Dr. Nisha D.S, N17712, Dr. Vipul Bhandari, Dr. Sri Ganesh,
Dr.Rahul Pandey
Corneal Blindness is the fourth leading cause of Global Blindness after Cataract, Glaucoma and Age related Macular Degeneration. According to the World Health Organization, more than 10 million of the 45 million blind or severely visually impaired people suffer from corneal disease or injury and would benefit from a corneal transplant surgery. If statistics are to be believed, of the 45 million blind people across the world, 15 million live in India.75% of these cases are of avoidable blindness, but due to the nation’s acute shortage of donors, most of these cases go untreated .
On an average, the country needs 200,000 corneas in a year, and only 44,806 are collected. Out of these, only 46% (20,632 eyes) are utilized for sight restoration as the other 54% do not meet the standards for transplantation. As a result, the patient line-up and wait to get a corneal transplant keeps getting longer with each passing day.
Lamellar corneal defects and traumatic microperforations refractory to conventional management remains a challenge to corneal surgeons worldwide. Accepted treatment modalities for such cases are tissue adhesives1, conjunctival flaps2, amniotic membrane graft3, scleral lamellar graft4, corneal patch grafts5 and keratoplasty. The use of a patch graft derived from lenticules extracted from the small incision lenticule extraction (SMILE) procedure as a safe and inexpensive surgical option in the management of microperforations and complicated corneal tears may be a feasible option.
The use of cyanoacrylate glue as a bioadhesive has been reported in ophthalmology since 19636 for sealing corneal perforations7 and attaching methacrylate contact lenses.8 However, it is rarely preferred in current practice due to potential risk of tissue necrosis and high incidence of extrusion when present near the surface.
Fibrin adhesives have been successfully used in pterygium surgeries for attaching amniotic membrane graft or conjunctival autograft ,9 for conjunctival closure following glaucoma surgery10 and strabismus surgery11 and for closure of scleral tunnel after cataract surgery.12 Studies reporting the use of this adhesive for attachment of corneal flaps in de-epithelialized rabbit corneas showed that it was well tolerated, did not cause inflammation, allowed for adherence of the corneal flap, and created an interface that healed after the adhesive disappeared.13,14
Although cyanoacrylate or fibrin glue alone can temporarily seal the partial thickness corneal tear, a secondary surgery is usually required in order to maintain the tectonic integrity of the eye. 5 A corneal patch graft or lamellar keratoplasty would be a permanent solution. However, being a major surgery it requires the use of general or local anesthesia. Moreover, the sutures applied often lead to complications such as postoperative astigmatism, epithelial ingrowth, graft rejection and failure, all in addition to prolonging the surgical time and patient discomfort.
Intra stromal lenticule removal during ReLEx® SMILE (Refractive Lenticule Extraction, Small Incision Lenticule Extraction) for myopic correction and its implantation in allogenic subjects was first reported by Pradhan et al15 for correction of aphakia. Following this report, our research team (Ganesh et al) reported the outcomes with a new technique called FILI (Femtosecond Intrastromal Lenticule Implantation) using cryopreserved ReLEx® SMILE lenticules for potential treatment of hypermetropia and keratoconus.16,17
At our center, ReLEx® SMILE is the main refractive procedure being performed in large numbers for correction of myopia. Thus, the availability of ample amount of lenticule tissue prompted us to use it as patch graft in corneas with microperforations and partial thickness defects as an alternative to currently practiced techniques.
Recently Wu et al published a case series in which they used a SMILE lenticule for sealing corneal perforation18 in 6 patients19 using interrupted sutures to attach the lenticule over the affected area. Though sutures provide stable fixation, they require local anaesthesia, increase surgical time, cause irregular astigmatism and patient discomfort and need subsequent removal at a later date.
Our research team, Bhandari V, Et al. 19 conducted a study, application of the SMILE-Derived Glued Lenticule Patch Graft in Microperforations and Partial-Thickness Corneal Defects in 7 eyes of 7 patients and assessed its short term outcomes. So we decided to carry forward this study to assess its long term clinical and visual outcomes with a larger sample size.
