Dr. Rohit Dureja,D19203, Dr. Dipali Parmar
Presenting Author: Dr. Rohit Dureja*
Co Authors: Dr. Dipali Parmar**,Dr. Pradnya Bhole **
INTRODUCTION:
Ocular burns consist of burns to eyelids, conjunctiva, cornea and sclera.
Ocular burns particularly those involving the cornea, are considered a true ophthalmic emergency and require prompt assessment and intervention to minimize morbidity.
PURPOSE:
To evaluate the usefulness of amniotic membrane grafting in acute ocular surface burns.
MATERIALS & METHODS:
A Prospective Study Conducted at M & J Western Regional Institute of Ophthalmology in 30 eyes of 26 patients with acute ocular surface burns (4 bilateral& 22 unilateral )from November 2015 to April 2016.
Inclusion Criteria:
- Patients with ocular surface burns (grade II & onwards): Estimation of ocular burns & classification according to Dua’s classification.
- Cases of ocular burns occurred & presented with in 2 weeks
Exclusion Criteria:
- Lack of timely referral of patients for examinations (>2 weeks on presentation)
Treatment strategy:
Irrigation &/or debridement immediately &estimation of injury & grading as per Dua’s classification.
Wet AMG transplantation was performed within 48 hours of presentation in all the cases with fibrin glue &/or sutures (Within 2 weeks post insult).
All the patients received topical & systemic medication pre & post AMG transplantations as per requirement in individual case.[Medications: topical Antibiotic eye drops(PF), Artificial tear substitutes (PF), Topical steroid preparation(PF)-cases of <10 days of presentation, &/or without melting/perforation, Vitamin C eye drops, Cycloplegic eye drops, IOP lowering agents if indicated. Systemic: Doxycycline (if Not C/I), analgesic/anti-inflammatory medications, Vitamin C supplementation as per recommended dose]
Post-operative assessment for
- Symptoms/signs
{irritation, pain, watering, photophobia, Inflammation/infection}
- Epithelization & healing of ocular surface-Vascularization
- Sequelae/complications-Symblepharon, lid deformities, progressive melting, infection.
Was done on 1stpost-operative day, weekly for 1stmonth, biweekly for the next 2 months & every month thereafter if required.
RESULTS:
Of the 26 patients,
- 21 patients were male(80.76%) and 5 patients were females(19.24%).
- The ratio of male to female was 4.2 : 1
- Age distribution: mean age of patients 28.65 years (Range 2-60 years)
- Paediatric group (2-14 yrs.) 8 cases(30.77%)
- Adult group (15-60yrs) 18 cases(69.23%).
- Unilateral injury -22 (84.62%)
- Bilateral injury- 4(15.38%).
- Of the 4 bilateral injuries, 2 (50%)were due to acids and 2 (50%) due to alkalis.
- Patients with bilateral injuries:3 adults,1 paediatric
- 28 eyes had accidental injury and 2 had homicidal following vitriolage.
- Of all the accidental injuries, 10 eyes had encountered the injury at workplace while the rest 18 eyes at home.
- The average time of presentation post insult was 5.15 days (range-1 to 13 days).
