Dr.Avadhesh Oli, O13081, Dr. Santosh Kumar, Dr.Dattakiran Joshi
Normal color vision is requirement for usual day to day activities1. Color Perception (CP) assessment is crucial in initial medical assessment of candidates for entry into armed forces. Defective color perception has various grades and no two color blinds are similar2. Defective Red color perception is known as Protanopia when absolute and protanomaly when mild. The visible range of the spectrum is shorter at red. They see the blue, green part of the spectrum as gray. Similarly, defective green vision is called deuteranopia when absolute and deutrenomalia when relative. In this condition, the normal green part appears as gray. Tritanopes have defective blue vision. Color defective people see blue and yellow color more distinctly than red and green and have difficulty in discriminating hue and saturation of colors which adds to confusion in identifying colors. This aspect is used in various tests for defective color vision3.
All the colors can be perceived by the retina by mixing of three primary colors i.e. red, green and blue. The normal color vision is called trichromatic where three cone systems are responsible for red, green and blue colors. Loss of green perception is most common followed by red and blue. Most common congenital dyschromatopsia is a Red-green color deficiency and it remains static.
Color vision defect is a continuous spectrum. The degree of color vision deficiency may vary from mild deficiency to very severe where the patient may not recognize any colors4.
Various methods of color vision assessment are in use. They can be broadly divided into 4 types Pseudoisochromatic plates like Ishihara, Arrangement like Farnsworth D-15, matching tests like anomaloscope and naming tests like Martin Lantern Test or Farnsworth Lantern. Ishihara plates are most commonly used screening method. This test is handy to use and is widely available.
Color vision assessment is an important aspect of the armed forces medical examination. The peculiar job requirements of the correct interpretation of signals in aviation and sailing make this assessment more important5. The Ishihara test is the most important and common screening test at the initial medical examination for the majority of recruits and candidates. In a few specialized entries like aviation and Navy, the color perception is reconfirmed by Martin Lantern Test6.
Ishihara is most commonly used color vision test for screening world over, but the printed books available are of numerous variations from the original. In the market even look alike duplicate versions are available which are very difficult to authenticate. Wear and tear and old faded booklets also pose problems. Incorrect assessment of color perception at initial entry has got remarkable legal and practical problems. Smart phones have created a special place in day to day tasks. Apart from acting as a portable library for data storage various tests can be administered using smart phones. Recently some authors have reported assessment of color vision with Smart phones7. Consequently this study was done to study the utility of Smart phones with electronic Ishihara in assessment of color perception and comparison of results with printed Ishihara charts.
Material & Methods
50 potential subjects were enrolled in this study after taking informed written consent.
Inclusion criteria
- Subjects with defective color vision.
- Subjects willing to be part of the study
- Subjects more than 16 years of age.
Exclusion criteria
- Best Corrected Visual equity less than 6 /6
- Evidence of macular pathology or optic nerve disease
- Patients on drugs with known side effects on color vision
- One eyed or amblyopia
Color Vision Test Equipment
Ishihara Test Booklet 38 plate Chart, 1990 Ed, Carney Howrah and Co, Tokyo Japan
Comprehensive ophthalmology evaluation was done including Snellen’s visual acuity and Slit lamp examination. They underwent Ishihara test under standard testing conditions8.
Ishihara test
The 38 plate pseudoisochromatic chart was used. The guideline followed as per laid down for IP4303 Edition 4 Ed. The timing and the numbers read were recorded. Method of testing
New Ishihara test booklets were used for assessment in day light. The distance for assessment was 75 Cms. Booklet was inclined so that it makes a right angle with line of sight. Day light near a window was used for testing. The subjects were allowed to wear spectacles if they habitually used one, but tinted glasses were strictly not allowed. 3 seconds were given for reading a plate. The subject was not allowed to touch the plates. Random plates were presented to avoid advantage due to the memorizing of charts. Plates 1-25 were used for assessment as all participants were literate. The response was recorded.
Classification of color perception
| 1 | CP II | Able to read all plates except 18-21 as they don’t have any no |
| 2 | CP III | Plates 22-25 are read correctly but some plates are misread |
| 3 | CP IV | Plates 22-25 are also misread |
The scores were noted and Color perception classification was done as followed by Indian Armed Forces.
Subsequently Ishihara test was done by electronic version of eye hand book by American academy of ophthalmology using I Phone 6. Total 16 plates as available were used to classify the color vision defect.
The results were tabulated and analyzed. Kappa values were calculated for agreement between two methods.
