Dr. (Ms). Tulika Ghoshal, G08450, Dr. Soumen Mondal
PREVAILING CLINICAL PRACTICES OF OPHTHALMOLOGISTS REGARDING HBA1C ESTIMATION OF THEIR DIABETIC PATIENTS
Authors– Ms. Tulika Ghoshal, FRCS (Edin.), FICO, MBBS
Dr. SoumenMondal,MS, MBBS
Introduction–
Glycemic control is the key modifiable risk factor associated with the development of diabetic retinopathy.1HbA1c levels correlate well with diabetes control, the progressof diabetic retinopathy andits outcome.
Optimallong termglycemic control,based on HbA1c values,is fundamental to the management of diabetes.2 As Ophthalmologists commonly have to deal with diabetic patients and take part in providing comprehensive care in general and specialised care for eye diseases in particular especially Diabetic Retinopathy, it is imperative that Ophthalmologists should be well conversant with theconcepts of HbA1c and its importance.
There is a general agreement that the duration of diabetes and the severity of hyperglycemia are the major risk factors for developing diabetic retinopathy. Once retinopathy is present, the duration of diabetes appears to be a less important factor than the glycemic control in forecasting progression from earlier to later stages of retinopathy. It is recommended that an HbA1c of 7% or lower is the target for glycemic control in most patients whereas in selected patients, there may be some benefit to setting a lower target of 6.5%.1
This study evaluates the awareness and prevailing clinical practices of Ophthalmologists about HbA1c estimation of their diabetic patients and its important relationship with diabetic retinopathy which is a potentially blinding disease.
Materials and Methods–
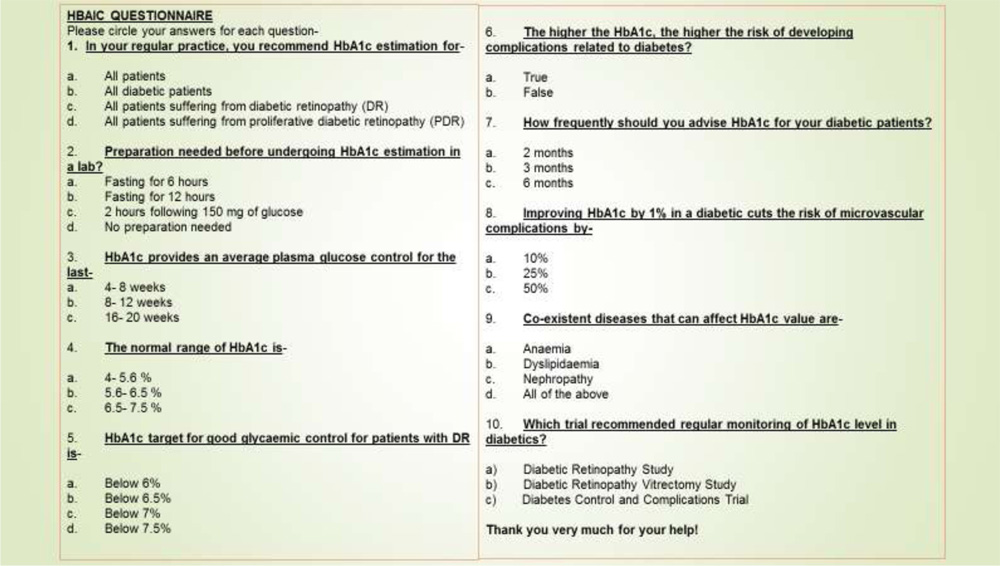
A printed multiple choice questionnaire was devised. It containedten questions regarding normal and abnormal levels of HbA1c, clinical significance, association of HbA1c with diabetic retinopathy and other co-morbid conditions. Each question had 2- 4 choices. The questionnaire was validated by circulating amongst a small sample population and necessary corrections were made. The final questionnaire was circulated amongst Ophthalmologists from different stateswho were attending an Annual Ophthalmological Conference.All the responses were tabulated and analysed.
Figure 1- The final HbA1c Questionnaire which was used.