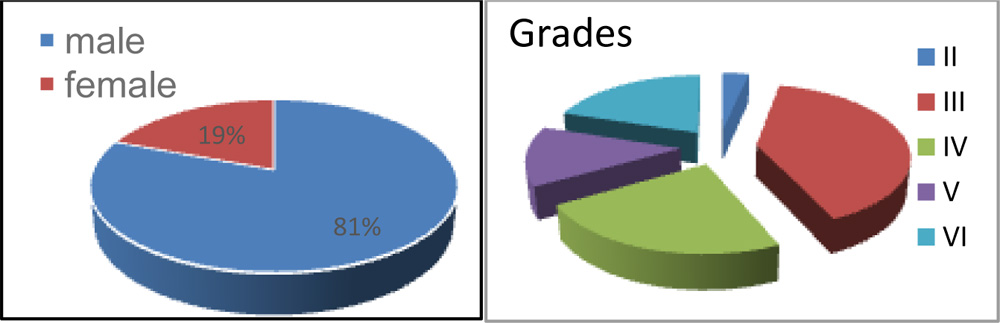 Chart 1. Male: Female – 4.2 : 1 Chart 2. Grade Distribution
Chart 1. Male: Female – 4.2 : 1 Chart 2. Grade Distribution
Grade of the injuries (Dua’s classification)-Of the 30 eyes that presented:
- II = 1 (3.33%)
- III = 12 (40%)
- IV = 7 (23.33%)
- V = 4 (13.34%)
- VI = 6 (20%)
Nature of injury:
- Alkali = 13 (50%)
- Acids = 11(42.30%)
- Thermal = 02(7.70%)
- Total = 26 patients
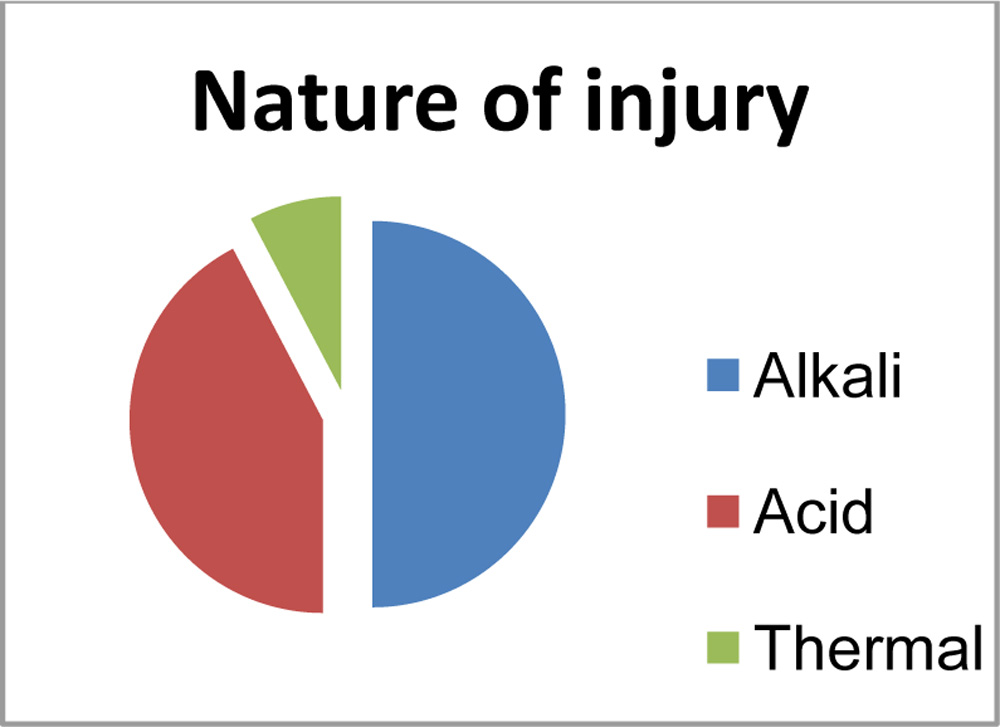 Chart 3. Agents causing ocular burn
Chart 3. Agents causing ocular burn
Around 50% were alkali injuries due to following agents:
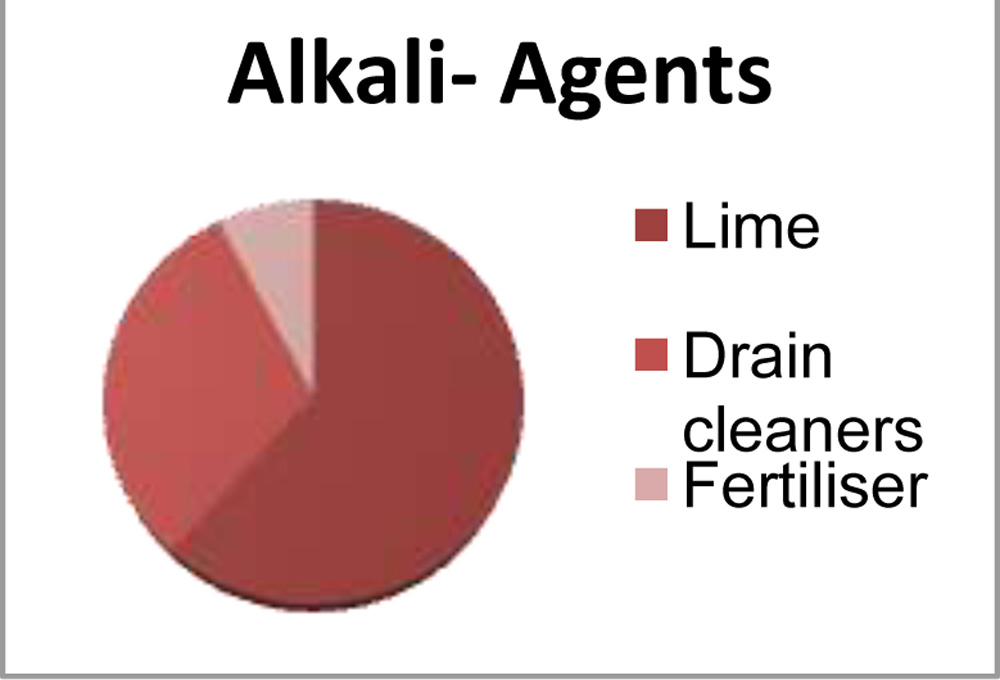 Chart.4. Alkali agents
Chart.4. Alkali agents
• Lime = 08 (61.54%): (The most common etiological agent in our study)
• Drain cleaners(sodium hydroxide) = 04 (30.77%)
• Fertiliser (Ammonia) = 01 (7.69%)
On presentation:
# Melting: 2 cases had melting without perforation (1 thermal injury:3rd day of presentation post insult &1 lime injury :7th day of presentation post insult)
# Perforation:
Of all the 30 eyes, 3 eyes had with perforation due to corneal melting at the time of presentation which necessitated immediate tectonic penetrating keratoplasty.
All of the 3 eyes with perforation presented more than 10 days post ocular injury (mean duration-11 days) and 2 were due to lime injury and 1 was due to acid injury.
