Dr. Noornika Khuraijam, K13595, Dr.Sachindra Laishram, Dr. Romen Singh Keisham
Dr. Noornika Khuraijam, MS, DNB, Dr Sachindra Laishram MD, Dr Romen Keisham DNB
Shija Eye Care Foundation, Imphal
Top of Form
Bottom of Form
Introduction
The eyes, are the main points of focus on the face, and contribute immensely towards an individual’s appearance. Enhancing the attractiveness of the eyes can greatly lift a person’s confidence and self esteem.
Asian double eyelid blepharoplasty or surgical creation of a lid crease is the most commonly performed aesthetic procedure in East Asian countries 1, 2
At present it is the most common surgical procedure in South Korea and among the five most common aesthetic surgeries done in New York City in the last two years.
India is home to multiple ethnic communities, and around 40 million of its population has mongoloid or oriental facial characteristics. 3 It is estimated that 50% of people with these features are born without a lid crease.4, 5 Furthermore 50% of those with a pre-existing lid fold have a small or ill defined crease. 5, 6. Therefore an oculoplastic surgeon in India should be familiar with the different anatomical structures that differentiate an oriental eyelid from an Indo Aryan or Caucasian eyelid. This will further help the surgeon in achieving satisfactory results while performing a double Eye lid blepharoplasty.
Surgical eyelid anatomy is typically described in three layers. The anterior most lamella consists of skin and orbicularis oculi, the middle lamella consists of the orbital septum, fat and levator complex, and the posterior lamella consists of the tarsal plate, mullers muscle and conjunctiva.(Figure 1 & 2) The major reason in the anatomy behind the absence of a lid crease as seen in East Asian races, is due to lack of attachments between the fibres of the levator aponeurosis and skin of the eyelid6. In addition presence of excess fat and subcutaneous tissues in the anterior and middle lamella as well as descent of the post septal fat over the tarsal edge may obscure the lid crease. 7 (Figure 1a & 1b) 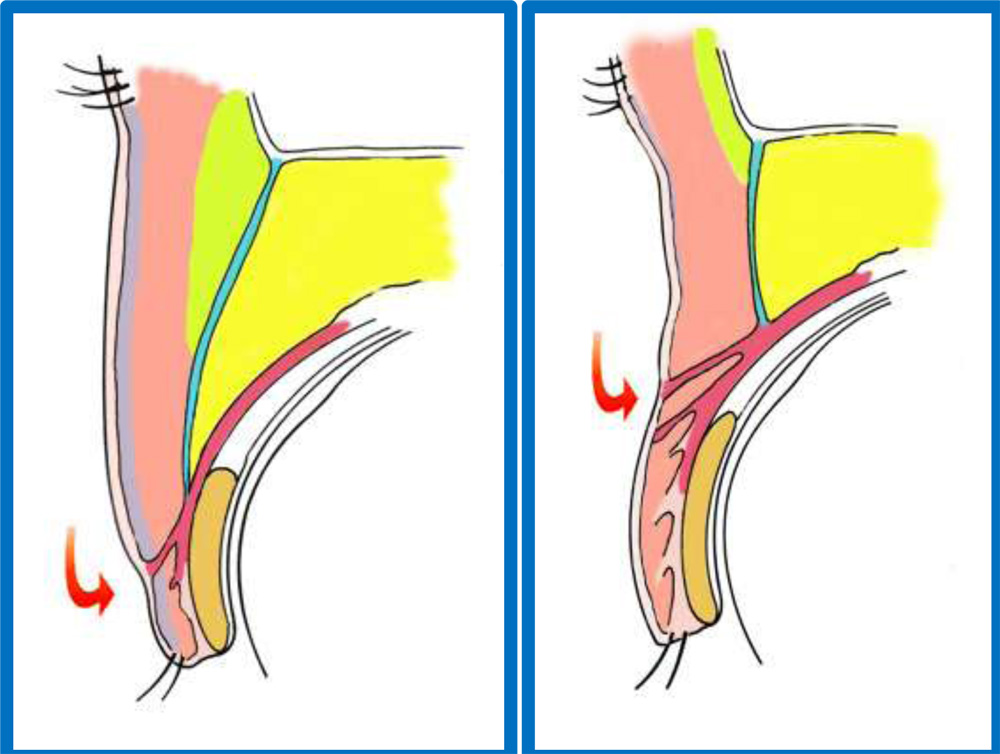
