Dr. Ashwini H, A14563, Dr. Lilan Bhat, Dr. Prashob Mohan
Abstract
Meibomian gland dysfunction (MGD) is one of the leading causes of dry eye syndrome. Morphological changes in the meibomian glands (MG) like tortousity, shortening, drop-outs, dilatation and distortion lead to dysfunctioning of glands, and subsequent evaporative dry eye syndrome. Commercially available meibographer is usually used to visualize the MG morphology. However, we tried to image the MG using simple routine out-patient department (OPD) instrument like autorefractomer (Topcon RM8900), non contact tonometer (CT 80 Topcon), fundus camera (Zeiss), Zeiss IOL master 500, specular miscroscope (Topcon SP-3000p), ATLAS 9000 topographer and Visante AS-OCT. The morphological changes of MG were visualized and correlated with the clinical findings of severity of dry eye on the basis of ocular surface disease index (OSDI) score and non-invasive tear film breakup time. This method using simple, non expensive, routine OPD/clinic instruments is very useful and feasible for ophthalmologists.
Aim
To study the morphologic pattern of meibomian glands using routine outpatient department instruments in meibomian gland dysfunction.
Introduction
Meibomian gland dysfunction (MGD) is a chronic diffuse abnormality of the meibomian glands commonly characterised by terminal duct obstruction and/or qualitative/quantitative changes in glandular secretion. It may result in alteration of the tear film, symptoms of eye irritation, clinically apparent inflammation and ocular surface disease.1 Obstructive MGD is a major cause of lipid layer deficiency and evaporative dry eye, and often results in an unstable tear film, damage to the ocular surface epithelium, chronic blepharitis and contact lens intolerance.
Meibography is a technique that yields information on the morphological characteristics of meibomian glands by observing their silhouette through retroillumination of the everted eyelids from the skin side. The conventional meibography done is by shining torch through lid and examining the MGs after everting the lids. This needs physical contact of the torch to the eyelids. While conventional meibography is difficult to apply to the upper eyelid, non-contact meibography allows for observation of a wide area encompassing both the lower and upper eyelids. Instruments offering non-contact meibography are now available in the market in some regions of the world. One is the TOPCON BG-4M for slit lamp, which is an IR illumination system with an external IR CCD. The Meibom Pen is a mobile pen-shaped meibography device ( Japan Focus Corporation, Tokyo, Japan), and others include the Eye Top Topographer, Sirius Scheimpflug Camera and Cobra Fundus Camera (CSO and bon Optic VerttiebsgmbH) and the OCULUS Keratograph 5M (Oculus, Wetzlar, Germany). These instruments no doubt give excellent photographic images of the morphological features of meibomian glands; all eye hospital or clinics may not afford these expensive setup. Especially, in developing nation like India, a simple cost effective yet efficient day today OPD instrument would be handy if we can capture the morphologic features of MGs which will aid us in the better management of MGD. Hence, in that approach, we found that infra red camera of any simple OPD instruments like auto-refractometer, non contact tonometer, IOL master, fundus camera, specular microscope, and corneal topographer which is easily available in almost all eye clinics or hospitals can be utilized for the same. This is first of its kind as per our knowledge and we tried capturing the images from the upper and lower lids after everting them and found them good enough to be used for routine meibography.
Materials and methods
30 eyes of 20 patients diagnosed to have meibomian gland dysfunction (MGD) clinically were recruited from the patients attending our hospital OPD from December 2015 to March 2016. After obtaining clinical history, the patients were evaluated on slit lamp thoroughly. Subjects having ocular symptoms, lid margin abnormalities (irregular lid margin, vascular engorgement, plugged meibomian gland orifices), altered expressibility of the secretion were considered to have MGD. Dry eye questionnaire (OSDI-ocular surface dry eye index) was asked to all patients. Tear film height, tear film breakup time was noted. Meibum expressibility scores (assessed from 5 glands: 0= all glands expressible; 1=3–4 glands expressible; 2=1–2 glands expressible; 3=no glands expressible)2. This can be assessed in the lower or upper lid, and meibum secretion quality score (assessed in each of 8 glands of the central third of the lower lid on a 0–3 scale for each gland: 0=clear meibum; 1=cloudy meibum; 2=cloudy with debris (granular); 3=thick, like toothpaste)3 , were also assessed. Their meibomian glands were then visualized using simple out-patient department(OPD) instrument like autorefractomer (Topcon RM8900), non contact tonometer (CT 80 Topcon), fundus camera (Zeiss), Zeiss IOL master 500, specular miscroscope ( Topcon SP-3000p), ATLAS 9000 topographer and Visante AS-OCT. The lower lid (LL) and upper lid (UL) of all the subjects were everted and images of the MGs were taken. A meibomian gland dropout score (MGDS)4 due to complete or partial gland loss of eye lids was obtained from upper lids using a subjective 4-grade scoring system, (grade 0: no loss of meibomian glands, grade 1: gland dropout area <1/3 of the total meibomian glands, grade 2: gland dropout area 1/3 to 2/3 of the total meibomian glands, grade 3: gland dropout >2/3 of the total meibomian glands, grade 4: total gland drop-out). Presence of tortuosity and visible acinar changes of the meibomian glands were also noted. . Schirmer’s test type 1 and 2 were also done using 35x5mm filter paper.
