Dr. Tanuja
Kate,T09033, Dr. Rajiv Choudhary, Dr. Jyoti
Singhai, Dr. Navita Mittal
Introduction
In the present era of refractive cataract surgery, the goal of astigmatism management is to leave the patient with as little astigmatism as possible. Femtolaser assisted arcuate keratotomy is one of the modalities of astigmatism management. Performing arcuate incisions intraoperatively during cataract surgery is a convenient way to correct astigmatism. Femtosecond laser assisted arcuate incisions have the advantages of being more precise with enhanced reproducibility, improved accuracy & safety and minimal complications.
The purpose of the present study was to find out effect of paired arcuate incisions and opening or not opening them on astigmatism.
Material & Methods
This was a prospective study of 30 cases who had undergone FLACS (LensAR laser with streamline) with paired arcuate incisions during Feb. 2015 to March 2016 at Rajas Eye Hospital, Indore (M.P.), India. All the cases were operated by single surgeon (Dr. Rajiv Choudhary) (IS NAME OF SURGEON REQUIRED?)using the same technique.
The inclusion criteria were:
- Presence of >0.5 D of corneal astigmatism
- Smooth ocular surface
- Good visual potential
The Exclusion criteria were:
Keratoconus, ectatic disorders, corneal scarring and any other ocular pathology.
Under topical anesthesia, the cases were taken for FLACS. The Arcuate incision planning software of LensAR auto populated incision parameters based on the surgeon’s preferences and SIA. Also, this software recommended the placement of laser incisions based on preoperative data. The optical zone was 8 mm, arcuate incision depth was 0.9 and the nomogram used was Woodcock. The written informed consent was obtained prior to surgery. After the laser incisions were made, arcuate wounds were opened in the operating room using a sinskey hook. The Arcuate incisions were opened in 21 cases(Group 1)and not opened in 9 cases(Group 2).
Preoperatively patients underwent comprehensive ophthalmic check up and specifically patient’s Keratometry was recorded. Postoperatively at 1 month follow up, keratometry and Best Corrected Distance Visual Acuity (BCDVA) were recorded. Also, at the same visit, the correction required was also noted.