Skin Subcutaneous Fat
Orbicularis Muscle Retro Orbicularis Oculi Fat
Orbital Septum Orbital Fat
Levator Aponeurosis Tarsal Plate
Patients with oriental features who undergo a double eyelid blepharoplasty are often misunderstood as desiring to lose their ethnic appearance. This is not necessarily the reason in most of these cases. 5 An absence of lid crease results in a hooded appearance of the upper eyelid which occludes the root of the lash line. Moreover oriental eyelids tend to have more fat and subcutaneous tissues than those with Caucasian or Indo Aryan features. 8 This results in a dull puffy appearance of the eyes sometimes leading to a pseudoptosis of the upper eye lid. The hooded upper lid skin can also result in epiblepharon causing inversion of the eyelashes. 9 Application of eye makeup also becomes difficult in such cases. Presence of a lid crease results in a brighter more alert look and aids in easy application of eye makeup. (figure3)
Methods
The study includes a total of 84 patients (168 eyes) with typical East Asian eyelid configuration desiring a double eyelid Blepharoplasty, who visited Shija Eye Care Foundation between January 2015 to April 2016. Patients with gross asymmetry of the eyelids, patients who had come for secondary surgery after primary blepharoplasty done elsewhere, and patients with pre-existing ptosis were excluded from the study. All patients were asked to fill a questionnaire at the counselling stage
(figure2). 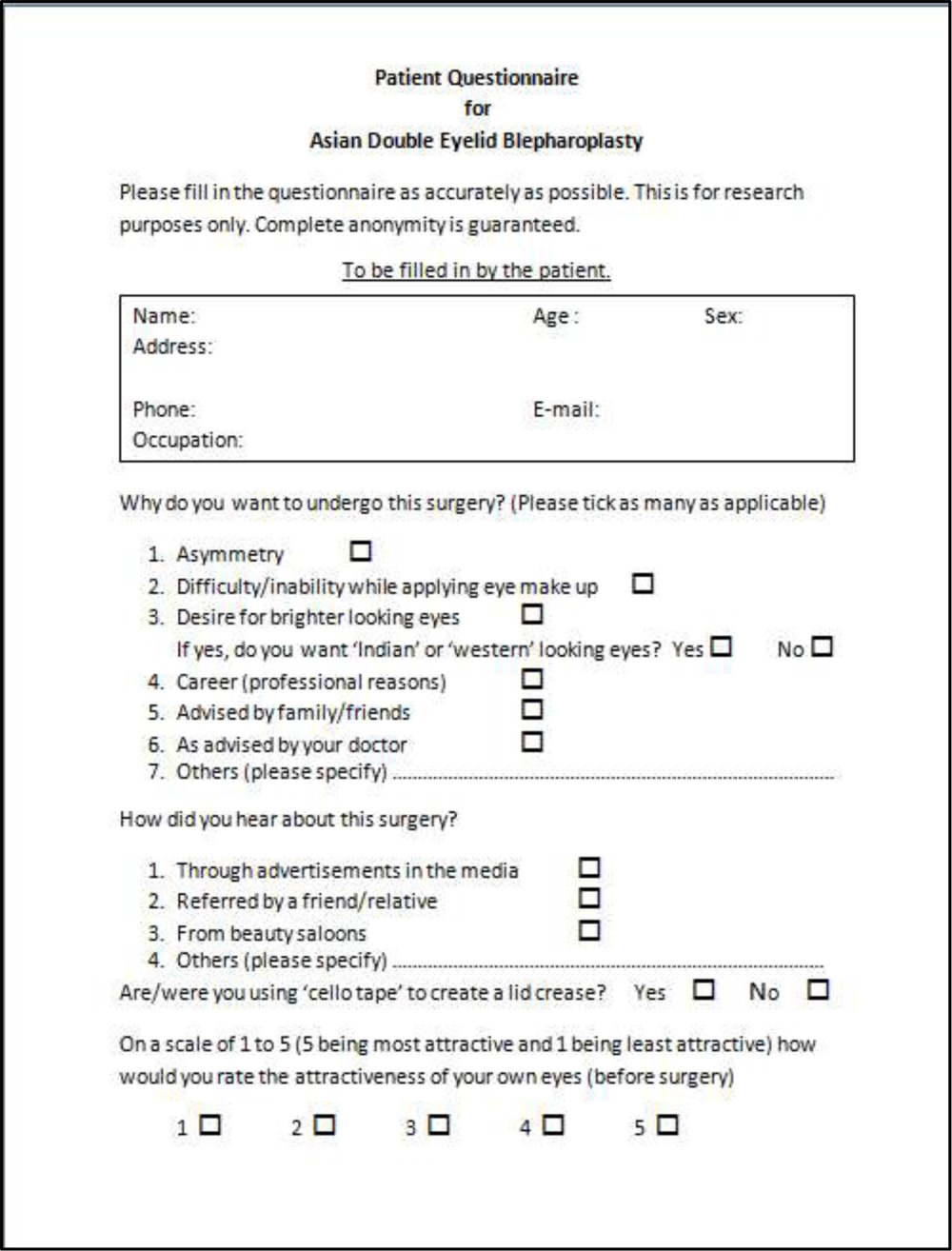
Figure 2: Questionnaire supplied to patients
Patients were informed and counselled about the realistic expectations of the surgery. A temporary lid fold was created with a lacrimal probe to give them an idea about the size, shape and configuration of the lid crease. (Figure 3)
 Figure 3 – creation of a temporary lid fold with the help of a lacrimal probe, showing visibility of eye makeup after creation of lid crease.