Inclusion criteria
All patients of either gender above 20 years of age attending our hospital OPD and diagnosed to have MGD clinically.
Exclusion criteria
All patients who were on topical medications, having any ocular infections, contact lens wearer, history of injury to eyes, or who have underwent any ocular intervention procedure or surgery in last 6 months were excluded
Results
30 eyes of 20 patients were analysed. 14(46.7%) eyes belonged to males and 16(53.4%) females. The range of age of the patients belonging was 54 to 80 years as shown in table 1 Mean age was 67.4 years with SD (standard deviation) of 7.16.
Table 1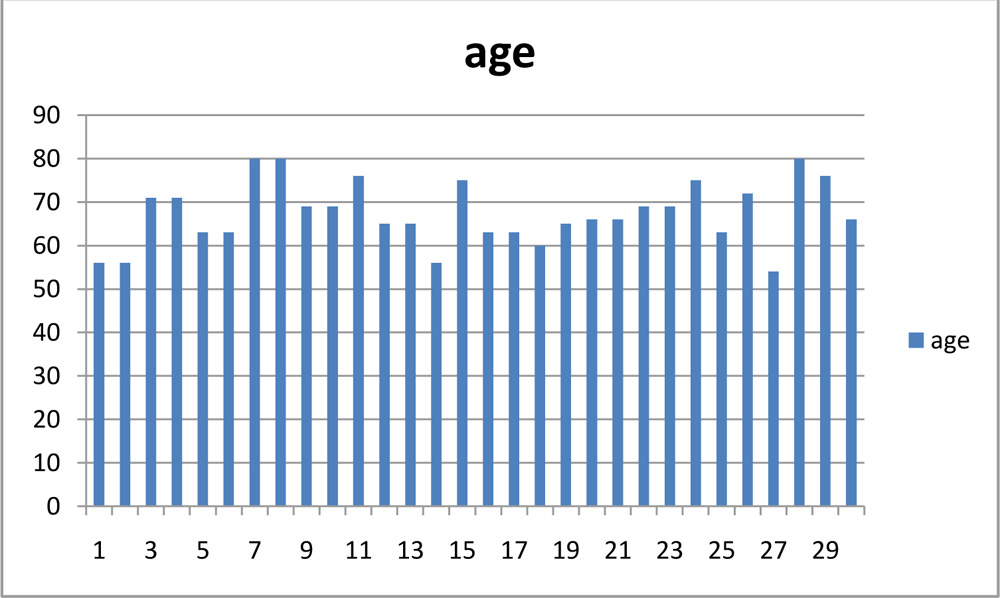
The most common ocular complaints of the patients were foreign body sensation (14 eyes) accounting for 46.7%, followed by itching and watering.(8 eyes- 26.7% and 6 eyes-20% respectively) as shown in table 2.
