Dr. Shreyas Ramamurthy, R14399, Dr. Chitra Ramamurthy
Abstract:
Puprose:
To compare efficacy, refractive accuracy & safety of combining PRK with CXL to standard PRK.
Methods:
Retrospective comparative interventional study. For PRK with CXL (Group A), eyes with borderline suspicious tomography or low pachymetry (<475μ) were included. Age and spherical equivalent matched eyes with normal tomography and pachymetry were taken up for standard PRK(Group B). Group A underwent accelerated crosslinking 30mW/cm2 for 90 seconds. Minimum follow up was 6 months.
Results:
150 eyes were included with 75 eyes in each group. The mean spherical equivalent was -3.57D in Group A and -3.42D in Group B. Group A had significantly higher eyes with low pachymetry(p<0.01). 100% in Group A & 98% in group B maintained BCVA. The mean residual spherical equivalent was 0.62D & 0.35D respectively. No difference in significant haze or contrast sensitivity was noted.
Conclusion:Combining crosslinking with PRK in suspicious tomographies augurs for safe and predictable outcomes.
Introduction:
Iatrogenic Ectasia and Myopic Regression are two well recognized complications following ablative keratorefractive surgery both of which occur in part due to the biomechanical weakening of the cornea post refractive surgery1. Collagen Cross linking has become the mainstay of treatment to arrest progression of both keratoconus and iatrogenic ectasia by enhancing corneal rigidity2. The concept of using prophylactic cross linking in combination with LASIK has been used to reduce the incidence of regression and possibly ectasia3-5. In our study we have compared the safety and efficacy of PRK alone versus PRK combined with cross linking in eyes with borderline pachymetry and borderline topography.
Materials & Methods:
The study was a comparative retrospective interventional study conducted at the Refractive Services of The Eye Foundation, Coimbatore, India. All patients underwent detailed anterior and posterior segment examination, a corneal tomography was performed using Oculus Pentacam Scheimpflug imaging. Patients who had pachymetry of > 475u but less than 500u and no suspicious red flag signs on tomography were considered suitable candidates for PRK alone. Patient having pachymetry in the range of 450-475u and/or having subtle red flag signs on tomography (mild Inferior superior asymmetry; Overall D of Pentacam being RED) not amounting to forme fruste or subclinical keratconus were included in the PRK with CXL group.
The excimer laser ablation was performed using the Wavelight Allegretto EX 500 system. The epithelial removal in all patients was done using the PTK mode using a preset depth of 50u.
Subsequent to excimer ablation, subjects in the PRK group underwent Mitomycin C 0.02% application for 30 seconds. In the PRK with CXL group, No mitomycin C was applied. Instead a 90 second soak using 0.25% riboflavin was performed, and then followed up with a 90 second irradtiaion with 30 mW/cm2 to give a total fluence of 2.7 J, using the Avedro KXL cross linking system. No adjustment in the excimer ablation nomogram was done for the PRK Xtra group.
The primary outcome measure was uncorrected visual acuity at 6 months follow up. The secondary outcome measures included corneal haze and Residual Error/Regression. All data was entered into Microsoft Excel 2010 and analysed using SPSS software. Student t test was used for parametric date and Chi square test was used for non parametric data. A p value of <0.05 was considered statistically significant.
