Dr.Kalkoti Prasad Rajkumar, K09709, Dr. Rutika Khadse, Dr. Padmavathy Maharajan, Dr. Neelam Pawar, Dr. Rama Krishnan R
Introduction
Patients with acute ocular motor cranial neuropathies are evaluated with factors like age at presentation, associated systemic risk factors, onset and duration of neuropathy and systemic and neurological signs, based on which diagnoses are concluded. Neuro-ophthalmology traditionally taught us that those individuals older than 50 years of age suffering acute isolated motor cranial neuropathy having vasculopathic risk factors like diabetes mellitus, hypertension, hyperlipidemia can be observed without neuroimaging investigation, as spontaneous resolution of palsy is expected in about 8-10 weeks1,2. Increased incidence of identification of other causes for acute motor mono-neuropathies, which are less benign and treatable, is observed since development of Magnetic Resonance Imaging (MRI)1. Prevalence of these findings is different for third, fourth and sixth cranial nerve palsy and it may beneficial for patient not to follow same traditional treatment recommendation for all.
Here we designed this study to analyze the diagnostic yield of neuroimaging for third nerve palsy
Materials and Methods
This was a prospective observational studyconducted at tertiary eye center in south India, with aim to evaluate diagnostic yield of neuroimaging in cases of third nerve palsy. Patients with third nerve paresis presenting to Neuro-ophthalmology clinic from December 2012 to December 2014 were studied to analyze the various etiologies with the help of neuroimaging in these patients. Specific emphasis was laid on documenting the findings of neuroimaging studies. All patients having third nerve paresis were included in study while patients unable to follow-up or contraindicated for MRI were excluded from the study.
The etiologies of third nerve palsy were grouped into ischemic, inflammatory, traumatic, compressive, congenital, and idiopathic. Cases of third nerve palsy were also grouped as isolated or non-isolated. Presence of any other neuropathies and bilateral third nerve palsies were considered as non-isolated cases.
Etiologies like Inflammatory, compressive and vascular causes (aneurysms hemorrhage) were diagnosed on neuroimaging. Those without positive clinical or radiological findings were classified as idiopathic.
Results
A total of 60 cases were analyzed. We found male preponderance with 41(68%) males and 19 (32%)females. (Chart no.1) Age ranged between 17-78yrs with mean age 50.5yrs (SD±16.07). Age at presentation is elaborated in Table 1.
Chart 1: Sex ratio
| Age at presentation | Total | |
| <20 | 2 | |
| 21- 40 | 16 | |
| 41- 60 | 22 | |
| >60 | 20 | |
| Total | 60 |
Table 1: Age at presentation
Among 60 cases, 48 (80%) had isolated third nerve involvement while 12 (20%) were associated with other neuropathies. Of these 60 cases, 26 (43.3%) cases had presence of vasculopathic risk factors like diabetes, hypertension, hypercholesterolemia, etc. and were grouped as ischemic third nerve palsy. 11 (18%) were diagnosed as having orbital inflammatory etiology, 9 (15%) were attributable to trauma, 4(6%) had history of third nerve palsy from birth but who presented at this age for first time, and were classified as congenital third nerve palsy (6.67%). In 6 (10%) cases cause was undetermined, 4 (6%) cases were secondary to compression of third nerve (Table 2).