Results
Out of fifty subjects tested mean age was 17 years. All were males.Mean visual acuity was 0.1 log MAR but best corrected vision was 0 log MAR (Snellen’s 6/6). No abnormality was detected in ophthalmological or pupillary examination. The results of color vision assessment were as shown in table .
| N 50 | Ishihara booklet | Smart Phone |
| CP II | 42 | 42 |
| CP III | 5 | 7 |
| CP IV | 3 | 1 |
Table 1 Results of two testing modalities
42/50 (84 %) were CP II on Ishihara, they read all similar plates on smart phone also. Overall kappa value 0.85 (p < 0.05) showing good correlation between two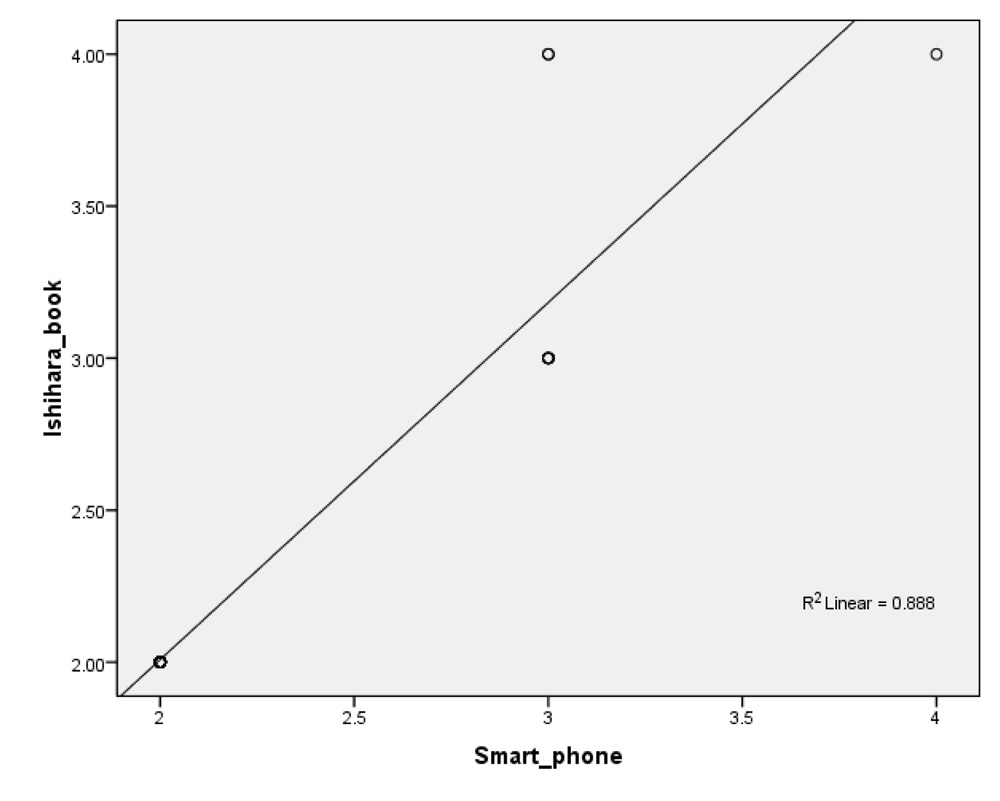 methods.
methods.
On linear regression analysis the values were statistically significant (p<0.05)
A statistically and clinically significant correlation was found between the two methods (Spearman’s rho 0.997, p<0.05) Five candidates were CP III on Ishihara and seven were CP III on smart phone testing. Rest three were CP IV on Ishihara but only one was CP IV on smart phone assessment. On sub group analysis of CP III and CP IV the kappa value was 0.35 (p > 0.05)
This group showed a (Spearman’s rho 0.488, p>0.05) This was statistically not significant.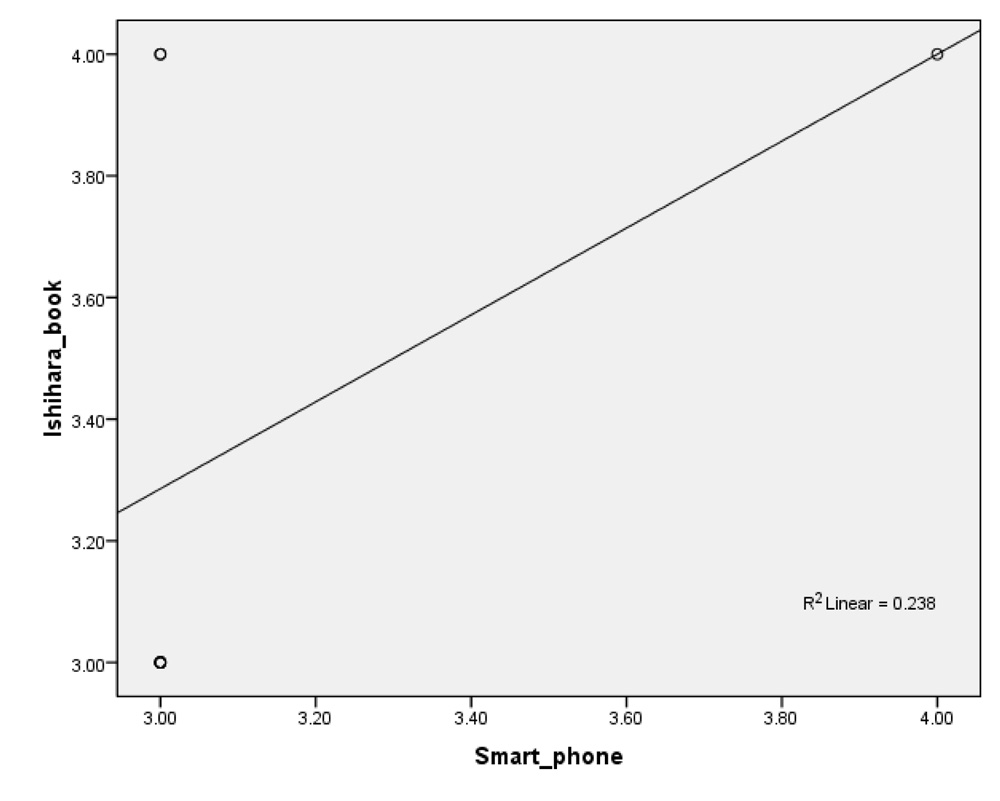
Discussion
This study was done in 50 subjects to compare the results of color vision assessment on printed Ishihara booklets and Smart phone based Ishihara. The mean age of subjects was 19 years. All patients were male, which could be because of typical referral pattern of patients to our center.
