Dr. Amarendra Deka, D10525
Introduction
Public health in India is a strange paradox. Because 70% of health resources are located in urban area where 30% population lives whereas less than 30% health resources are located in rural area where 70% of the population lives(Review of health care in India).
Due to absence of quality primary healthcare and low awareness among poor on availing such care, they are availing care from dubious sources or foregoing care leading to rise in morbidity and mortality in the rural community (Ibid).
Present Facts
- 4 million blind children in the world.
- Every minute, somewhere in the world, a child goes blind and nearly half a million children develop blindness each year.
- Ninety per cent of blind children die before reaching adulthood (usually from malnutrition).
- It has been estimated that nearly a third of the global economic cost of blindness is due to childhood blindness
- About 45 per cent of blindness in these children could have been prevented or treated.
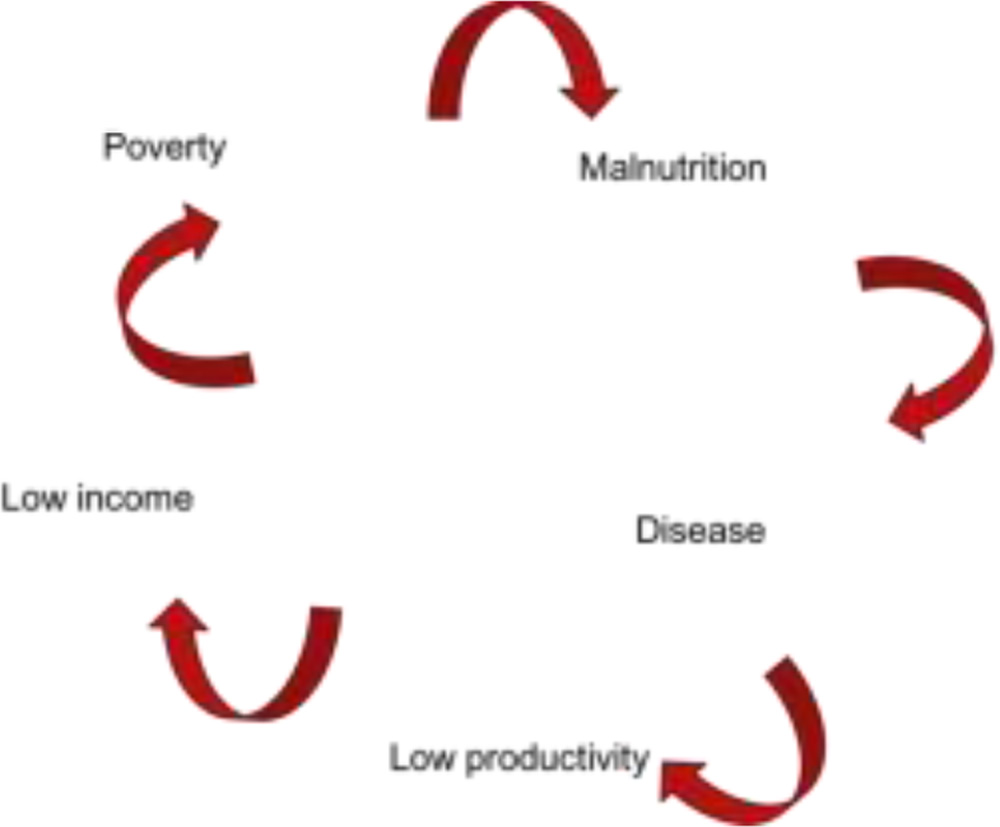
This is the vicious circle of poverty and poor health and it does exist in rural areas of developing countries like India. Presently all community approaches are focusing on diagnosing and treating the diseases. However, time has come to think to reduce prevalence of childhood blindness as a whole from the community.
So, the purpose of this study is to evaluate the role of participatory rural appraisal (PRA) over community based rehabilitation (CBR) to detect and manage childhood blindness from rural community. This prospective non randomized study was initiated in the year 2012 and still carrying on.
Method and Methodology
Fifteen rural villages with preexisting CBR project are selected.Main criteria of this selection are preexisting CBR project with significant number of visually impaired children.PRA like methodology is adopted to reach out rural community to detect childhood blindness, to improve knowledge and general health along with eye care of that community. PRA approaches is also utilized to improve immunization, spacing, proper maternal & child health and overall improvement of lifestyle.WHO classification of blindness is used to categorize the cases.Student’s t test is used to analyze the result.
First step of PRA like approaches is site selection and preliminary site visit. Depending on certain criteria like distance from base hospital, size of villages and socioeconomic status, we selected the villages. However, foremost important criteria for selection is active participation by the villagers for the activities. Then, next step is announcement of activities in the villages and we used locally available resources to spread the activities.