Observations:
30 cases (Eyes) of 26 patients
Profile in terms of age:
Table 1
| Mean | Standard Deviation | Median | Min. | Max. |
| 61.63 | 9.05 | 60 | 41 | 86 |
Postoperatively what happened to corneal astigmatism magnitude?
Postoperatively what happened to corneal astigmatism magnitude?
Mean corneal astigmatism reduction from preoperative to postoperative
Postoperative correction required in Spherical Equivalent
Data Analysis Table 2
| Mean | Std. Deviation | Median | Minimum | Maximum | N | P Value of Mann-Whitney Test Comparing Group 1 Vs Group 2 | Interpretation | ||
| Preoperative Cylinders Flipped Cylindrical component Preoperative (K1-K2) | Group 1 | 1.15 | .500 | 1.00 | 1 | 2 | 21 | 0.59 | Difference in preoperative cylinders is not statistically significant between the two groups |
| Group 2 | 1.06 | .419 | 1.00 | 1 | 2 | 9 | |||
| Overall arcuate | 1.13 | .472 | 1.00 | 1 | 2 | 30 | Preoperative cylindrical component was similar in both the groups | ||
| Preoperative axis Flipped Axis of astigmatism component Preoperative (higher of the two values of A1 and A2 adjusted for OD and OS) | Group1 | 112.29 | 68.562 | 153.00 | 10 | 180 | 21 | 0.68 | Difference in preoperative axis is not statistically significant between the two groups |
| Group 2 | 101.22 | 68.784 | 90.00 | 5 | 180 | 9 | |||
| Overall arcuate | 108.97 | 67.629 | 135.00 | 5 | 180 | 30 | Preoperative axis was similar in both the groups | ||
| Postoperative Cylinders Flipped Cylindrical component Postoperative (K1-K2) | Group1 | .70 | .387 | .75 | 2 | 21 | 0.11 | Difference in postoperative Cylinders is not statistically significant between the two groups | |
| Group 2 | .82 | .205 | .81 | 1 | 1 | 9 | |||
| Overall arcuate | .74 | .343 | .75 | 2 | 30 | Postoperative Cylindrical Component was similar in both the groups | |||
| Postoperative axis Flipped Axis of astigmatism component Postoperative (higher of the two values of A1 and A2 adjusted for OD and OS) | Group1 | 85.71 | 35.857 | 95.00 | 10 | 160 | 21 | 1 | Difference in postoperative axis is not statistically significant between the two groups |