Table 2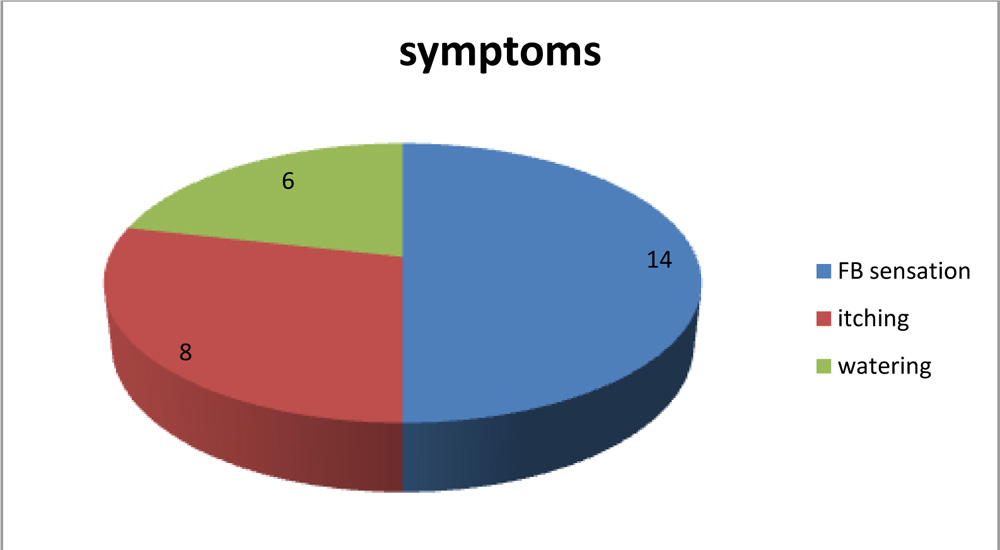
14(46.7%) eyes didn’t have any systemic association followed by diabetes mellitus being the most common (7 eyes) followed by bronchial asthma(3 eyes) hypertension(2 eyes) and cardiac disease(2 eyes). Dry eye questionnaire asked using OSDI had scores ranging from 22.7 to 62.5 as shown in table 3.The mean score was 37.39, median 34.1 and mode value of 31.3.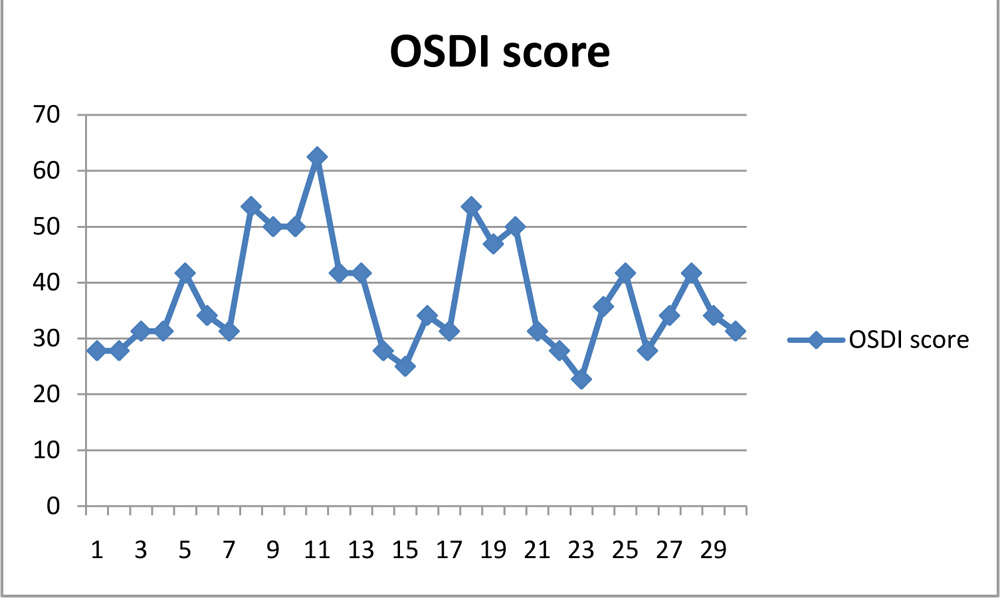
On lid margin examination via slit lamp noted MG block in all the eyes, followed by foaming seen on lid margin (8 eyes) flowed by lid margin vascularization(6 eyes) and keratinization (6 eyes).5 eyes were noted to have enlarged lid margin and 4 eyes had blunting of posterior lid margin as demonstrated in table 4.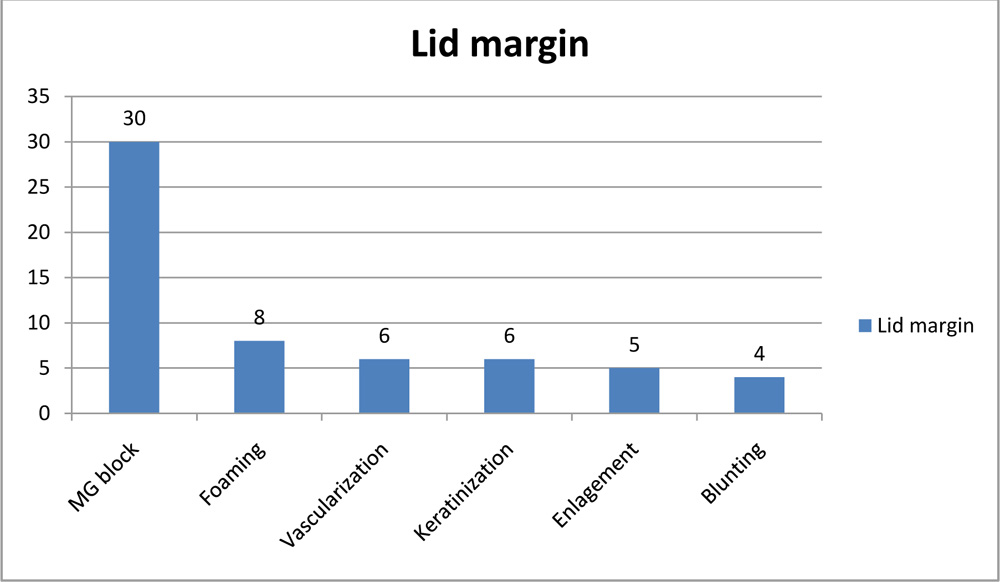
Tear film height was assessed on slit lamp and found that 21(70%) eyes having 0.25mm and 9(30%) eyes had 0.5mm. Non invasive tear film up time (TBUT) was noted and found that all 