Results:
A total of 150 eyes were included in the study with 75 eyes in each group. The mean age in the PRK Xtra (Group A) and PRK group (Group B) was 24.7 & 24.9 respectively. The Mean Pre op spherical equivalent was -3.57D in Group A and -3.42 in Group B. The patients with a pre op spherical equivalent of >-3D was 47 in group A and 43 in the PRK group.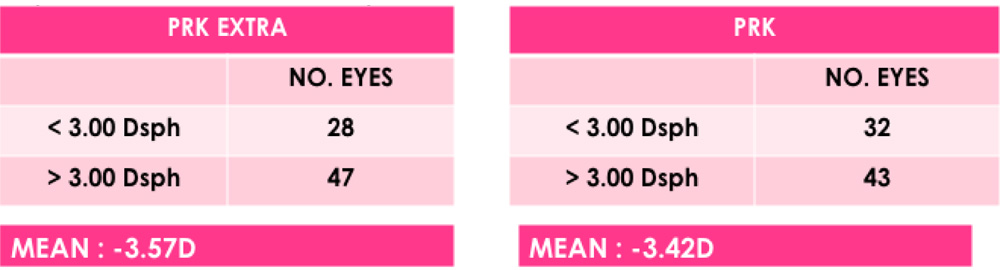
The mean preoperative central corneal thickness was 482.32μ in the PRK Xtra and 486.39μin the PRK group. But notably 28 eyes in the PRK Xtra group had a pachymetry between 450-475μ as compared to none in the PRK group. Of the remaining 47 eyes in the PRK Xtra group, all of them had tomographic abnormalities with Overall D being yellow in 17 eyes and red in 30 eyes.
Post operatively an uncorrected visual acuity of 20/20 was achieved in 67 eyes (89.3%) In Group A& in 70 eyes(93%) in Group B. This difference was not statistically significant. (p = 0.23). Contrast sensitivity measured both in photopic and mesopic conditions did not reveal any difference between the two groups.
8 eyes had a residual error in Group A ranging from -0.25D to -1.5D with a mean of -0.63D. No patient had any overcorrection in Group A in 6 months post op follow up period. In Group B, 5 eyes had a residual error ranging from +0.25 D to -0.75D with a mean of -0.33D.
No major complications like infection or reduction in BCVA was seen in either group. 9 eyes developed Grade 1 superficial corneal haze in Group A which resolved in 6 months time. It was of note that all patients who developed haze in Group A had a pre op spherical equivalent of >3D with a mean of -4.4D.
Discussion:
Keratorefractive surgeries reduce the biomechanical strength of the cornea both due to flap creation as well as due to ablation9. The beneficial effect of cross linking in preventing progression in Keratoconus and causing an increase in biomechanical rigidity of the cornea has been well established2. The safety and efficacy of combining a partial surface ablation with cross linking in keratoconic eyes using the Athens protocol has been proven in multiple studies6-8. Recently cross linking has been combined with laser vision correction in high myopic and hyperopic eyes to reduce the incidence of regression4,10,11.
In this study we have analysed the safety and efficacy of combining accelerated crosslinking with standard PRK in eyes with lower pachymetry (between 450-475u) and in eyes with borderline topographies but those which do not fall into the category of subclinical or formefruste Keratconus. The concept of using additional cross linking along with surface ablation in these eyes was to compensate for the biomechanical weakening caused by the excimer ablation and reduce the risk of ectasia and regression in these borderline corneas.
The concern behind combining crosslinking along with regular laser correction is that whether the cross linking will cause subsequent flattening leading to overcorrections and if the possible haze caused by cross linking could lead to drop in best corrected visual acuity. The advent of accelerated cross linking has enabled us to use faster protocols which increase biomechanical rigidity but at the same time do not cause the same flattening as the conventional protocol12.
In our study we used accelerated cross linking with a high irradiance of 30mw/cm2 for a period of 90 seconds delivering a total fluence of 2.7J/cm2. This protocol has been used previously along with LASIK in eyes undergoing correction for high myopia and hyperopia3,10.
We found a similar safety and efficacy profile between the groups undergoing cross linking and surface ablation as compared to eyes undergoing only surface ablation which were matched for age and spherical equivalent. There was no correction or adjustment which was made in the excimer laser algorithm for PRK Xtra group to account for the cross linking. Similar studies which have combined crosslinking with laser in-situ Keratomileusis did not have any corrections made to the laser algorithms for both myopic and hyperopic refractive corrections4,10,11. No progressive overcorrections were seen in the cross linked group over a period of 6 months and none of the patients lost any lines of best corrected visual acuity. This showed that the crosslinking in this dosage and application did not require any undercorrections or adjustment in the excimer laser nomogram.