Patients and methods:
25 eyes of 25 patients with partial thickness corneal defects needing a patch graft were included in this study and informed consent was obtained from all patients undergoing the procedure after explaining to them the nature and risks associated with the surgery, in the language they understood. The study was conducted in accordance with the tenets of Declaration of Helsinki.
All donors were healthy individuals between the ages of 20 to 40 years who were scheduled to undergo refractive correction with ReLEx® SMILE for myopia on the same day. Formal informed consent was also obtained from all donors regarding the use of their tissue for a new procedure. Serological tests were conducted on those who consented to donate their lenticules in order to rule out transmissible diseases such as HIV (human immunodeficiency virus), HBsAg (hepatitis B surface antigen), HCV (hepatitis C virus) and syphilis. Preoperatively, all patients underwent detailed slit lamp examination, as well as uncorrected and Corrected distant visual acuity (CDVA) measured by Snellen’s test types. Anterior segment optical coherence tomography (AS-OCT) (Optovue, Fremont, CA) was performed to document the extent of corneal thinning or pathology and to guide us in calculating the lenticule thickness.
Surgical Procedure:
In all the cases, the lenticule was transferred from an adjacent refractive operating room, where ReLEx® SMILE was scheduled. The procedure was planned in advance and availability of donor subjects was ensured. The VisuMax® FS laser system (Carl Zeiss Meditec, Jena, Germany) was used for lenticule creation during the SMILE procedure in the donor cornea for correction of 5-10 D myopia, using a cap thickness of 100 microns, optical zone of 6 mm and a superior 2 mm incision through which the lenticules were extracted by a single and experienced refractive surgeon(S.G.) . The fresh lenticule tissue was immediately and carefully transferred in a sterile petridish containing phosphate buffer solution under strict aseptic conditions. It was ensured that the tissue was used within one hour of extraction in order to minimise the risk of contamination. All lenticule patch graft surgeries were performed by a single experienced cornea surgeon(V.B.) under topical anesthesia of proparacaine eye drops. The recipient bed was debrided carefully using a crescent blade. Excised and debrided tissues were sent for microbiological and histopathological investigations to rule out infection and for confirmation of aetiology wherever indicated.
In patients with microperforations, limbal side port stab entry was made and the anterior chamber formed with air. The lenticule was washed thoroughly with balanced salt solution (BSS) and trephined (or hand fashioned) according to the shape and size of the recipient area. The reconstituted fibrin adhesive was applied to the bed, and the donor lenticule graft was pressed rapidly and firmly against the bed with the help of an atraumatic corneal forceps before the adhesive hardened. A Bandage soft contact lens was applied on all the eyes after surgery and left in place for 7 days
In two patients with severe corneal thinning, two lenticules derived from the same donor were adhered to each other by fibrin glue and this complex was later attached to a thinned out recipient bed.
Postoperative management
Postoperatively, topical Chloramphenicol and Dexamethasone combination eye drops (Dexoren- S, Indico Pharma, India) were used in tapering doses for 1 month and then switched over to topical loteprednol eye drops(Lotepred, Sun Pharma, India) which was tapered over the next 2 months. Subsequently, patients were maintained on loteprednol eye drops once a day for another 3 months.
All patients were followed-up on day 1,7, 15, 1 month, 3 months and 6 months after the surgery. On each postoperative follow-up visit, assessment of corrected distance VA, slit lamp examination to assess graft clarity, digital photography and AS-OCT were carried out. Any complications or adverse effects were also recorded.
Few of the clinical scenarios:
Management of traumatic lamellar corneal tear with secondary fungal infection
The patient presented with a lamellar corneal tear following trauma with a stick. Slit lamp examination showed hanging edematous flap with significant infiltration. Ten percent (10%) KOH mount revealed Aspergillus sp., after which, the patient was started on 5% Natamycin (Natamet, Sun Pharmaceuticals, India) and 0.3% Fluconazole (Zocon, FDC, India) eye drops. Infiltration significantly reduced with treatment, however corneal thinning remained. After one month, a tectonic glued SMILE lenticule patch graft was planned.