# Symblepharon:
Symblepharon was found in 5 eyes (16.67%), all post alkali injury(grade 3 to 6) at the time of presentation.2 eyes had grade 6 injury and 2 eyes had grade 3 injury (8th day & 12th day of presentation post insult) and 1 with grade 5.
The mean duration of presentation was 9.2 days post injury.
# Surgical Intervention:(along with the AMG transplantation)
- AMT was performed within 2 weeks post insult, within 48 hours of presentation to the centre.
- AMT with tarsorraphy was done in 18 eyes with the duration of tarsorraphy ranging from 2 to 8 weeks.
- AMT with tenonplasty was done in 19 eyes.
- There was a need for repeat AMT in 5 cases due to melting/ dislodgement of the AMG.One case needed a total ocular surface AMG due to melting and 2 needed superior fornix reinforcement of AMG while 2 needed inferior fornix reinforcement.
- Debridement was needed in 13 eyes.
- Keratoplasty/patch graft was needed in 3 eyes on presentation (mean duration 11 days)
FOLLOW UP:
The mean follow up period post-surgery was 4.73 months (range= 3 to 6 months).
The following parameters were found on follow up-
# Symptomatic relief:
Notably, pain and discomfort with improvement in symptoms was seen in 27 of the 30 eyes postoperatively.