| Etiology | No. of cases | Percent (%) |
| Ischemic | 26 | 43.33 |
| Inflammatory | 11 | 18.33 |
| Traumatic | 9 | 15 |
| Congenital | 4 | 6.67 |
| Idiopathic | 6 | 10 |
| Compressive | 4 | 6.67 |
| Total | 60 | 100 |
Table 2: Etiologies of third nerve palsy in our study
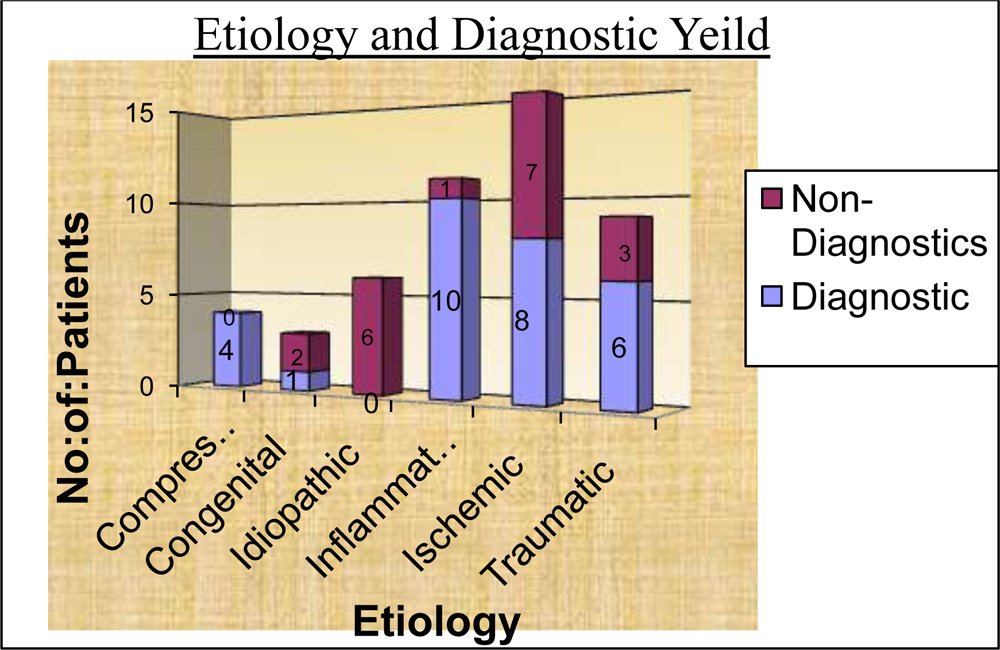
Among 60 cases, neuroimaging was not done for 12 cases, due to presumed ischemic cause and subsequent recovery. 48 cases underwent neuroimaging. In 29 cases it was diagnostic for etiology and in 19 cases MRI was found to be normal, giving a diagnostic yield of 60.41%.
Diagnostic yield of neuroimaging explaining various etiologies is shown in Table 3. Amongst 4 compressive lesions, one had pituitary macroadenoma with its lateral extension, one was diagnosed with Paget’s disease leading to skull thickening causing compression of third cranial nerve, one had extradural hemorrhage compressing third cranial nerve, and one had compression resulting from closely related posterior cerebral artery.
| Etiology | Diagnostic | Non-Diagnostics/WNL | Not Done |
| Compressive | 4 | 0 | 0 |
| Congenital | 1 | 2 | 1 |
| Idiopathic | 0 | 6 | 0 |
| Inflammatory | 10 | 1 | 0 |
| Ischemic | 8 | 7 | 11 |
| Traumatic | 6 | 3 | 0 |
| Total | 29 | 19 | 12 |
Table no. 3 Yield of neuroimaging describing various etiologies
Pupil involvement (PI) was observed in 34 (57%) cases, while 26 (43%) had pupil sparing (PS) third nerve involvement. Pupil involvement in relation to various etiologies is shown in Table 4. Pupil involvement was observed in all cases of inflammatory etiology.
| Etiology | PS | PI | Total |
| Ischemic | 20 | 6 | 26 |
| Inflammatory | 0 | 11 | 11 |
| Traumatic | 0 | 9 | 9 |
| Idiopathic | 2 | 4 | 6 |
| Compressive | 2 | 2 | 4 |
| Congenital | 2 | 2 | 4 |
| Total | 26 | 34 | 60 |
Table 4 :Pupil related to etiology
Discussion
This was a prospective study, to evaluate the necessity of neuroimaging in third nerve palsy (TNP), and also analyzed the demography and etiology. We compared our results with the earlier studies.