30 eyes had TBUT less than 10seconds, with 25 eyes (83.3%) having less than 5s and 5 eyes (16.7%) having TBUT between 6 and 10s.Schirmer’s Test Type 1 (without proparacain) done and was found to have mean value of 13.96mm (range-0-35mm) and Schirmer’s Test Type 2 (with proparacaine) had mean value of 13.93mm (range-0-35mm). No difference in the values has been noted between the two types per se. The meibum expressibility score was assessed and found that 3 eyes had score 3(no secretions expressed) and the maximum (14 eyes-46.7%) eyes had score 2, followed by score 1(9 eyes-30%). 4 eyes had score 0, accounting for all gland being expressible as shown in table 5. That means we found that almost 90% eyes had some expressible meibum.
Table 5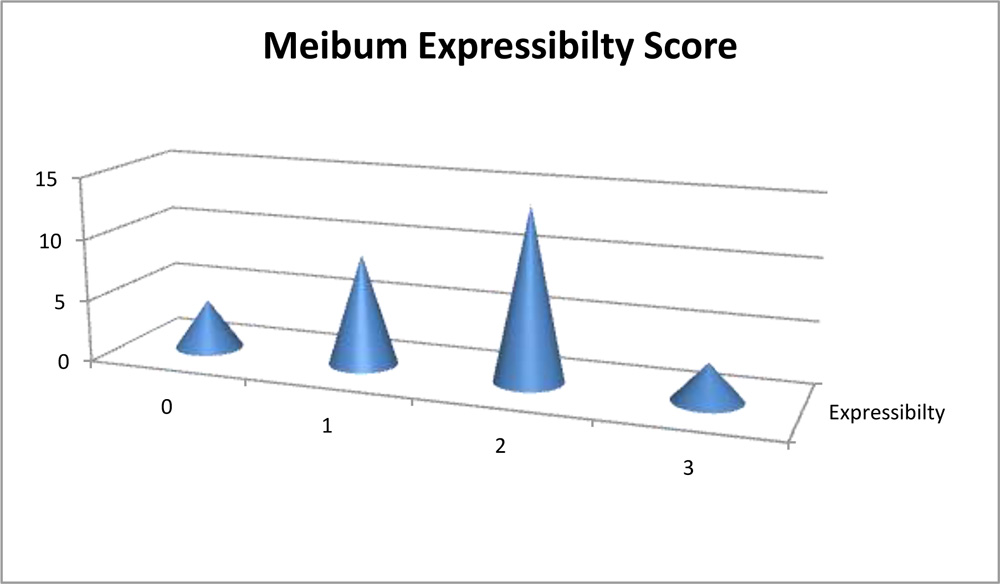
The quality of the expressed meibum was analysed and found that 26 eyes (86.7%) accounting maximum had cloudy type secretion with or without granular debris (score 1 and 2) and only 1 eye had thick toothpaste like material secretion as noted on table 6.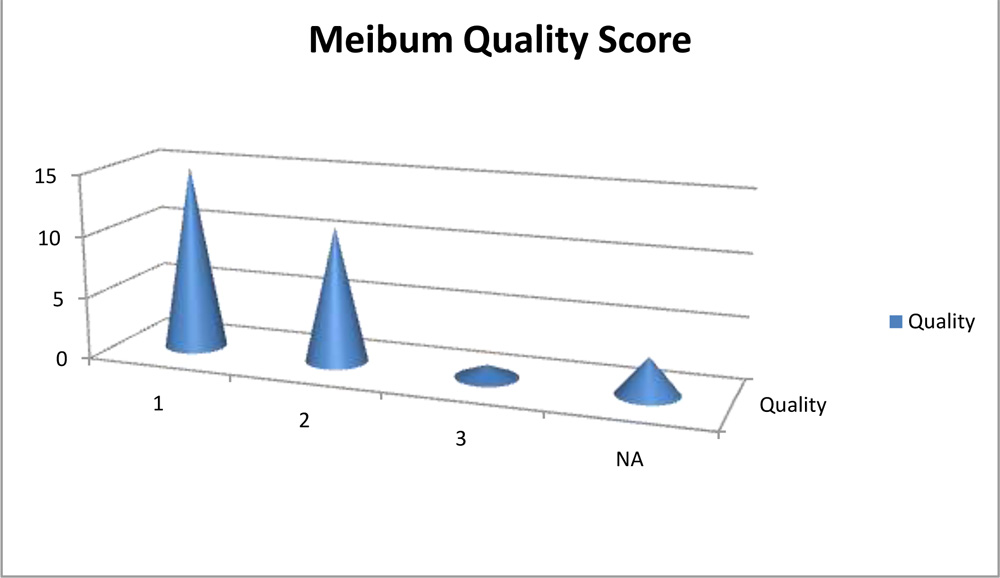