# Surface re-epithelisation:
Table 1. Surface re-epithelisation Duration : 2 weeks- 8 weeks
| Grade | Average duration of presentation(days) | Average duration of surface re-epithelisation(weeks) |
| II | 3 | 2 |
| III | 5.41 | 4.25 |
| IV | 4.85 | 5 |
| V | 2.75 | 6.5 |
| VI | 7.33 | 7.5 |
Unable to promote surface reconstruction in 3 eyes due to extreme severity of ocular burn.
# Perforation(post AMT):
3 eyes (10%) showed corneal melting post AMT, one in grade 5, two in grade 6 (1 acid injury and 2 alkali injury), progressed to perforation due to corneal melting in spite of AMT, which necessitated full thickness tectonic keratoplasty.
# Infection:
3 eyes of 3 patients with bilateral injury (2 of alkali injury with grade 6 &1 of acid injury with grade 5) had infection during the course of follow up, which finally resulted in visually unsalvageable eyes with failure of visual potential & structural integrity.
# Symblepharon:
Symblepharon was graded as mild, moderate and severe, with or without involvement of the canthi (ankyloblepharon).
Cases of fornix shortening and depth of involvement
- < 25% were graded as mild,
- 25-50% as moderate and
- greater than this as severe.
14 out of 30 eyes developed Symblepharon.
1 eye with grade 3 burn developed severe Symblepharon (>5o% of the inferior deep fornix, lime injury presented after 12th day of injury with inferior corneal melting & perforation).9 eyes developed mild symblepharon (gr3-6).4eyes developed moderate symblepharon (gr5-6).
# Stem cell deficiency:
26 of the 30 eyes (86.67%) showed superficial corneal vascularisation as an indicator of stem cell deficiency. (22 eyes >3 clock hours position & 4 eyes <3 clock hours position)
Table 2. Nature of injury & SCL
| Nature | SCL+ Eyes | Total eyes | SCL+(percentage) |
| Thermal | 2 | 2 | 100% |
| Acid | 10 | 13 | 76.92% |
| Alkali | 14 | 15 | 93.33% |
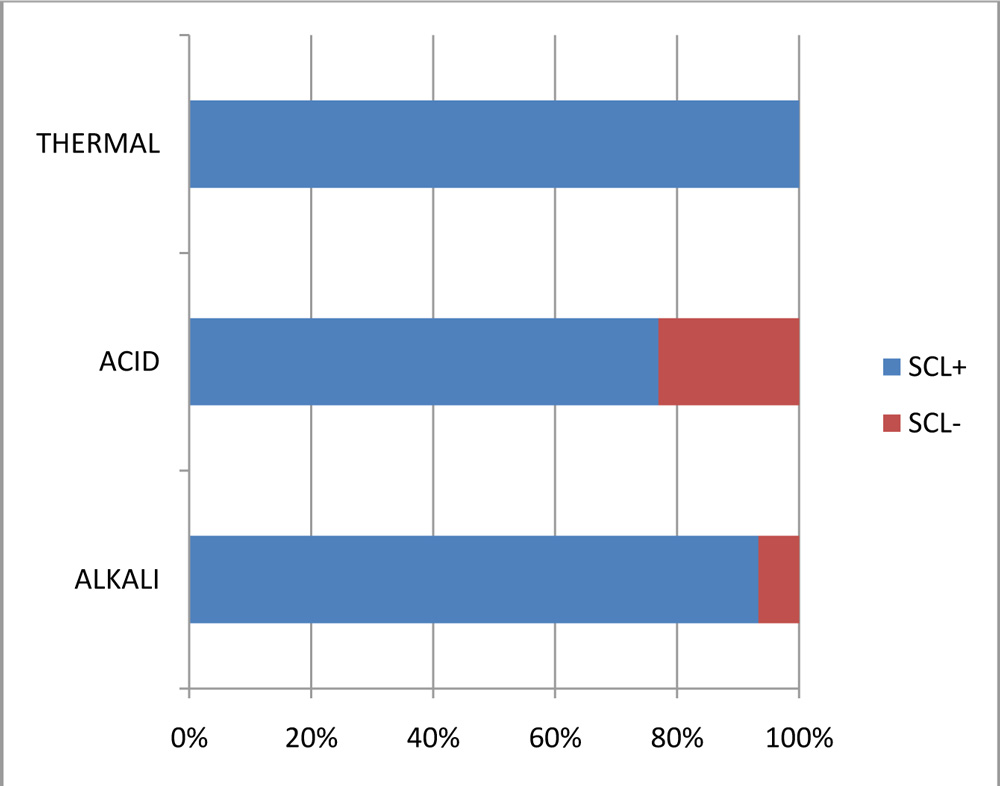 Chart.5. An association between the nature /agent of injury and the presence of stem cell loss (p<0.5).