In the group undergoing crosslinking with PRK, Mitomycin C was not used. This was to see whether the cross linking itself which causes apoptosis of the keratocytes in the anterior stroma may reduce the incidence of anterior stromal haze. 9 eyes however did develop a Grade 1 haze which resolved within the first 6 months and all eyes had a BCVA of 20/20. The haze was also seen in eyes undergoing higher myopic corrections. Although the minimal haze did not affect the visual outcome in our series, we recommend the use of 0.02% Mitomycin C even when the laser correction is being combined with cross linking in this accelerated half fluence mode, as it is likely that the amount of apoptosis caused by this form of cross linking may not be sufficient to prevent haze formation.
This study had all the limitations of a retrospective study. We did not perform aberrometry in all patients in the post op period and therefore an effective comparison of higher order aberrations between the two groups could not be made. Another limitation was that anterior segment optical coherence tomography (AS-OCT) was not performed to look for the demarcation line if any.
Conclusion:
This study was able to establish the efficacy & safety of combining accelerated cross linking along with standard PRK in eyes with borderline pachymetry and in eyes with subtle abnormalities on corneal tomography which do not characterize subclinical or formefruste keratconus. The addition of cross linking to such corneas could help maintain biomechanical stability after excimer ablation. Long term results are awaited to establish the efficacy of this protocol.
Refrerences:
- Post-laser in-situ keratomileusis ectasia: current understanding and future directions. Randlemann J. Current Opinion in Ophthalmology 2006, 17:406–412.
- Corneal Cross Linking. Randlemann J, Khandelwal S, Hafezi F. Survey of Ophthalmology. 60; 2015; 509-523.
- Predictable visual outcomes with accelerated corneal cross-linking concurrent with laser in situ keratomileusis. Kanellopoulos AJ, Tamayo GE. J Cataract Refract Surg. 2012;38(12):2206-08.
- Adjuvant corneal crosslinking to prevent hyperopic LASIK regression. Aslanides IM, Mukherjee AN. Clinical ophthalmology (Auckland, N.Z.). 2013;7:637–41.
- Accelerated corneal crosslinking concurrent with laser in situ keratomileusis. Celik HU, Alagöz N, Yildirim Y, et al. J Cataract Refract Surg. 2012;38(8):1424–31.
- Keratoconus management: long-term stability of topography-guided normalization combined with high-fluence CXL stabilization (the Athens protocol). Asimellis G, Kanellopoulos AJ. J Refract Surg. 2014;30:88-93.
- Simultaneous topography-guided PRK followed by corneal collagen cross-linking for keratoconus. Kymionis GD, Kontadakis GA, Kounis GA, et al. J Refract Surg. 2009;25:S807-S811.
- Comparison of sequential vs same-day simultaneous collagen cross-linking and topography-guided PRK for treatment of keratoconus. Kanellopoulos AJ. J Refract Surg. 2009;25:S812-S818
- Postoperative changes in intraocular pressure and corneal biomechanical metrics Laser in situ keratomileusis versus laser-assisted subepithelial keratectomy. Qazi MA, Sanderson JP, Mahmoud AM, Yoon EY, Roberts CJ, Pepose JS. J Cataract Refract Surg. 2009 Oct;35(10):1774-88.
- In vivo confocal laser microscopy of morphologic changes after simultaneous LASIK and accelerated collagen crosslinking for myopia: One-year results. Tomita M, Yoshida Y, Yamamoto Y, Mita M, Waring G. J Cataract Refract Surg 2014; 40:981–5.
- Comparison of prophylactic higher fluence corneal cross-linking to control, in myopic LASIK, one year results.Kanellopoulos AJ,George A,Karabatsas C. Clinical Ophthalmology 2014:8 2373–2381.
- Current Protocols of Corneal Collagen Cross-Linking: Visual, Refractive, and Tomographic Outcomes. Shetty R,Pahuja N et al. Am J Ophthalmol 2015;160(2): 243–249.