Dr. Sonal Dua Juneja,
D16060, Dr. Deepak Bhojwani, Dr. Viraj
Abhayakumar Vasavada, Dr. Shail
Dislocated IOLS:Etiology, Risk factors ,management &
visual outcomes
Authors
Dr Sonal Dua Juneja
Dr Viraj Vasavada
Dr Abhay R. Vasavada
Dr Deepak Bhojwani
Dr Shail Vasavada
Iladevi Cataract & IOL Research Center, Raghudeep Eye Clinic, Gurukul Road, Memnagar,Ahmedabad, India.
Address :
Raghudeep Eye Hospital,
Gurukul Road, Memnagar,
Ahmedabad – 380052. India.
E-mail: info@raghudeepeyeclinic.com
Dislocated IOLS:Etiology, Risk factors ,management &
visual outcomes
INTRODUCTION
Posterior Chamber IOL subluxation or dislocation as a late complication of cataract surgery is uncommon but represents one of the most serious complications & has been reported with increasing frequency in recent years.1-4 The incidence of surgery specifically due to late dislocated IOL is 0.032–0.28%.5-6
These dislocations are divided into early occurring within 3 months and late presenting after 3 months.
- Early dislocations,occurs most often due to intraoperative zonular dehiscence, insufficient capsular support (i.e. Posterior capsular tear ) or improper placement of IOL.
- Late dislocations, mainly occurs due to progressive zonular weakness or capsular bag contraction years after an uneventful cataract surgery.
Other associated conditions predisposing to zonular dehiscence are aging, high myopia, uveitis, trauma, previous vitreoretinal surgery, retinitis pigmentosa,Diabetes mellitus, atopic dermatitis, previous acute angle-closure glaucoma attack, and connective tissue disorders.1
MATERIAL & METHODS
A single center ,retrospective ,observational study.The medical records of all patients who developed IOL dislocation were reviewed from Feb 2013 to Feb 2016.
- Data retrieved included age, gender, laterality, duration of IOL dislocation after previous cataract surgery, cause for dislocation, ocular comorbidity , axial length & previous surgery details were noted.
- Management for dislocation, Visual acuity (VA) before and after the surgeryuntil 6 months post operatively &post operativecomplications were reviewed.
RESULTS
Total 28 eyes of 26 patients presented with dislocationof Intraocular lens were reviewed.
- Out of them 20 (71.42%) were males & 8 (28.57%) females, mean age was 58.75 years (range 15-81 years).24 patients presented with unilateral IOL dislocation & 2 patients had bilateral dislocation.
Table 1.Demographics
| PARAMETERS | n (%) |
| No. of patients | 26 |
| No. of eyes | 28 |
| Male | 20(71.42%) |
| Female | 8(28.57%) |
| Age (mean) | 58.75 |
| Age (range) | 15-81 |
| Unilateral | 24 patients |
| Bilateral | 2 patients |
- In most of the cases dislocation occurred spontaneously, most common identifiable cause was pseudoexfoliation followed by posterior capsular tear,high myopia (axial length ≥26.5mm), trauma ,uveitis &atypical retinitis pigmentosa.
Table 2. Cause of IOL dislocation
| Cause of IOL Dislocation | No. of Cases |
| Spontaneous | 8 |
| PEX | 7 |
| PCR | 6 |
| High Myopia* | 3 |
| Uveitis | 2 |
| Trauma | 1 |
| Atypical RP | 1 |
*High Myopia was defined in our study as eyes having Axial Length of ≥26.5mm
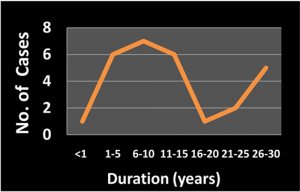
- Mean time between cataract surgery & IOL dislocation is 12.5 years
Majority cases dislocation occurred within 6-10 years & also after 20 years after
cataract surgery.
Table 3. Duration of IOL dislocation
| Duration (in years) | No. of Cases |
| < 1 | 1 |
| 1-5 | 6 |
| 6-10 | 7 |
| 11-15 | 6 |
| 16-20 | 1 |
| 21-25 | 2 |
| 26-30 | 5 |
Surgical correction was performed in the form of IOL exchange with implantation of new IOL & IOL refixation.