Management of severe wound burn following phacoemulsification for brown hard cataract. Figure 1A depicts the pre- operative clinical picture of a patient showing wound burn with corneal thinning following phacoemulsification. AS-OCT showed corneal thickness of 429 μ (fig 1C) at the incision site. Post operatively the graft cleared (fig 1B) and AS-OCT showed improved corneal thickness of 605 μ (fig 1D) at the incision site.
Management of a traumatic central corneal microperforation, unresponsive to conventional management with cyanoacrylate glue and bandage contact lens(Fig 2A). As observed through AS-OCT, central corneal thickness was greatly increased (724μ) (fig 2B) when ompared to a normal peripheral cornea due to cyanoacrylate glue in situ and stromal edema. In this eye, intra-operatively cyanoacrylate glue was carefully removed and patch graft applied as described above. Postoperatively, graft cleared very well(Fig 2C) and AS-OCT showed CCT (Central Corneal Thickness) reduced to 551μ (fig 2D).
Management of corneal degeneration with severe scarring and corneal thinning presented to us. AS-OCT showed corneal thickness of 306µ at the site of lesion. We decided to do a patch graft using to SMILE derived lenticule to fill the defect. Post operatively the graft cleared and AS-OCT showed a thickness of 512 µ.
Management of deeply embedded corneal foreign body, AS-OCT was done to confirm the depth and following the removal of foreign body the defect was sealed with a glued stromal lenticule graft.
Glued stromal lenticule patch graft was also tried in non healing corneal ulcers, corneal degenerations and following corneal melts.
Results
All 25 surgeries were uneventful and patients tolerated the procedure well. On postoperative day 1, mild edema and wrinkling of the graft was seen in 6 cases, which cleared within 1 week. All corneas were completely epithelialized after the removal of bandage contact lens, 1 week after the surgery. In 24 patients the graft was clear and well apposed until the last follow-up time point. 1 patient presented with graft neovascularisation and rejection within the first one month following surgery and was taken up for Anterior Lamellar Keratoplasty. There were no other incidences of graft displacement, aqueous leakage, additional stromalysis, or any clinically detectable opacities or infection post operatively. 20 of the 25 patients showed a significant improvement in their corrected distance visual acuity. However, 3 eyes did not show any change in visual acuity due to underlying glaucomatous damage and 2 patients showed a significant decrease in CDVA post surgery due to secondary Choroidal Detachment and graft rejection.
Table 2 shows the corrected distance visual acuity (CDVA) and comparison of corneal thickness preoperatively and at 3 months and 6 months postoperatively.
Discussion:
Corneal microperforations associated with corneal melting and lamellar corneal tears with corneal thinning must be managed by an emergency tectonic surgery to prevent devastating complications such as endophthalmitis, irido-corneal touch, hypotony with choroidals and subsequent permanent visual loss. Restoring tectonic integrity in these complicated cases poses a challenge to a cornea surgeon. Temporary sealing by cyanoacrylate or fibrin glue with or without amniotic membrane graft does not serve the purpose fully, as the patient invariably requires a secondary permanent procedure in the form of lamellar or full-thickness corneal graft, which is risky and associated with a high rate of immunological rejection and subsequent graft failure. Moreover, constraints of availability, cost, storage and transportation limit the use of fresh and good quality corneal tissues for tectonic purposes.
Various advantages such as lower incidence of dry eye, fewer aberrations, absence of flap related complications, better biomechanical stability and patient comfort have made ReLEx® SMILE, a preferred choice of modern refractive surgeons for correction of myopia and myopic astigmatism. This has led to easy access of good quality corneal lenticules for further use.