| Group 2 | 90.56 | 53.236 | 80.00 | 20 | 175 | 9 | |||
| Overall arcuate | 87.17 | 40.910 | 92.50 | 10 | 175 | 30 | Postoperative axis was similar in both the groups | ||
| Surgically Induced Astigmatism Magnitude | Group 1 | 1.6396 | .78016 | 1.4798 | .51 | 3.33 | 21 | 0.68 | Difference in Surgically Induced Astigmatism Magnitude is not statistically significant between the two groups |
| Group 2 | 1.4763 | .60798 | 1.3400 | .51 | 2.46 | 9 | |||
| Overall arcuate | 1.5906 | .72630 | 1.4465 | .51 | 3.33 | 30 | |||
| Surgically Induced Astigmatism axis. (Difference of Axis from theoretical astigmatism induced by a Tilted Lens, 50 in our case) | Group 1 | 84.012 | 33.0824 | 85.000 | 12.3 | 177.5 | 21 | 0.82 | Difference in Surgically Induced Astigmatism axis is not statistically significant between the two groups |
| Group 2 | 95.592 | 45.1723 | 90.052 | 47.0 | 170.0 | 9 | |||
| Overall arcuate | 87.486 | 36.6992 | 86.459 | 12.3 | 177.5 | 30 | |||
| Angle Error refractive astigmatism angle error | Group 1 | 38.109 | 28.0032 | 37.705 | 1.7 | 127.5 | 21 | 1 | Difference in Absolute Angle Error is not statistically significant between the two groups |
| Group 2 | 46.259 | 44.4029 | 40.052 | 1.5 | 120.0 | 9 | |||
| Overall arcuate | 40.554 | 33.1533 | 37.811 | 1.5 | 127.5 | 30 |
Results and statistical analysis
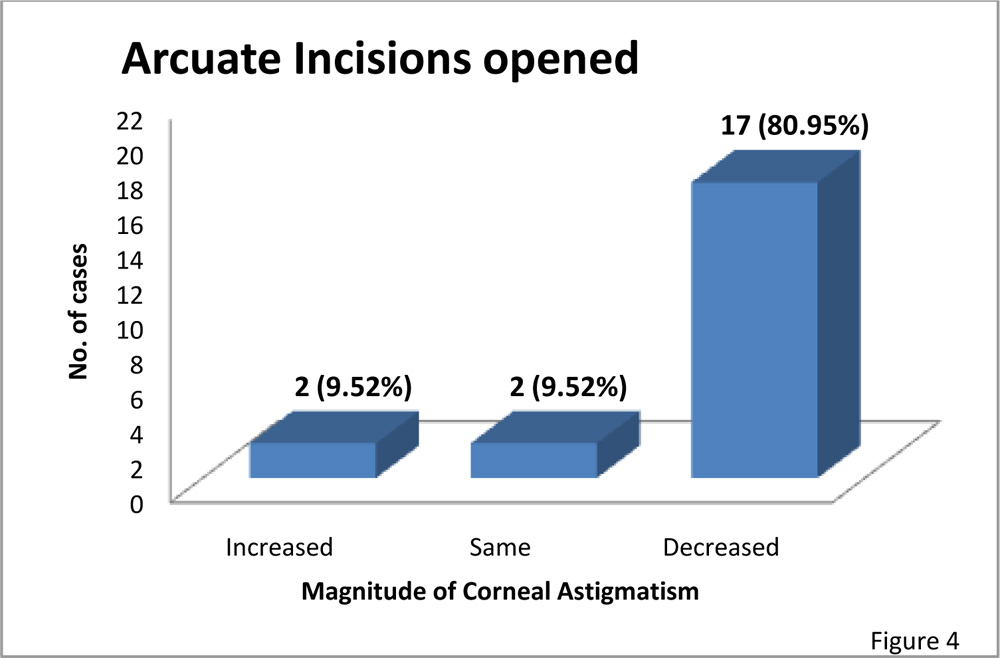
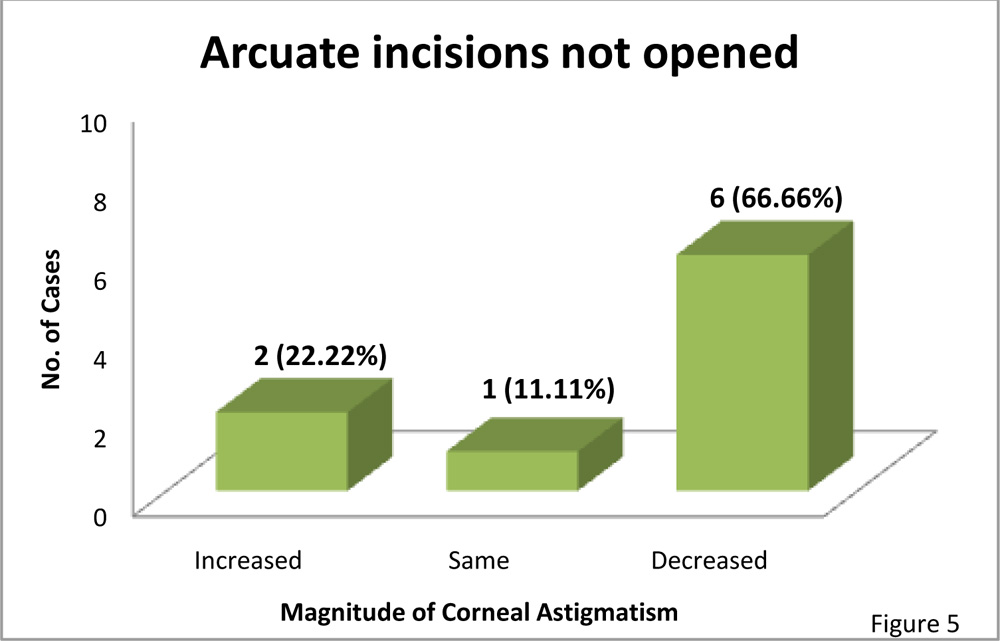
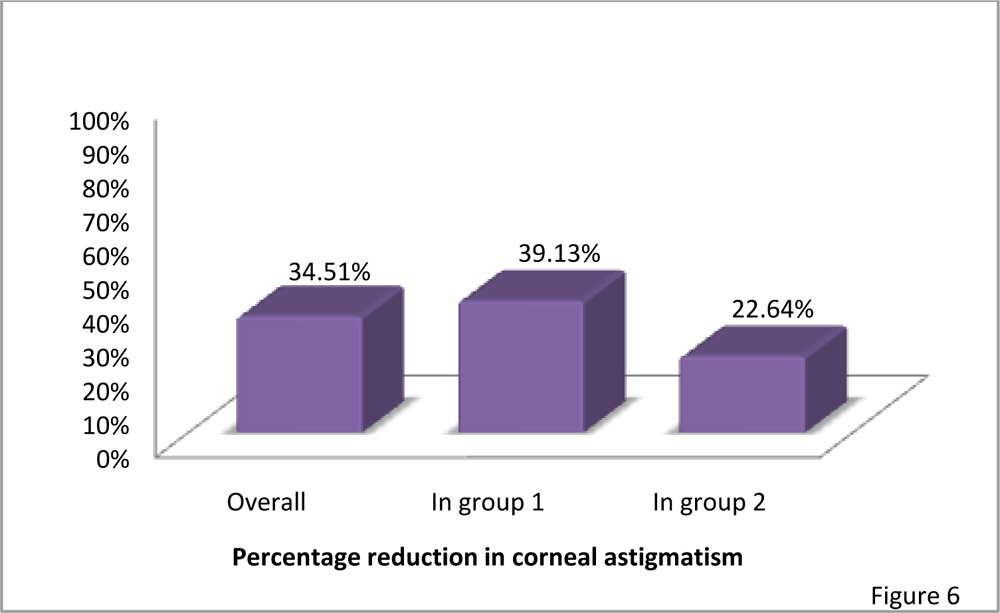
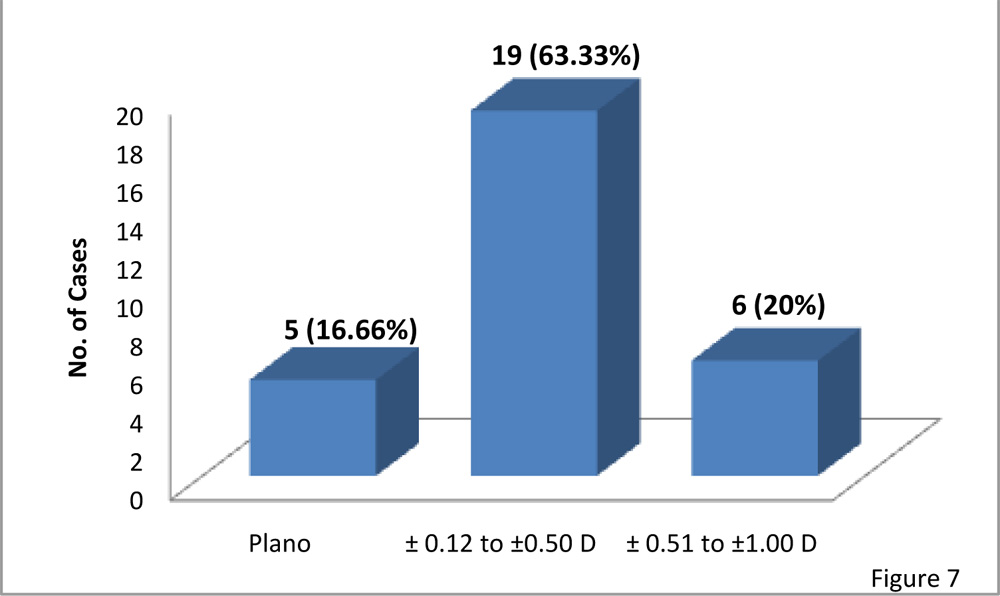
The present study reveals that corneal astigmatism decreased more in cases where arcuate incisions were opened(80.95%)as compared where not opened(66.66%)(Fig.4,5) .Also, the mean corneal astigmatism from preoperative to postoperative decreased by 39.13% in the group with arcuate incisions opened and 22.64% in the one with arcuate incisions not opened(Fig.6).From figure 7,it is inferred that postoperatively correction required in spherical equivalent for distance was nil in 5(16.66%) cases, ± 0.12 to ± 0.50D in 19(63.33%) cases and ± 0.51 to ± 1D in 6(20%) cases.
