye. Bonn: Wayenborgh Editions; 1981.
- Arba-Mosquera S, Merayo-Lloves J, de Ortueta D. Clinical effects of pure cyclotorsional errors during refractive surgery. Invest Ophthalmol Vis Sci 2008;49:4828–36.
- Reinstein DZ, Gobbe M, Gobbe L, Archer TJ, Carp GI. Optical Zone Centration Accuracy Using Corneal Fixation-based SMILE Compared to Eye Tracker-based Femtosecond Laser-assisted LASIK for Myopia. J Refract Surg. 2015;31(9):586-92.
- Aslanides IM, Toliou G, Padroni S, Arba Mosquera S, Kolli S. The effect of static cyclotorsion compensation on refractive and visual outcomes using the Schwind Amaris laser platform for the correction of high astigmatism. Cont Lens Anterior Eye. 2011;34(3):114-20.
- Lazaridis A, Droutsas K, Sekundo W. Topographic analysis of the centration of the treatment zone after SMILE for myopia and comparison to FS-LASIK: subjective versus objective alignment. J Refract Surg. 2014;30(10):680-6.
- Kathleen S. Kunert, MD, Christoph Russmann, PhD, Marcus Blum. Vector analysis of myopic astigmatism corrected by femtosecond refractive lenticule extraction. J Cataract Refract Surg 2013; 39:759–769.
- Blum M, Kunert KS, Engelbrecht C, Dawczynski J, Sekundo W. Femtosecond lenticule extraction (FLEx)—Results after 12 months in myopic astigmatism. Klin Monbl Augenheilkd. 2010; 227: 961–965.
- Sekundo W, Kunert KS, Blum M. Small incision corneal refractive surgery using the small incision lenticule extraction (SMILE) procedure for the correction of myopia and myopic astigmatism: results of a 6month prospective study. Br J Ophthalmol. 2011; 95: 335–339.
- Elizabeth P. Shen, MD, Wei-Li Chen, MD, PhD, Fung-Rong Hu, MD .Manual limbal markings versus iris-registration software for correction of myopic astigmatism by laser in situ keratomileusis. J Cataract Refract Surg 2010; 36:431–436
- Alpins NA. A new method of analyzing vectors for changes in astigmatism. J Cataract Refract Surg. 1993;19:524–33.
- Alpins NA. New method of targeting vectors to treat astigmatism. J Cataract Refract Surg. 1997;23:65–75.
- Alpins NA. Vector analysis of astigmatism changes by flattening, steepening, and torque. J Cataract Refract Surg. 1997;23:1503–14.
- Chan TC, Ng AL, Cheng GP, Wang Z, Ye C, Woo VC, et al. Vector analysis of astigmatic correction after small-incision lenticule extraction and femtosecond-assisted LASIK for low to moderate myopic astigmatism. Br J Ophthalmol. 2016;100(4):553-9.
- Zhang J, Wang Y, Wu W, Xu L, Li X, Dou R. Vector analysis of low to moderate astigmatism with small incision lenticule extraction (SMILE): results of a 1-year follow-up. BMC Ophthalmol. 2015;15:8.
- Ivarsen A, Asp S, Hjortdal J. Safety and complications of more than 1500 small-incision lenticule extraction procedures. Ophthalmology. 2014;121:822–8.
- Alpines NA, Goggin M. Practicle astigmatism analysis for refractive outcomes in cataract and refractive surgery. Surv Ophthalmol 2004;49:109-122.
- Febbraro J-L, Aron-Rosa D, Gross M, Aron B, Bre´mond- Gignac D. One year clinical results of photoastigmatic refractive keratectomy for compound myopic astigmatism. J Cataract Refract Surg 1999; 25:911–920
- Cyclotorsion: a possible cause of residual astigmatism in refractive surgery eye motion occurring between wavefront measurement and refractive surgery. J Cataract Refract Surg 2002;28:599–602
- Chernyak DA. Cyclotorsion eye motion occurring between wavefront measurement and refractive surgery. J Cataract Refract Surg 2004; 30:633–638
- KobashiH,KamiyaK,AliMA,IgarashiA,ElewaMEM,ShimizuK.Comparison of Astigmatic Correction after Femtosecond Lenticule Extraction and Small Incision Lenticule Extraction for MyopicAstigmatism. PLoSONE. 2015;10(4):e0123408.
- Miao H, Tian M, Xu Y, Chen Y, Zhou X. Visual Outcomes and Optical Quality After Femtosecond Laser Small Incision Lenticule Extraction: An 18-Month Prospective Study. J Refract Surg. 2015;31(11):726-31.
- Ganesh S, Gupta R. Comparison of visual and refractive outcomes following femtosecond laser- assisted LASIK with SMILE in patients with myopia or myopic astigmatism. J Refract Surg 2014;30:590–6.