- In 20 eyes IOL exchange was done with Scleral fixated IOL (SFIOL)in 10 cases, Intra-scleral fixation in 2 cases & 3 piece IOL implantation with optic capture in 6 cases.
- In 8 eyes IOL refixation was performed with intra-scleral glued IOL in 4 cases, trans-scleral fixation in 3 cases & in 1 case IOL was placed in ciliary sulcus.
Table 4. Surgical intervention
| Surgical Intervention | No. of Cases |
| IOL Re-fixation
a) Ciliary Sulcus b) Intrascleral fixation (GLUED IOL) c) Transcleral fixation |
8(29%)
1 4
3 |
| IOL Exchange (+PPV)
a) SFIOL b) Intra-scleral fixation c) 3 piece IOL with optic capture |
20*(71%)
10 2 6 |
*2 cases were left aphakic
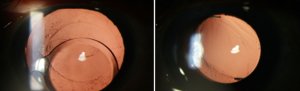
a) Preoperative (b) Post op 3months
Fig 1.(a)Preoperative-Single piece acrylic IOL dislocated into anterior chamber (b)
IOL explantation with new IOL implantation haptics in ciliary sulcus & optic capture
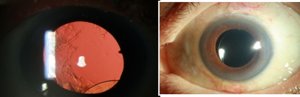
a) Preoperative (b) Post op 6 months
Fig 1.(a)Preoperative- Complete IOL dislocated (b) IOL repositioning- intrascleral glued IOL
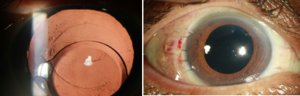
Preoperative Post op 4 months
(IOL exchange with SFIOL )
Fig 1.(a)Preoperative- Complete IOL dislocated (b) IOL exchange with Scleral fixated IOL
- Most common post operative complications were cystoid macular edemain 3 cases(33.3%) & glaucomain 3 cases(33.3%) followed by decompensated cornea in 2 cases(22.2% ) & 1 case(11.11%) with preexisting macular hole developed retinal detachment.
Table 6.Complications post management of IOL dislocation
| Complications post Mx of IOL
Dislocation |
No. of cases |
| CME | 3 |
| Glaucoma | 3 |
| Decompensated cornea | 2 |
| RD with preexisting macular hole | 1 |
- Out of 3 cases of cystoid macular edema 2 were managed conservatively & 1 was given intravitreal Ozurdex.
- There were 5 cases with pre-existing glaucoma out of which 4 remained stable & 1 worsened in whom Ahmed glaucoma valve surgery was performed. New onset glaucoma occurred in 2 cases &were managed conservatively.
- 2 cases developed decompensated cornea out of which 1 had preexisting decompensated cornea.
- 1 case with preexisting full thickness macular hole developed Retinal detachment.
Mean logMAR BCVA preoperatively & post operatively after 6 months showed significant improvement(P value <0.0001).
DISCUSSION
Posterior chamber IOL dislocation or decentration is a well known complication post cataract surgery & it occur when the integrity of posterior or equatorial capsule is disturbed.
The findings in our study have shown that most cases of IOL dislocation occurred within 6-10 years after cataract surgery & also after 20years of primary cataract surgery. Mean duration for IOL dislocation was 12.5 years.
Common theories postulated for late spontaneous IOL dislocation are progressive zonular weakness & capsular bag contraction years after an uneventful surgery.
The role of capsule contraction syndrome, before the popularization of capsulorhexis late in-the-bag dislocation was virtually unreported. The centripetal forces on the zonule caused by the fibrosis around an intact capsulorhexis are more pronounced than on the irregular edge of a can-opener capsulotomy and recent studies have found that dislocation occurs earlier in cases with capsular phimosis & also capsular contraction results in additional stress on potentially weak zonules.7
Some degree of capsule contraction is common in most eyes, but profound capsule shrinkage has been described in pseudoexfoliation, diabetes mellitus, uveitis, pigmentary retinal degeneration and myotonic dystrophy.8
Lina Krėpštė 9have reported mean duration of IOL dislocation of 5.5 year in their study &Davis et al4&Ferna´ ndez-Buenaga et al9 reported 8.5 years&7.5 years respectively.