Chart.5. An association between the nature /agent of injury and the presence of stem cell loss (p<0.5).
Table.3. Involvement of limbal clock position as per grades of injury.
| Grade | SCD >3 to <=6 | SCD >6 to <=9 | SCD>9 to <=12 |
| III | 8 | – | – |
| IV | 4 | 2 | 1 |
| V | – | – | 3 |
| VI | – | 1 | 3 |
DISCUSSUION:
Dua et al reported that in extremely severe burns AMT does not establish the ocular surface or preserve the integrity of the globe.
Meller in his study of 13 eyes with acute ocular burns over a period of 9 month follow up, concluded that in mild to moderate burns, AMT alone rapidly restores both corneal and conjunctival surfaces. In severe burns, however it restores the conjunctival ocular surface without debilitating symblepharonand reduces limbal stromal inflammation, but does not prevent LSCD, which requires further LSCT.
Kobayashi et al reported 5 eyes of 5 pts and concluded that immediate AMG is quite useful for managing moderately severe acute chemical injury by facilitating rapid epithelisation and pain relief and securing ocular surface integrity.
Disadvantages of AMG:
Repeat transplantation & the need for storage & refrigeration of wet AMG.
Limitations of our study:
- Limited follow up period
- Not a comparative study
- Dua’s classification does not classify extent & role of corneal epithelial defect size & limbal staining does not rule out limbal ischemia; so. grading & prognosis needs to be re-evaluated in follow up.
CONCLUSION:
AMG in acute ocular surface injury.
- Useful for relief in symptoms & signs in acute phase-better patient comfort
- Decreases inflammation & promotes surface re-epithelization by providing healthy environment for epithelial cell proliferation & migration- promotes healing.
- Less cicatrisation related ocular surface deformities-Symblepharon, lid malposition, lid closure – future visual rehabilitation procedures less complicated when required.
- Stem cell loss is not being prevented or cured, in severe grades of acute surface burns, leaving integrity of eye still threatened due to ongoing melting process in severe limbal stem cell deficiency cases.
Abbreviations: AMG: amniotic membrane graft, AMT; amniotic membrane transplantation, PF: preservative free, C/I: contraindication, SCL: stem cell loss, SCD: stem cell deficiency)
Financial interest: none
Conflicts of interest: none
Authors: *3rd year Resident,** Assistant Professor at M & J Western Regional Institute of Ophthalmology, Ahmedabad, India.
REFERENCES:
- Kim JC, Tseng SCG. Transplantation of preserved human amniotic membrane for surface reconstruction in severely damaged rabbit corneas.
- Sorsby A, Symons HM. Amniotic membrane grafts in caustic burns of the eye.
- Koizumi N, Inatomi T, Suzuki T. Cultivated corneal epithelial stem cell transplantation in ocular surface disorders.
- Shimazaki J, Yang H-Y, Tsubota K Amniotic membrane transplantation for ocular surface reconstruction in patients with chemical and thermal burns.
- Dua HS, Azuara-Blanco A. Amniotic membrane transplantation.
- Mellor D, Renato TF, Pires, et al. Amniotic membrane transplantation for acute chemical or thermal burns.