Table 5 shows comparison of various etiologies with previous studies.
| Causes | Rama et al | V Menon et al | U C Park et al | Present study |
| Ischemic | 19.3% | 35% | 43% | |
| Inflammatory | 9.5% | 18% | ||
| Traumatic | 21.1% | 18% | 15% | |
| Idiopathic | 10.5% | 18% | 10% |
Table 5: Etiology comparison with previous studies
We found that despite the fact that sophisticated investigative procedures like computed tomography, MRI, MRA, etc. that are available to us, some proportion of cases with unknown etiology exist. Our study had 6 (10%) cases of idiopathic etiology compared to U C Park et al study which was having 18% idiopathic etiology3. In our study, presumed ischemic etiology the most common cause of isolated TNP and about half of these cases spared the pupil. Pseudotumors (idiopathic inflammation) of orbit emerged as a significant cause of cranial nerve palsies especially cases with multiple nerve affection and third nerve palsies. In our study 18% TNP was related to inflammatory etiology compared to V Menon et al4 study showing 9.5% inflammatory etiology.
The presence of any vasculopathic risk factor like diabetes mellitus, hypertension, hypercholesterolemia or coronary artery disease, was associated with peripheral microvascular ischemic etiology. Despite high prevalence of ischemic etiology in cases having vasculopathic risk factors, substantial number of cases 10 (16%) were found to have other etiologies identified by neuroimaging. Out of these 10 cases, 6 had non-isolated palsies with inflammatory etiology, 1 was attributed to trauma, 3 cases were found to have compressive lesions like Paget’s disease, subdural hemorrhage, and compression due to closely situated posterior cerebral artery. Neuroimaging procedures may have a role in the initial evaluation of patients 50 years of age or older with acute ocular motor palsies.
Presumed ischemic etiology for TNP accounted for 10cases (59%) by Schultz et al5 and Lee et al6 19 cases (67.9%) compared with our 26 cases (43.3%). The majority of patients with presumed ischemic TNP (Schultz et al:60%; Lee et al:73%) had normal pupil function, while (Schultz et al:40%; Lee et al:26%) had pupil involvement partially or completely, which is comparable to our study (pupil sparing: 77% and pupil involving :23%).
In the Lee et al series, 3 cases (10.7%) were due to aneurysm, as compared with 2 cases (11.8%) inSchultz et al study. All 3 cases of aneurysm described by Lee et al had complete internal dysfunction, while both patients in Schultz et al study presented with only partial internal dysfunction.We did not find any case of posterior communicating artery aneurysms, compared to Rama et al7 study, which also could find only one case of aneurysmal etiology in their 90 patients and suggested that aneurysms are less common in South India.
We had 4 compressive lesions of which 2 showed pupil involvement while in 2 cases pupil was spared.
We believe that the diagnostic yield for imaging of non-isolated TNP is likely to be high.
Conclusion
Neuroimaging plays important role to evaluate, diagnose & treat TNP .Most common etiology found was ischemic, Inflammatory and Traumatic Majority of pupil involving palsies were secondary to trauma. There were no cases of third nerve palsy due to aneurysms
References
- Tamhankar MA, Volpe NJ. Management of acute cranial nerve 3, 4 and 6 palsies: role of neuroimaging. CurrOpinOphthalmol. 2015 Nov:464–8.
- Murchison AP, Gilbert ME, Savino PJ. Neuroimaging and acute ocular motor mononeuropathies: a prospective study. Arch Ophthalmol 2011; 129:301–305.
- U C Park, S J Kim, J M Hwang, Y S YU. Clinical features and natural history of acquired third,fourth, sixth cranial nerve palsy. Eye (London) 2008 may;22(5):691-6
- Menon V, Singh J, Prakash P. Aetiological patterns of ocular motor nerve palsies. IJO 1984;32:447-453
- Kara L. Schultz, Andrew G. Lee.Diagnostic yield of the evaluation of isolated third nerve palsy in adultsCan J Ophthalmol2007;42:110–115
- Lee AG, Hayman LA, Brazis PW. The evaluation of isolatedthird nerve palsy revisited: an update on the evolving role ofmagnetic resonance, computed tomography, and catheterangiography. SurvOphthalmol2002; 47:137–57.
- Rama V, Vimala J, Chandrasekhar M, Anjaneyulu C, Dinakar I. Ophthalmoplegia. Indian J Ophthalmol 1980;28:13-6