Some researchers have shown successful implantation of intrastromal lenticule derived as a by-product of the ReLEx® SMILE procedure for correction of aphakia and hypermetropia.15, 16 Recently Wu et al published a case series in which they used a SMILE lenticule for sealing corneal perforation in 6 patients18 using interrupted sutures to secure the lenticule over the affected area. Though sutures provide stable fixation, they warrant the need for local anaesthetic infiltration, increase the surgical time, cause irregular astigmatism and patient discomfort, and require subsequent removal at a later date.
In our study, fibrin glue was used to secure the lenticule under topical anesthesia, which provided better stability with no incidence of displacement. In almost all cases, the procedure was successful and the patch graft was well taken up by the host cornea. The glued tissue eventually became a part of host cornea with a well epithelised surface, indicating that this treatment could be permanent one.
The issue of transplantation of Lenticule should be treated in lines of a Corneal Transplantation . Hence need for HOTA & following all norms of EBAI must be followed.
REFERENCES :
1.Weiss JL, Williams P, Lindstrom RL, et al. The use of tissue adhesive in corneal 247 perforations. Ophthalmology1983;90:610-615.
2.Izaguirre Roncal LB, Gonzalvo Ibáñez FJ, Pérez Oliván S, et al. [Conjunctival flaps in 249 corneal perforations.] Arch Soc Esp Oftalmol2000;75:825-829. [Article in Spanish]
3.Rodríguez-Ares MT, Touriño R, López-Valladares MJ, et al. Multilayer amniotic membrane transplantation in the treatment of corneal perforations. Cornea2004;23:577-254 583
4.Larsson S. Treatment of perforated corneal ulcer by autoplastic scleral transplantation. Br J Ophthalmol1948;32:54-57.
5.Parmar P, Salman A, Jesudasan CA. Visual outcome and corneal topography after eccentric “shaped” corneal grafts. Cornea2009;28:379-384.
6.Bloomfield S, Barnert AH, Kanter P. The use of Eastman-910 monomer as an adhesive in ocular surgery. II. Effectiveness in closure of limbal wounds in rabbits. Am J Ophthalmol1963;55:946-953.
7.Boruchoff SA, Refojo M, Slansky HH, et al. Clinical applications of adhesives in corneal surgery. Trans Am Acad Ophthalmol Otolaryngol1969;73:499-505.
8.Gasset AR, Kaufman HE. Epikeratoprosthesis. Replacement of superficial cornea by methyl methacrylate. Am J Ophthalmol1968;66:641-645.
9.Kucukerdonmez C, Karalezli A, AAkova Y, et al. Amniotic membrane transplantation using fibrin glue in pterygium surgery: a comparative randomized clinical trial. Eye2010;24:558-566.
10.O’Sullivan F, Dalton R, Rostron CK. Fibrin glue: an alternative method of wound closure in glaucoma surgery. J Glaucoma1996;5:367-70.
11.Biedner B, Rosenthal G. Conjunctival closure in strabismus surgery: Vicryl versus fibrin glue. Ophthalmic Surg Lasers1996;27:967.
12.Kim JC, Bassage SD, Kempski MH, et al. Evaluation of tissue adhesives in closure of scleral tunnel incisions. J Cataract Refract Surg1995;21:320-325.
13.Ibrahim-Elzembely HA, Kaufman SC, Kaufman HE. Human fibrin tissue glue for corneal lamellar adhesion in rabbits: a preliminary study. Cornea2003;22:735-739.
14.Cho SY, Kim MS, Oh SJ, et al. Comparison of synthetic glues and 10-0 nylon in rabbit lamellar keratoplasty. Cornea2013;32:1265-1268.
15.Pradhan KR, Reinstein DZ, Carp GI, et al. Femtosecond laser-assisted keyhole endokeratophakia: correction of hyperopia by implantation of an allogeneic lenticule obtained by SMILE from a myopic donor. J Refract Surg2013;29:777-782. 280
16.Ganesh S, Brar S, Rao PA. Cryopreservation of extracted corneal lenticules after small 281 incision lenticule extraction for potential use in human subjects. Cornea2014;33:1355- 1362.