Data were not normally distributed and hence non-parametric test i.e., Mann Whitney test was used to compare the two groups i.e. group 1 with arcuate incisions opened and group 2 with arcuate incisions not opened. As per table 2 the preoperative cylindrical component, preoperative axis, postoperative cylindrical component & postoperative axis were not statistically significantly different i.e. they were similar in both the groups.
Angle of error is the angle between surgically induced astigmatism and target induced astigmatism vectors. Target induced astigmatism (TIA) vector represents the change by magnitude & axis the surgeon intended to induce. Surgically induced astigmatism means the astigmatic change the surgery actually induced.
In our study, the overall mean angle error was 40.55 while it was 38.10 in group 1 & 46.25 in group 2.Although the angle error was more in the group with Arcuate incision not opened but this difference was not statistically significant.
Discussion
Multiple studies have found Femtosecond assisted laser arcuate keratotomy to have enhanced predictability and a reduced rate of complications (Bahar et al 2008; Hoffart et al 2009).In our study also, we didn’t encounter any complications.
In a study by Yoo A et al the mean preoperative refractive cylinder was 1.71 ± 1.15D which decreased to 0.78 ± 1.06 (P < 0.001). In our study corneal astigmatism reduced from 1.13± 0.47 D to 0.74± 0.34 D. Also, in our study the overall mean cylinder reduction was 34.51%. In cases where arcuate incisions were opened, the reduction was 39.13% and where not opened, the reduction was 22.64%.
Conclusion:
Thus the arcuate incisions reduced corneal astigmatism more in cases where incisions were opened as compared when they were not opened.
References
1.Femtosecond laser assisted intrastromal arcuate keratotomy to reduce corneal astigmatism
J Cataract Refract surg. 2013 Apr; 39(4): 528-38
Ruckl T, Dexl AK, Bachernegg A et al
2.Prevalence of corneal astigmatism before cataract surgery.
J Cataract Refract surgery 2009;35:70-75
Ferrer – Blasco T, Montes-Mico R et al
3.Femtosecond laser assisted arcuate
Keratotomy versus toric IOL implantation for correcting astigmatism.
J Refract Surg. 2015 Sep.; 31(9): 574-8
Yoo A, Yun S et al