Figure 3 – creation of a temporary lid fold with the help of a lacrimal probe, showing visibility of eye makeup after creation of lid crease.
Patients with loose or overhanging skin were noted, as well as those with puffy lids which may indicate presence of excessive fat. Asymmetry if any was also noted. MRD was measured and LPS function assessed to rule out ptosis. Pre-operative photographs were taken in all cases. Routine baseline investigations were done
Surgical Technique
All cases were operated by a single surgeon. After painting and draping, tarsal plate height was measured by everting the upper lid.
 Figure 4- measuring the height of the tarsal plate
Figure 4- measuring the height of the tarsal plate
The area of incision is marked at the maximum height of the tarsal plate ± 1 millimetre. The lid crease is marked ensuring symmetry, regarding its size, shape and height in both eyes. Frontal block supplemented by local infiltration with a solution of lidocaine containing 1:100 000 epinephrine is given in both eyes. Two to three stay sutures are given at the lid margin with the help of 4-0 silk sutures which are then held over a lid spatula and pulled over the eye keeping the skin taut. Incision is given with a 15 number blade. (Figure 5)
 Figure 5: Making the incision
Figure 5: Making the incision
Dissection is then carried out till the tarsal plate exposing the upper edge of the tarsus. Superiorly, the dissection is continued till the septum. Post septal fat if found to be overhanging the upper border of the tarsus is abscised after opening the septum. Care is taken at this stage to not remove excessive orbital fat which can later lead to an unnatural hollowing of the orbital area. Levator Aponeurosis is exposed. Retro orbicularis oculi fat (ROOF) is noted and removed at this stage in patients with preoperative puffy eyelids. A strip of pre tarsal orbicularis oculi is removed to debulk the pretarsal area of the eyelid and also to ensure complete adherence of the pretarsal skin over the tarsal surface. 6-0 prolene sutures are used to anchor the subcuticular tissues to the upper edge of the tarsal plate as well as to the fibres of the levator aponeurosis. 6-0 silk sutures are then used to close the skin over the incision area taking care to take a bite of the upper edge of the tarsus as well as the levator aponeurosis, in at least 3 points. These are done in the central, medial and lateral points of the lids corresponding to the mid pupillary area, the medial limbus and the lateral limbus respectively. Post operatively, ice pack is applied for at least half an hour to the lids in order to minimise oedema and ecchymosis. Patients are prescribed local and systemic antibiotics and anti inflammatory medicines. Suture removal is done at one week. Photographic documentation is done at 1 week, one month, 2 months, and 6 months postoperatively.