Results-
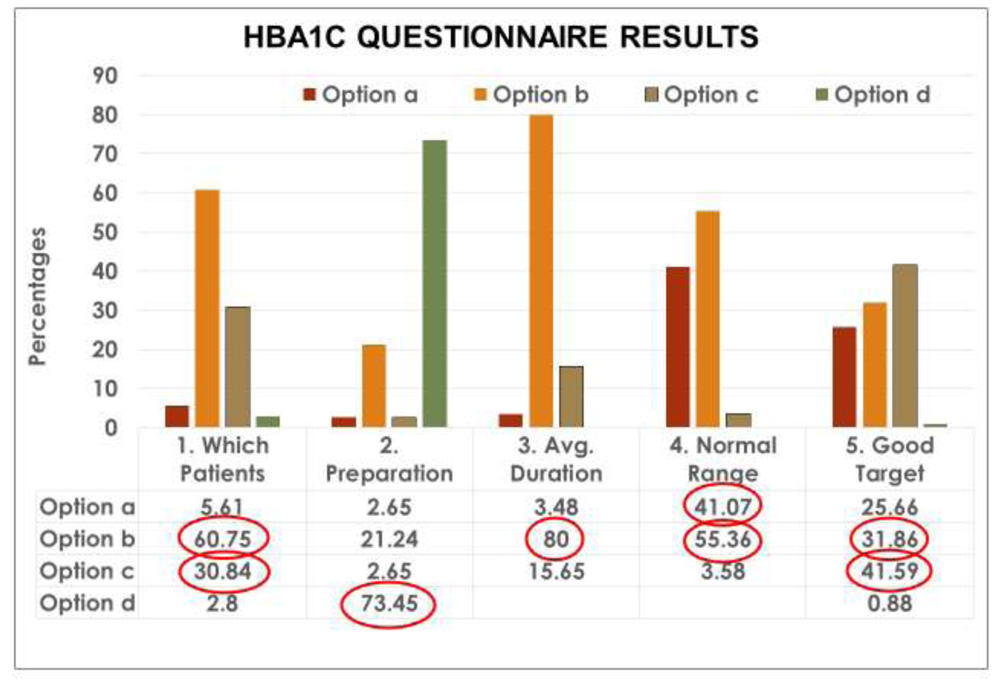
Almost 61% of Ophthalmologists correctly recommended HbA1c for all diabetics (Option b) while nearlyone- third (30.84%) chose only patients with Diabetic Retinopathy. Surprisingly >5% asked for HbA1c in all patients (Option a)and 2.8%requested it for patients with Proliferative Diabetic Retinopathy.
Nearly three- fourths(74%)said that no special preparation is needed before HbA1c testing (Option d). Almost one- fourth (21.24%) chose 12 hours fasting (Option b) despite the fact that HbA1c can be done at any time of the day and has absolutely no relation to food.
80% of Ophthalmologists correctly said that HbA1c provides an average of plasma glucose control over 8-12 weeks (Option b). Nearly 4% chose 4- 8 weeks (Option a) and just over 15% chose 16- 20 weeks (Option c).
Only 41% correctly identified the normal HbA1c range as 4- 5.6% (Option a) while more than half (55%) thought it was 5.6- 6.5% (Option b). Nearly 4% chose 6.5- 7.5% (Option c).
Nearly 42% correctly chose <7% as the HbA1c target for good glycemic control for patients with Diabetic Retinopathy (Option c) whereas almost one- third(31.9%) chose <6.5% (Option b).Just more than one- fourth (25.66%) chose <6% (Option a) and less than 1% chose<7.5% (Optiond).1An HbA1c of 5- 7% indicates good control, 7- 9% indicates poorer control and levels >9% indicate very poor control of Diabetes Mellitus.3
Figure 2- The HbA1c Questionnaire Results for Questions 1- 5.
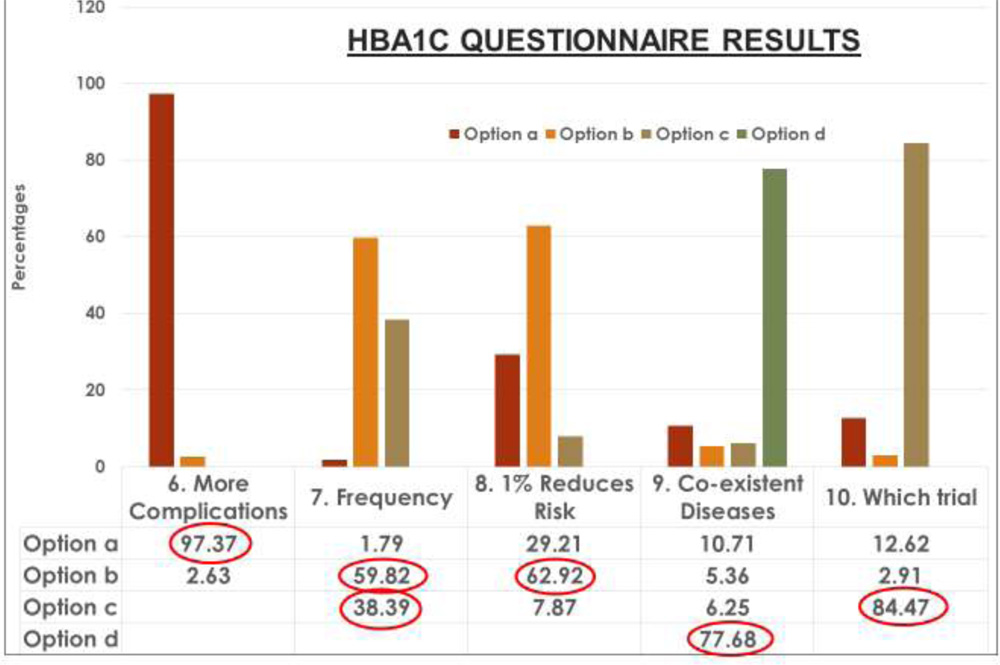
Over 97% of Ophthalmologists agreed that the higher the HbA1c, the higher the risk of developing diabetic complications (Option a) while only 2.63%disagreed (Option b).