17.Ganesh S, Brar S. Femtosecond Intrastromal Lenticular Implantation Combined With Accelerated Collagen Cross-Linking for the Treatment of Keratoconus – Initial Clinical Result in 6 Eyes. Cornea2015;34:1331-1339.
18.Wu F, Jin X, Xu Y, et al. Treatment of corneal perforation with lenticules from small incision lenticule extraction surgery: a preliminary study of 6 patients. 292 Cornea2015;34:658-663.
19.Cornea: March 2016 – Volume 35 – Issue 3 – p 408–412 Application of the SMILE-Derived Glued Lenticule Patch Graft in Microperforations and Partial-Thickness Corneal Defects Bhandari, Vipul DOMS, DNB; Ganesh, Sri MS, DNB; Brar, Sheetal MS; Pandey, Rahul M.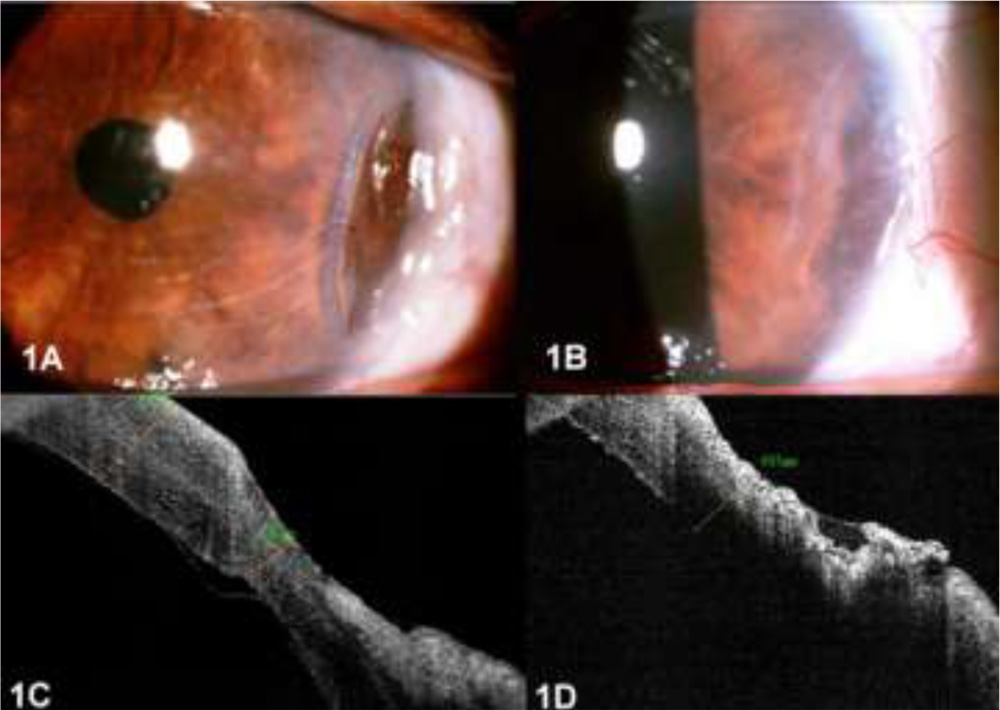
Figure 1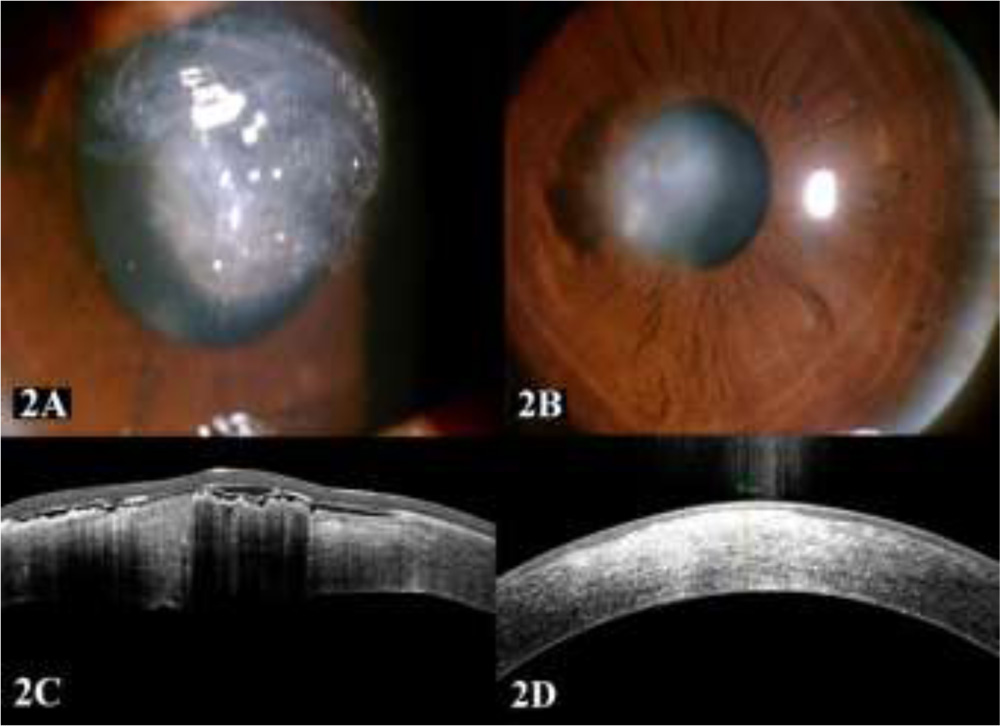
Figure 2
| Serial No. | AGE/
SEX |
CDVA | INDICATION | PAST HISTORY | HISTO PATHOLOGY | PRE OP AS-OCT |
| 1 | 16/F | 6/9 | Lamellar tear | Trauma | Tissue necrosis with no active infection | 510 |
| 2 | 26/M | CFCF | Microperforation | Trauma | Tissue necrosis with no active infection | 724 |
| 3 | 28/M | 6/36 | Lamellar tear | Trauma | Tissue necrosis with no active infection | 486 |
| 4 | 60/F | 6/12 | Wound burn with microperforation | Phacoemulsification surgery | Tissue necrosis with no active infection | 429 |