We tried to visualize the MGs by the infra red imaging using autorefractomer (Topcon RM8900), non contact tonometer (CT 80 Topcon), fundus camera (Zeiss), Zeiss IOL master 500, specular miscroscope ( Topcon SP-3000p), ATLAS 9000 topographer and Visante AS-OCT which we have in our hospital. The images obtained were good enough to visualize the morphological features of MGs in these MGD eyes. We noted gland tortousity, shortening of the glands, broadening of the glands and gland drop-outs to various extent in many eyes. The images obtained by autorefractometer, IOL master, specular microscope, fundus camera, corneal topographer and Visante AS-OCT were better than those obtained by non-contact tonometer (NCT). The central shadowing of NCT while noting the MGs obscures the full visualization of MGs. The sample images obtained from these above mentioned instruments are as follows:
Autorefractometer: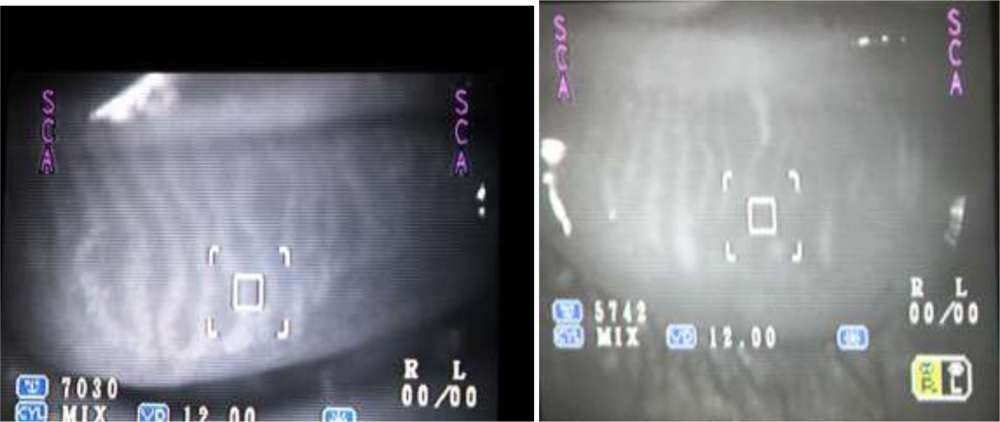
IOL Master: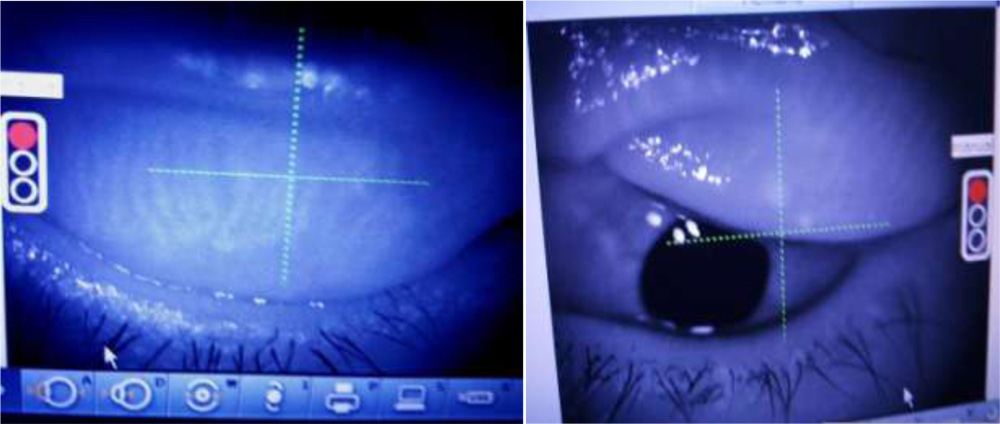
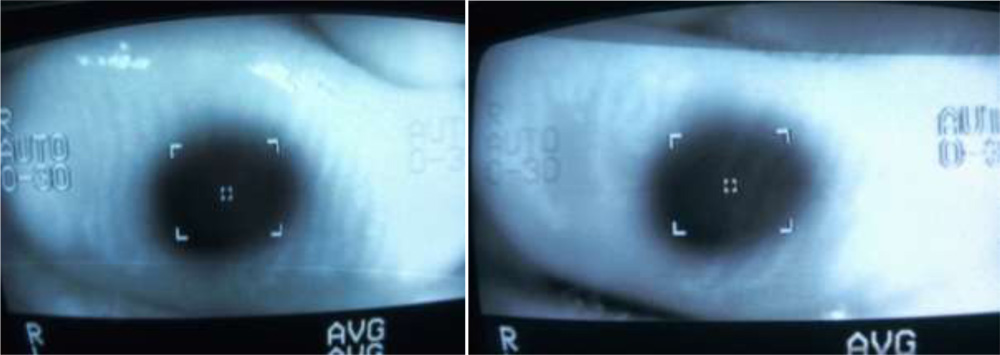 Non-contact tonometer:
Non-contact tonometer:
Specular microscope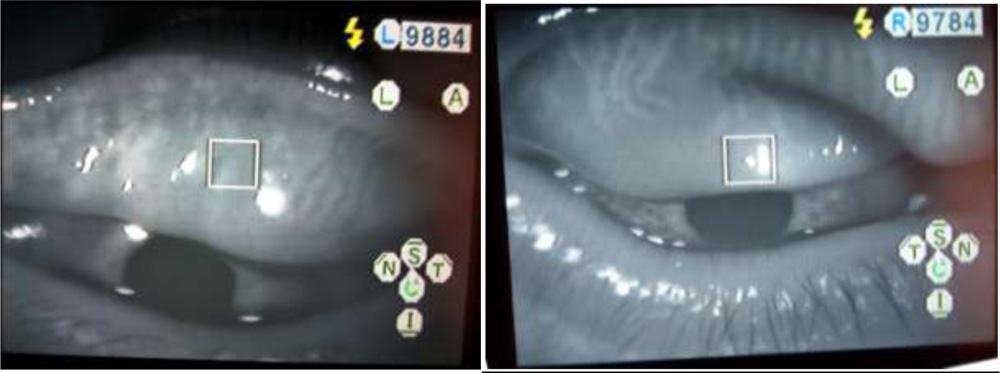
Fundus camera:
Atlas Corneal topographer: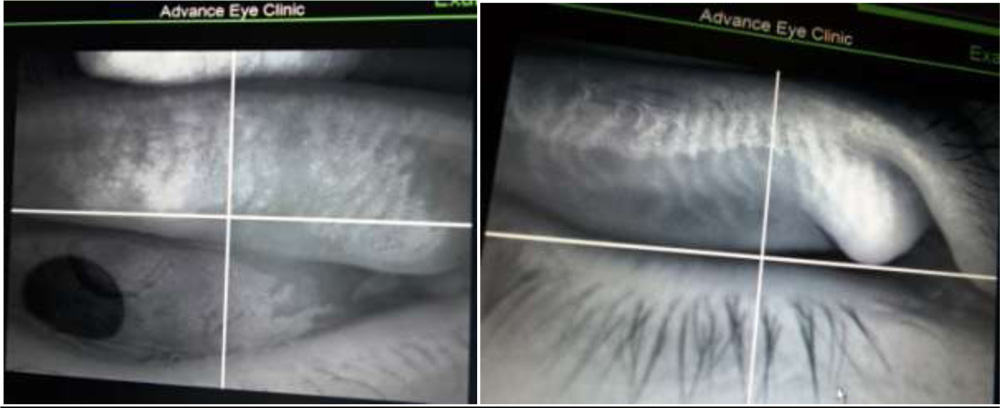
Visante AS-OCT:
On visualizing the MGs, we noted the gland drop outs and graded them. The MGDS (Meibomian gland drop out score) showed grade 2 accounting the maximum with 17 eyes (56.7%) followed by grade 1 and grade 2 almost at same level(6 and 7 eyes respectively). So we found that most of our analyzed eyes had MG dropout more than 1/3rd area of MG but less than 2/3rd noted on the infra red imaging as shown in table no.7.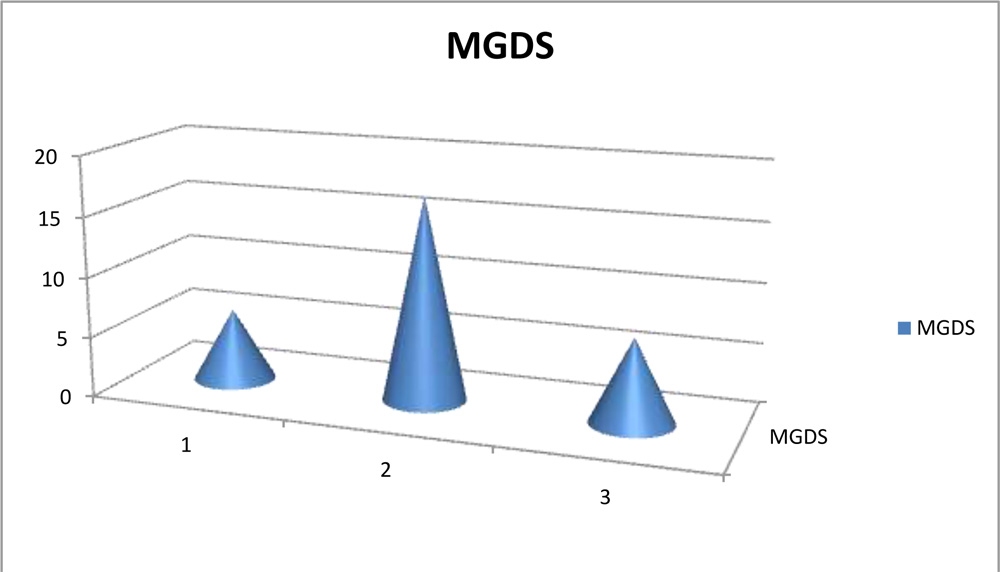
We have noted overall from analyzing the various parameters that eyes with MGDS of 2 or 3 that is MG drop out area of more than 1/3rd of lid had tear film break up time (TBUT) of less than 5 seconds. These eyes were also noted to have meibum expressiblity of 1-2 glands or no expressiblity at all. And the maximum type of expressible meibum was cloudy with or without debris. The tear film height was mostly 0.25mm associated with MGDS of 2 or 3, correlating to the TBUT of less than 5 seconds in these eyes. However, we also noted that presence or absence of systemic illness had no correlation with the MG drop out score. Neither did OSDI have any significant correlation with the grading of MGDS. We also found that lid margin slit lamp findings were varied in appearance ranging from simple MG block or foaming to vascularization and keratinization and had no correlation with MG drop out score. The Schirmer’s test type, both 1 and 2 were found to be not at all relevant in analyzing the extent of meibomian gland dysfunction. It had no correlation with even TBUT, tear film height or meibum expressiblity score or meibum quality grading.