Nearly 60% chose 3 months (Option b) as the recommended frequency for testing HbA1c for diabeticswhile more than one- third (38.39%) chose 6 months (Option c). Only 1.79% chose 2 months (Option a).
Almost 63% of Ophthalmologists chose correctly that improving HbA1c by 1% cuts the risk of microvascular complications by 25% (Option b).[DCCT4 and UKPDS5].29.21% chose 10% (Option a) whereas 7.87% chose 50% (Option c).6
Nearly 78% of Ophthalmologists correctly chose all the co-existent diseases that can affect HbA1ci.e. Anemia, Dyslipidemia, Nephropathy (Option d). 10.71% chose Anemia alone(Option a)while 5.36% chose Dyslipidemia (Option b) and6.25% chose Nephropathy(Option c).
Almost 85% correctly chose the Diabetes Control and Complications Trial (Option c) as the trial which recommended regular monitoring of HbA1c levels in diabetics.412.62% chose the Diabetic Retinopathy Study(Option a) whereas 2.91% chosethe Diabetic Retinopathy Vitrectomy Study(Option b).
Figure 3- The HbA1c Questionnaire Results for Questions 6- 10.
Discussion-
Diabetic retinopathy is a leading cause of visual impairment in working-age adults.1Fasting Blood Sugar and Post- Prandial Blood Sugar are only indicative of the Blood Sugar at the moment the blood is drawn and can be easily affected by strict dietary control. HbA1c is the gold standard test with a memory for assessing glycemic control in diabetics.Red blood cells are freely permeable to glucose which irreversibly binds with Hemoglobin to form HbA1c. The life span of red blood cells is 120 days so HbA1c reflects the average plasma glucose levels over the last 2- 3 months.Therefore, HbA1c is preferred over Fasting Blood Sugar and Post- Prandial Blood Sugar in monitoring diabetes. In the United Kingdom’s National Health Serviceonce Diabetics are diagnosed using Fasting Blood Sugar and Post- Prandial Blood Sugar +/- HbA1c, their diabetic control is only monitored by HbA1c unless they require Insulin. HbA1c is done every 3 months if poorly controlled, every 4 months if moderately controlled and every 6 months if well- controlled.3
Figure 4-Ophthalmologists recommendedHbA1c for which of their patients?