 Figure 6: Showing the presence of retro orbicularis oculi fat (arrow)
Figure 6: Showing the presence of retro orbicularis oculi fat (arrow)
Results
Mean age of the study group was 27.02 ± 10.1 years. Minimum age was 15 years and maximum was 65 years. The age group of 20 to 30 years had the maximum number of patients (44 numbers, 52.4%). 85.7% of the patients were females. The male to female ratio was 1:6. 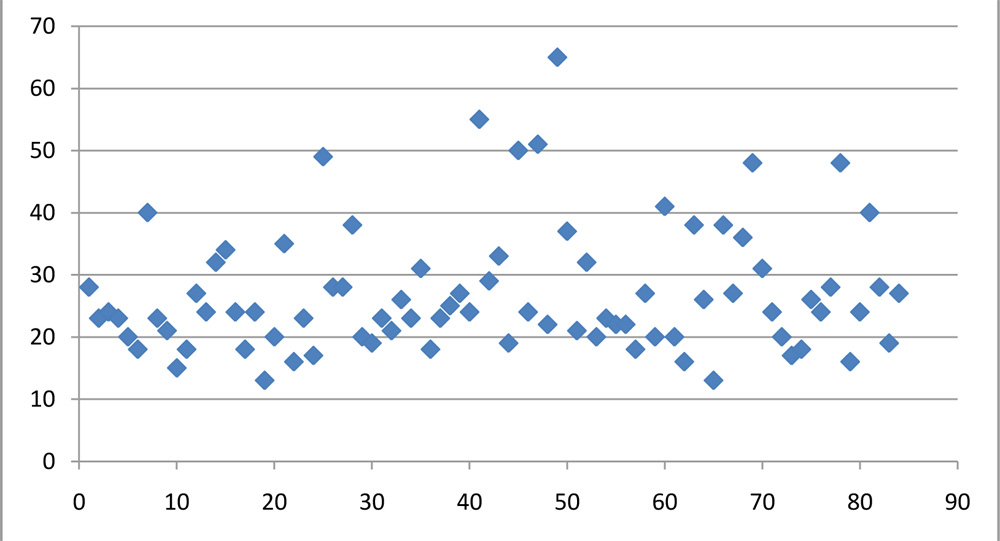 Figure 7: Scatter plot of age
Figure 7: Scatter plot of age
Figure 7: Scatter plot of age
Difficulty in applying eye makeup was the reason cited by 31 patients (37%). The desire for brighter looking eyes was the next most common reason cited (22 patients). Amongst the patients who desired brighter looking eyes, 9 out of 22 wanted eyes that had a Caucasian or Indo Aryan configuration. This accounted for 11% out of the total number of patients that came for surgery. Asymmetry between the two lids was quoted as a reason for undergoing surgery in 14% of the cases. 50% of these, (6 patients) were male. Functional cause for the surgery was 7%. This included foreign body sensation due to associated upper lid epiblepharon in 3 cases, pseudoptosis with overaction of frontalis muscle in 2 cases, and 1 case of field defect due to pseudoptosis.
Cosmetic reasons alone accounted for 77% of the total cases.
Reason for surgery Number of patients Percentage
Asymmetry 12 14
Difficulty in applying makeup 31 37
Desire for brighter looking eyes 22 26
Career purposes 8 9
Functional/advised by doctors 6 7
Advised by family/friends 5 6
Retro orbicularis oculi fat (ROOF) was removed in 52 cases (62%). This could be due to the fact that oriental eyelids have more ROOF than Indo Aryan or Caucasian eyelids. Skin-muscle was excised in 21 (25%) cases. Most of the cases requiring skin-muscle resection were above the age of 35 years. (12 cases out of 14) Post septal fat was removed in 33 cases. (39%)
80 patients (95%) were satisfied with their outcome. 3 patients underwent re-surgery. One patient underwent re-surgery to remove excess skin that covered the lash roots giving an unnatural appearance (Figure 8) and 2 were repeated for asymmetry. In 1 case, the patient was unsatisfied with the outcome due to the prominence of the epicanthal fold that appeared post surgery.
 Figure 8: showing a fold of extra skin covering the lash line, 3 months post operatively.
Figure 8: showing a fold of extra skin covering the lash line, 3 months post operatively.
Conclusion
Asian double eyelid blepharoplasty can be a very effective procedure in the hands of a well informed surgeon. Oriental eyes have particular features, anatomy and variations that make them distinct from the typical Indo Aryan or Caucasian eyes. A detailed understanding of this can greatly aid an oculoplastic surgeon trained in the Indian subcontinent to meet the patient’s expectations. Thorough preoperative discussion regarding the desired end result is necessary to reach a satisfied outcome.