Most important step is data gathering regarding child health in the community and social mapping is very suitable to gather information from the villagers. Most villagers took part in social mapping and they used locally available materials like pulse, bangles, stones, toilet papers etc. to denote important structures of the villages. Then next step is preparation of action plan, we visited houses of villagers to know the environment they are living in, also arrange health awareness lectures by local Ophthalmologist from nearby existing health structures. Basic idea to involve local Ophthalmologist is to build relation with the villagers so that they can visit the nearby existing health structure in future for

Social mapping
eye care. Besides gathering data on childhood blindness, we also encourage strategies to improve health. Simple practices likehand wash, safe drinking water, safe disposal of excreta, well ventilated house, proper drainage, use of mosquito nets, vaccination, spacing between child birth, balance diet,rehabilitation etc. can improve the child health in the rural community. We also organised evening free eye check-up camps in each village. As majority of villagers are daily wagers or cultivators, evening eye camp approach is very well accepted. Final step of this approach is monitoring of activities and matrix index is very useful for this purpose
Results
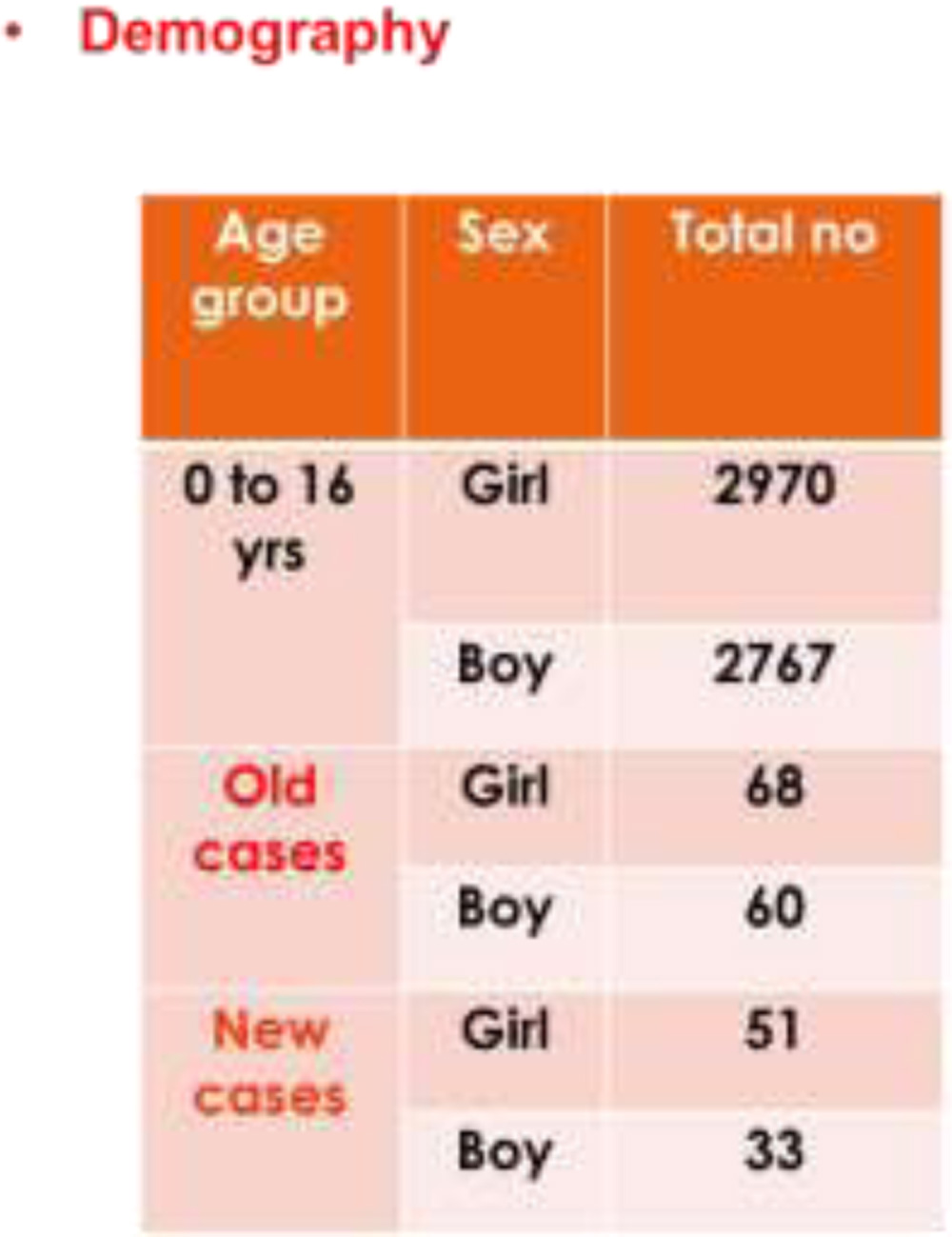
Table 1 shows demographic patterns children of the villagers.
128 children (CBR program) with visual disability are identified out of which 77.14% are blind and 22.86% has SVI. After adopting PRA project 84 new cases (p<0.05%) are detected of which 71.43% are blind and 28.57% has SVI. Main causes of blindness are cornea related in 31%, lens related in 21%, retina related 15%, congenital defect in 11%, buphthalmos in 8% and unknown in 14% cases. Matrix ranking shows improvement over a period of 1 year. All three parameters namely eye health, lifestyle of children and utilization of available health care system shows improvement over 1 year after implementation of this approach.Immunization rate improves from 11% to 81%(p=0.01), Spacing between child birth from12% to 43%(p<0.05). Vision of 9% blind child improved after intervention. Rehabilitation of blind children is very important as in majority of cases treatment is not possible due to delayed diagnosis and also each blind child has to live prolong blind years. It is observed that after adaptation of this project rehabilitation rate has improved from 11% during CBR project to 41% after adopting PRA approach, which was statistically significant.
Conclusion
Avoidance or prevention should be the strategy for childhood blindness as treatment is not possible in majority of cases. PRA like methodology is a new approach in community ophthalmology and is very promising to detect and rehabilitate visually impaired children. CBR method is effective in identifying blind child in the community, however PRA is very useful to improve knowledge, to plan rehabilitation as well to address underlining causes of childhood blindness.