IOL dislocation in majority cases occurred spontaneously in our study.The most common identifiable cause was found to be Pseudoexfoliation,7 cases(26%) followed by posterior capsule tear,6 cases(21%),high myopia,3 cases(11%), uveitis, 2 cases(7%),trauma, 1case(3.5%) &atypical retinitis pigmentosa,1 case(3.5%).
Davis et al4 reported pseudoexfoliation & vitrectomy surgery as the most common associated conditions for late IOL dislocation whereas Ferna´ ndez-Buenaga et al10 reported high myopia as the main risk factor for IOL dislocation.
The dislocation of a natural lens in patients with PEX is a widely recognized condition. A natural lens can be dislocated either spontaneously or intraoperatively. 11The pseudoexfoliative material has been shown to disrupt the zonules at 3 levels:
1) at the origin of the ciliary body where they are anchored;
2) in the pars plicata of the ciliary body where they pass alongside the ciliary processes;
and
3) at their attachment to the anterior lens capsule 12.
The contributory factors leading to further disruption include an increased friability and a decreased tensile strength of the zonules. In such cases, even after endocapsular IOL implantation, immediate postoperative IOL dislocation or late decentration can occur. This finding is attributed to decentration of the entire capsular bag because of zonular weakness and damage .13
High-myopic eyes show some typical alterations due to thinning and degeneration of several eye layers as lacquer cracks, chorioretinal atrophy, or posterior staphyloma14. It has been hypothesized that, as well as the previously mentioned alterations, these eyes may be also more prone to zonular failure due to excessive elongation of the zonular fibers, which have to support greater stress than in emmetropic eyes15-16.
Taking into account the two mechanisms involved in the dislocation, preventive strategies can be divided into three categories:
- The first, with full consensus among surgeons, includes those measures that minimize zonular damage during cataract surgery in at-risk cases, since we cannot stop progressive zonular dehiscence.17
- The second and more controversial strategy is whether to modify the IOL implantation site/technique. In-the-bag placement with some form of scleral IOL fixation (scleral suture of a capsular tension ring (CTR), Cionni ring, Ahmed segment, etc.) can be accomplished in cases of severe zonular instability during surgery.
An alternative technique would be to implant the IOL in the sulcus, performing an anterior optic capture. Although there is no agreement in the literature over the best option, it is our opinion that it is preferable for the IOL to be implanted within the capsular bag and fixated rather than implanted in the sulcus, a technique that is associated with more inflammation and risk of pigment dispersion if optic capture is not accomplished.17
The role of CTR in prevention is a matter of debate 5,7,18Some authors have hypothesized that the ring could prevent dislocation & capsular shrinkage.However, cases of in the bag dislocation with a CTR within the bag have been published.5,7,18
Moreover, it has been found that the interval between the original cataract surgery and IOL dislocation is shorter in cases with CTR.5,18This could be the result of selection bias, with CTR being implanted in the worst cases, or increased zonular damage due to additional stress on the zonules during implantation of the CTR. Thus, ubiquitous prophylactic use of CTRs does not seem to be a suitable approach in patients with pseudoexfoliation and no phakodonesis undergoing cataract surgery. However, it is our opinion that CTRs are advisable in cases of zonular insufficiency and in advanced pseudoexfoliation syndrome.
- Lastly,the third preventive strategy would be careful observation of the capsulorrhexis after surgery.We recommend anterior relaxing capsulotomy as a preventive measure to halt progressive capsular shrinkage in susceptible eyes, and it should be performed as soon as early contraction is detected,usually in the first month after surgery.
Thus we believe that in mild cases of pseudoexfoliation with no phacodonesis,the IOL may be implanted in the bag with close monitoring of capsular contraction: in moderate cases a CTR be implanted: in severe cases with intraoperative evidence of zonular instability ,in the bag placement with some form of scleral IOL/CTR fixation(scleral suture of a CTR,Cionni ring, Ahmed segment, etc) is strongly recommended.