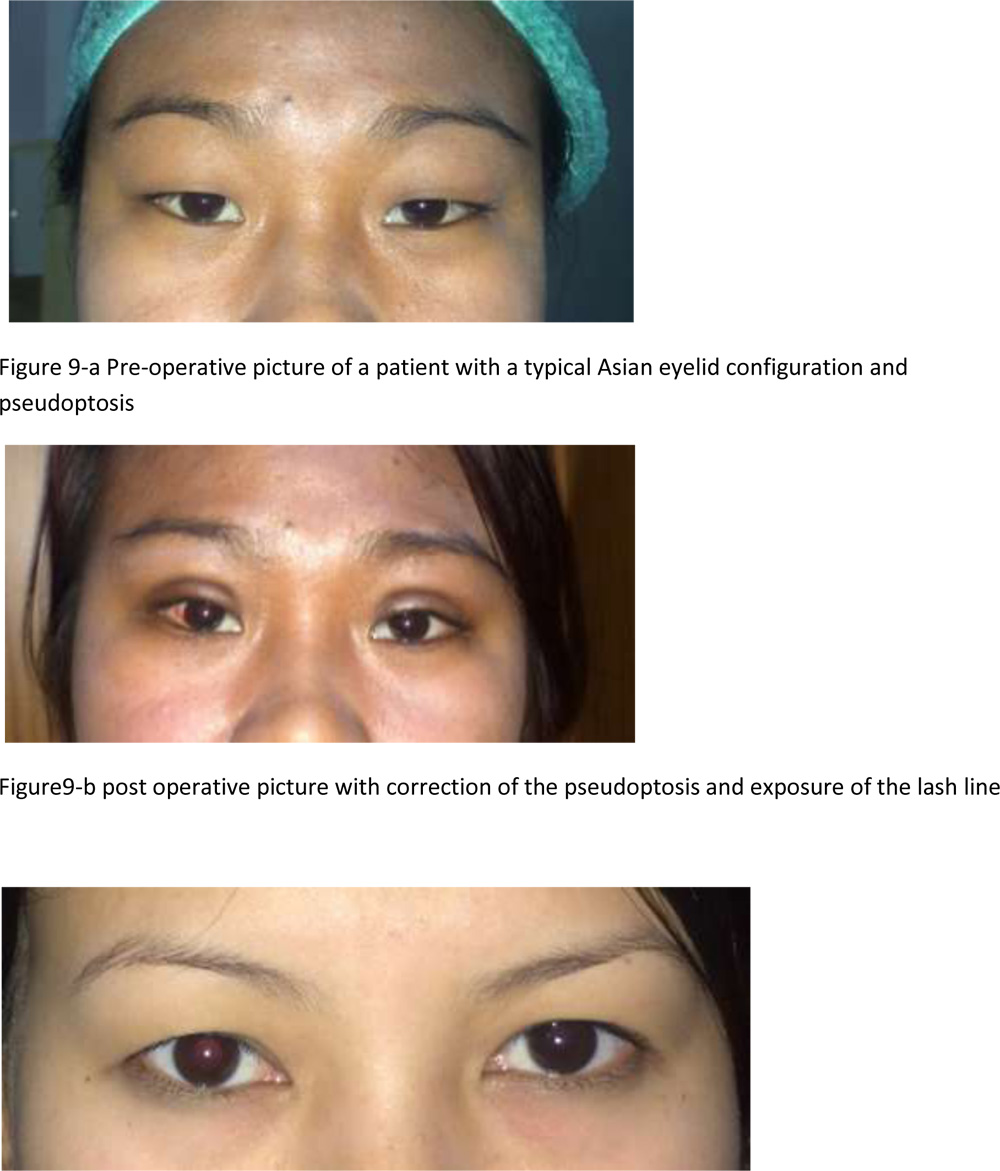 Figure 10-a Preoperative picture of an East Asian eyelid with hooding of upper lid skin which prevents application of eye make up
Figure 10-a Preoperative picture of an East Asian eyelid with hooding of upper lid skin which prevents application of eye make up 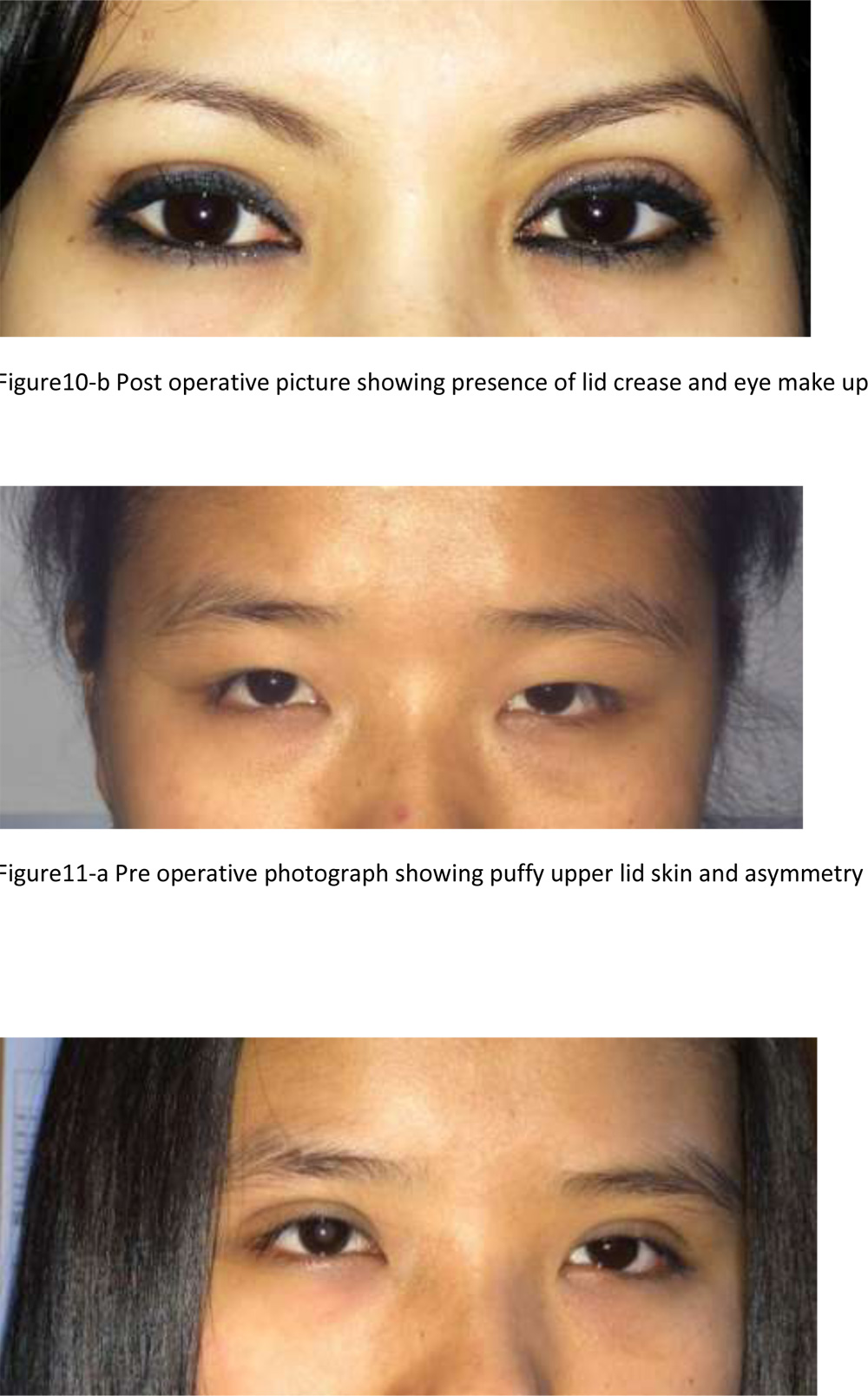 Figure 11-b Post operative photograph at 6 months.
Figure 11-b Post operative photograph at 6 months.
References
1. Chen WPD. Asian Blepharoplasty and the Eyelid Crease. 2nd ed. New York, NY: Elsevier; 2006
2. McCurdy JA. Cosmetic Surgery of the Asian Face. NewYork, NY: Thieme Medical Publishers; 1990
3. http://www.indexmundi.com/india/demographics_profile.html
4. Doxanas MT, Anderson RL. Oriental eyelids. An anatomic study. Arch Ophthalmol1984;102(8):1232–1235
5. Abdulla Fakhro, MD1, Hyung Woo Yim, MD2, Yong Kyu Kim, MD, PhD Anh H. Nguyen, MD. The Evolution of Looks and Expectations of Asian Eyelid and Eye Appearance Semin Plast Surg 2015;29:135–144.
6. Marilyn Q. Nguyen, M.D., Patrick W. Hsu, M.D., and Tue A. Dinh, M.D. Asian Blepharoplasty Semin Plast Surg 2009;23:185–197
7. Kidakorn Kiranantawat, MD, FRCST Jeong Hoon Suhk, MD Anh H. Nguyen, MD The Asian Eyelid; Relevant Anatomy Semin Plast Surg 2015;29:158–164.
8. Jeong S, Lemke BN, Dortzbach RK, Park YG, Kang HK. The Asian upper eyelid: an anatomical study with comparison to the Caucasian eyelid. Arch Ophthalmol 1999;117(7):907–912
9. Noda S, Hayasaka S, Setogawa T. Epiblepharon with inverted eyelashes in Japanese children. I. Incidence and symptoms. Br J Ophthalmol. 1989;73:126–127.