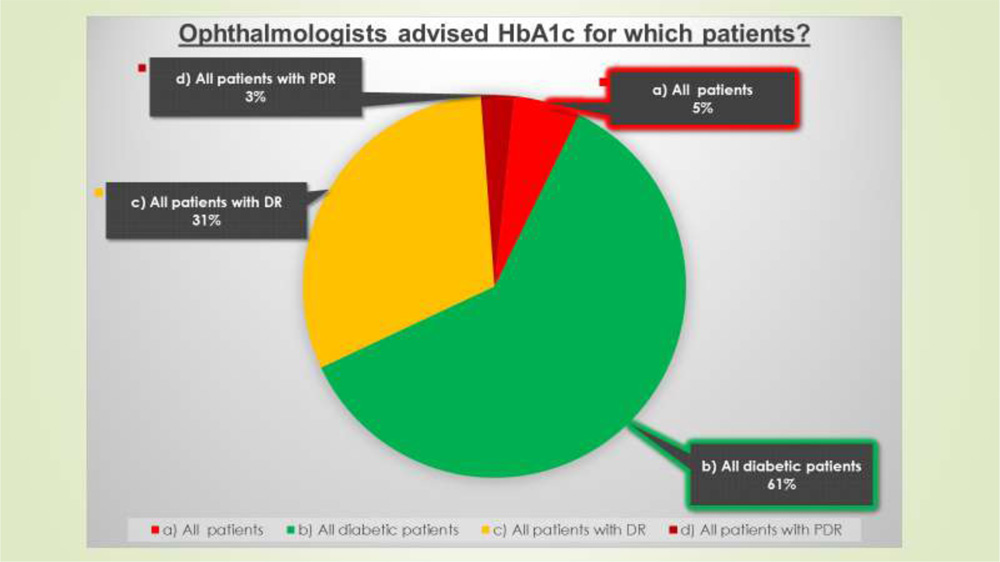
Considering the 1st question from our questionnaire only 61% of Ophthalmologists recommended HbA1c for all Diabetic patients, 31% for patients with Diabetic Retinopathy, 3% for patients with Proliferative Diabetic Retinopathy and surprisingly 5% for all patients whether they had diabetes or not! Therein lies the problem. Unfortunately,Ophthalmologists do not recommend HbA1c as often as they should. However, there is a very strong relationship between the control of Diabetes Mellitus, and therefore HbA1c, with the incidence and progression of Diabetic Retinopathy, a potentially blinding disease. The Diabetes Control and Complications Trial (DCCT) Research Grouprandomized 1441 patients with type 1 diabetes to receive intensive glycemic or conventional therapy. Over 6.5 years of follow-up, intensive treatment [median HbA1c (glycosylated hemoglobin A1c), 7.2%] reduced the incidence of diabetic retinopathy by 76% and progression of diabetic retinopathy by 54%, as compared with the conventional treatment.4It may be logical to assume that the same principles apply in type 2 diabetes (previously called non-insulin-dependent diabetes mellitus [NIDDM]).
Also, according to “Influence of glycosylated hemoglobin on sight-threatening diabetic retinopathy: A population-based study” by Rajiv Raman et al, an HbA1c value >8.0% was significantly related with sight threatening diabetic retinopathy.7
The approach of all Ophthalmologists, Diabetologists and General Practitioners seeing patients with Diabetic Retinopathy should be that good control of blood glucose, blood pressure and plasma lipids are all essential components of modern medical management.8
Pitfalls of this Study-
This study was a small one consisting of only 230 responders. A larger study should give a better idea of the prevailing clinical practices of Ophthalmologists regarding HbAa1c estimation of their diabetic patients.
Conclusions-
Ophthalmologists in India need to be much more aware of HbA1c and its importance in diabetic patients who are at risk of losing their sight permanently.Patients should also be made aware by Ophthalmologists that HbA1c should be regularly checked and controlled to reduce the incidence and progression of diabetic retinopathy.All Ophthalmologistsshould emphasize to the patient the need to adhere to the primary care physician’s guidance to optimize metabolic control1 and should recommend HbA1c, a gold standard test, regularly (every 3, 4 or 6 months according to the level of control) for all their diabetic patients to prevent blindness.
Financial interest- Nil
Source of Support- Nil
Conflict of Interest- None declared
References-
1) American Academy of Ophthalmology Preferred Practice Pattern® Guidelines.http://www.aao.org/preferred-practice-pattern/diabetic-retinopathy-ppp-updated-2016
2) Targets for Glycemic Control- Canadian Diabetes Association Clinical Practice Guidelines Expert Committee- S. Ali Imran MBBS, FRCP(Edin), FRCPC RémiRabasa-Lhoret MD, PhD Stuart Ross MBChB, FRACP, FRCPC.
3) Diabetes UK- https://www.diabetes.org.uk
4) Diabetes Control and Complications Trial (DCCT) Research Group. The relationship of glycemic exposure (HbA1c) to the risk of development and progression of retinopathy in the Diabetes Control and Complications Trial. Diabetes 1995;44:968-83; New England Journal of Medicine, (DCCT, 1993)
5) UK Prospective Diabetes Study (UKPDS) Group. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet 1998;352:837-53.
6) Kohner EM. Microvascular disease: what does the UKPDS tell us about diabetic retinopathy?Diabet Med. 2008 Aug. 25 Suppl 2:20-4. [Medline].
7) Influence of glycosylated hemoglobin on sight-threatening diabetic retinopathy: A population-based study- Rajiv Raman et al; Diabetes Research & Clinical Practice, 2011.
8) Medical management of diabetic retinopathy: Fenofibrate and ACCORD Eye studies- AD Wright and PM Dodson; Eye (2011) 25, 843–849-
Acknowledgements
Dr. Tuhin Chowdhury, MS, DO, MBBS
Dr. Aditya Pradhan, DNB, MBBS