Discussion
This study describes the morphological features of meibomian glands can be examined using the infra red imaging seen in simple out -patient department like autorefractometer, non contact tonometer, IOL Master, specular microscope, fundus camera, corneal topographer and AS-OCT. Various studies have been published in literature elaborating the MG morphological evaluation using commercial meibographers. The progression of severity MGD is reflected in the changes in the morphological features of MGs best described by Robin et al5. Progressive dysfunction results in dilation, distortion, shortening and loss of visualization of the ducts. Arita et al6 reported the coexistence of various morphological changes including enlargement or dilation and also atrophy, narrowing, cut-off, distortion, shortening and dropout in patients with MGD. Because meibomian glands can enlarge in MGD patients, measurement of meibomian gland area alone may not detect MGD in some patients. It is likely, however, that enlargement is an early finding of MGD and that shortening and dropout occur in more advanced stages of the disease. Thus, measuring the meibomian gland area could be useful for diagnosing MGD. Previous studies investigated the correlation between the area of meibomian gland loss and parameters of subjective symptoms and tear film. Pult et al7 reported that meibomian gland loss is significantly correlated with the thickness of the lipid layer, tear break-up time and subjective symptoms8. Ban et al9 reported that parameters of meibomian gland morphology, such as the mean length of meibomian gland ducts and the percentage area of meibomian glands, are significantly correlated with the parameters of tear film such as tear break-up time. All these studies findings closely are reflected in our study too where we too noted correlation between grading of MGDS and expressiblity of MGs, quality of meibum, TBUT and tear film height. However we did find that subjective complaints of MGD patients(as analysed by OSDI questionnaire) in our study had no correlation with morphological features of MGs nor any tear film parameters. We also agree with the finding of previous studies that Schirmer’s test alone doesn’t seem to be reliable indicator of the severity of dry eye status. A latest review article published by Vincenzo Fasanella et al10, reports a novel technique which studies the meibomian glands at cellular level using in vivo scanning laser confocal microscopy (LSCM).The meibography aids clinicians in monitoring the treatment of MGD patients by knowing the follow-up images and comparing the pre and post treatment by noting the morphological changes of the meibomian glands. It also prevents us from blindly advising aggressive lid massaging for MGD patients who have almost near total meibomian gland atrophy, where other options of long acting lubricants seem to be rather better option. Thus, all the analysis suggest that meibography is useful for assessing MGD in turn, ocular surface conditions and aid us it the proper management of dry eye patients and can be done using inexpensive, portable simple instruments of eye clinic/hospitals.
Conclusion
Simple, inexpensive and routine OPD instruments enable morphological assessment of meibomian glands thereby aids in diagnosis and effective treatment of MGD.
Reference
1.Nelson JD, Shimazaki J, Benitez-del-Castillo JM, et al. The international workshop on meibomian gland dysfunction: report of the definition and classification subcommittee. Invest Ophthalmol Vis Sci 2011;52:1930–7.
2.Pflugfelder SC, Tseng S, Sanabria O, et al. Evaluation of subjective assessments and objective diagnostic tests for diagnosing tear-film disorders known to cause ocular irritation. 1998;17:38 –56
3.Bron AJ, Benjamin L, Snibson GR. Meibomian gland disease. classification and grading of lid changes. 1991;5:395–411.
4.Arita R, Itoh K, Inoue K, Amano S. Noncontact infrared meibography to document age-related changes of the meibomian glands in a normal population. Ophthalmology 2008;115:911–5.
5.Robin JB, Nobe JR, Suarez E, et al. Meibomian gland evaluation in patients with extended wear soft contact lens deposits. CLAO J 1986;12:95–8.
6.Arita R, Itoh K, Maeda S, et al. Proposed diagnostic criteria for obstructive meibomian gland dysfunction. Ophthalmology 2009;116:2058–63.
7.Pult H, Riede-Pult B. Comparison of subjective grading and objective assessment in meibography. Cont Lens Anterior Eye 2013;36:22–7.
8.Pult H, Riede-Pult BH, Nichols JJ. Relation between upper and lower lids’ meibomian gland morphology, tear film, and dry eye. Optom Vis Sci. 2012;89:E310–15.
9.Ban Y, Shimazaki-Den S, Tsubota K, et al. Morphological evaluation of meibomian glands using noncontact infrared meibography. Ocul Surf 2013;11:47–53.
10.Vincenzo F et al. In vivo laser scanning confocal microscopy of human mibomian glands in aging and ocular surface diseases.