| 5 | 36/F
|
6/18 | Microperforation | PUK | Tissue necrosis with no active infection | 465 |
| 6 | 79/F | 6/24 | Partial thickness defect | Corneal Degeneration | Tissue necrosis with no active infection | 306 |
| 7 | 46/M | 6/18 | Partial thickness defect | Healed TB ulcer | Tissue necrosis with no active infection | 368 |
| 8 | 64/M | CF 0.5M | Microperforation | Corneal melt | Tissue necrosis with no active infection | 473 |
| 9 | 73/M | 6/18 | Microperforation | Corneal degeneration with thinning | Tissue necrosis with no active infection | 462 |
| 10 | 37/M | 6/24 | Partial thickness defect | Deep stromal FB | Tissue necrosis | 120µ deep |
Table 1: Demographic and clinical details of few patients
| Serial No. | Pre Operative Pachymetry (µ)(AS-OCT) | Lenticule thickness used
(µ) |
6months Post Operatively | |
| Pachymetry
(µ) |
CDVA | |||
| 1 | 510 | 131 | 746 | 6/9 |
| 2 | 724 | 146 | 551 | 6/18 |
| 3 | 486 | 118 | 571 | 6/15 |
| 4 | 429 | 142 | 603 | 6/12 |
| 5 | 465 | 103 | 546 | 6/9 |
| 6 | 306 | 133+124 | 512 | 6/12 |
| 7 | 368 | 124+120 | 574 | 6/12 |
| 8 | 473 | 112 | 566 | CF 1m |
| 9 | 462 | 129 | 636 | 6/18 |
| 10 | 120µ deep | 137 | 521 | 6/9 |
Table 2: CDVA and pre op and post op corneal thickness