Out of total 50 patients 84% were CPII on Ishihara testing. The tests were similar for Smart phone base Ishihara testing also. In a similar study by Campbell et al (2016) good correlation was found between two methods. They studied the utility of this method for patients with optic nerve disorders7. The percentage errors in both the methods were similar. The authors found this method clinically useful in ward settings. Notwithstanding the utility of this method the authors cautioned regarding the standardized version of these apps.
The issue in using mobile devices is the consistency of colors presented. Various models and apps have different luminance. For the purpose of consistency only I Phone 6 with eye book Ishihara was used in this study and was compared with original Ishihara booklet.
The issue of color consistency of various mobile devices was studied by Dain et al (2016). Various models of mobile devices of different manufacturers were studied for consistency of color representation9. The variation was found due to varying technology used by different manufacturers. The back lit LED and panel LED can present different colors. The I phone was found to have 2 times better illuminance. They concluded that with in the same model color vision tests can be designed successfully because the variation of various factors can be controlled.
This study was undertaken to counter the problem of unavailability of original Ishihara booklet for color vision testing. Ishihara booklet is a handy tool to check color vision if it is original. The color of faded original plate due to overuse may give false results. The availability of original Ishihara is further worsened by duplicate and imitated versions which are available for very low cost. The testing of color vision requires high sensitivity and specificity10. The color photocopies of original chart cannot detect defective color perception.
The advantages of this technique are portability, wide availability and standardization if same model of mobile device and app is used.
Smart phone based Ishihara testing was found comparable to printed booklet in testing color vision. It can be used as alternative screening tool.
References
1. Birch J. Worldwide prevalence of red-green color deficiency. J Opt Soc Am A Opt Image Sci Vis 2012;29:313-320.
2. Sheedy JE, Stocker EG. Surrogate color vision by luster discrimination. Am J Optom Physiol Optics 1984;61:495-505.
3. Swarbrick HA, Nguyen P, Nguyen T, Pham P. The ChromaGen contact lens system: colour vision test results and subjective responses. Ophthal Physiol Opt 2001; 21(3):182-196.
4. Richer S, Adams AJ. An experimental test of filteraided dichromatic color discrimination. Am J Optom PhysiolOptics 1984;61:256-264.
5. Welsh KW, Vaughan JA, Rasmussen PG. Aeromedical implications of the X-Chrom lens for improving color vision deficiencies. . Aviat Space Environ Med 1979; 50:249-255.
6. Walsh DV, Robinson J, Jurek GM, Capó-Aponte JE, Riggs DW, Temme LA. A Performance Comparison of Color Vision Tests for Military Screening
Aerosp Med Hum Perform 2016; 87(4):382 – 387.
7. Campbell TG, Lehn A, Blum S, Airey C, Brown H. iPad colour vision apps for dyschromatopsia screening Journal of Clinical Neuroscience 2016;29:92-94.
8. Manual of Medical Examinations and Medical Boards IAP 4303, 4th Ed. In: Delhi AHN, editor; 2010.
9. Dain SJ, Kwan B, Wong L. Consistency of color representation in smart
phones Journal of the Optical Society of America A 2016;33(3).
10. Walsh DV, Robinson J, Jurek GM, Capó-Aponte JE, Riggs DW, Temme LA. A Performance Comparison of Color Vision Tests for Military Screening
Aerosp Med Hum Perform 2016; 87(4):382 – 387.
11. Hodd NB. Putting ChromaGen to the test.Optom Today 1998;38(14):39-42.