Surgical correction was performed in the form of IOL exchange with implantation of new IOL & IOL refixation.
- In 20 eyes IOL exchange was done with Scleral fixated IOL (SFIOL)in 10 cases, Intra-scleral fixation in 2 cases & 3 piece IOL implantation with optic capture in 6 cases.
- In 8 eyes IOL refixation was performed with intra-scleral glued IOL in 4 cases, trans-scleral fixation in 3 cases & in 1 case IOL was placed in ciliary sulcus
Surgical approaches include repositioning and replacement. In majority of our cases we performed IOL exchange procedure along with 3 port pars plana vitrectomy & implanted a new IOL.
Adem gul et al19 observed that visual acuity improved following the use of either IOL repositioning or IOL exchange. No superiority of one method over the other was observed.
Post operative complications observed in our study were cystoid macular edema 3 cases(33.3%) & glaucoma in 3 cases(33.3%) followed by decompensated cornea in 2 cases(22.2% ) & 1 case(11.11%) with preexisting macular hole developed retinal detachment.
Out of 3 cases of cystoid macular edema 2 were managed conservatively & 1 was given intravitreal Ozurdex.There were 5 cases with pre-existing glaucoma out of which 4 remained stable & 1 worsened in whom Ahmed glaucoma valve surgery was performed. New onset glaucoma occurred in 2 cases &were managed conservatively.
2 cases developed decompensated cornea out of which 1 had preexisting decompensated cornea. 1 case with preexisting full thickness macular hole developed Retinal detachment.
Zheng Dan-ying et al20comprised IOL redislocation, retinal detachment,
transient elevation in intraocular pressure, transitorycorneal edema, CME, and vitreous hemorrhage as the post operative complications in their study.
Mean logMAR BCVA preoperatively & post operatively after 6 months showed significant improvement (P value <0.0001).
Zheng Dan-ying et al, reported in their study posterior chamber intraocular lens exchange surgery could provide satisfied final visual outcomes.
Fernández-Buenaga R10 reported Lens exchange with scleral suture-fixated IOL was the most frequently chosen treatment. CDVA improved significantly after surgery with a low rate of complications.
CONCLUSION
In our study, the most common identifiable cause for late spontaneous IOL dislocation was pseudoexfoliation.IOL exchange with implantation of new intraocular lens was performed in majority cases. Most common post operative complication observed in our cases was cystoid macular edema & glaucoma. Mean logMAR showed significant visual improvement preoperative & post operative 6 months. We implicated that pseudoexfoliation cases are at lifelong risk for IOL dislocation & need to be assessed periodically.
REFERENCES
1.Ascaso FJ et al, “Epidemiology, Etiology, and Prevention of Late IOL-Capsular Bag Complex Dislocation: Review of the Literature”, Journal of Ophthalmology, Vol. 2015, Article ID 805706, 7pages
2.Gimbal HV, Condon GP, Kohnen T, Olson RJ, Halkiadakis I. Late in-the-bag intraocular lens dislocation: incidence, prevention, and management. J Cataract Refract Surg. 2005; 31(11):2193–2204. [PubMed: 16412938]
3.Hayashi K, Hirata A, Hayashi H. Possible predisposing factors for in-the-bag and out-of-the bag intraocular lens dislocation and outcomes of intraocular exchange surgery. Ophthalmology. 2007;114(5):969–975. [PubMed: 17320961]
4.Davis D, Brubaker J, Espandar L, et al. Late in-the-bag spontaneous intraocular lens dislocation:evaluation of 86 consecutive cases. Ophthalmology. 2009; 116(4):664–670. [PubMed: 19344819]
5.Jakobsson G, Zetterberg M, Lundstrom M, Stenevi U, Grenmark R, Sundelin K. Late dislocation of in-the-bag andout-of-the bag intraocular lenses: ocular and surgical characteristics and time to lens repositioning. J CataractRefract Surg 2010; 36: 1637–1644.
6.Clark A, Morlet N, Ng JQ, Preen DB, Semmens JB. Whole population trends in complications of cataract surgery over 22 years in Western Australia. Ophthalmology 2011; 118(6):1055–1061
7.Werner L, Zaugg B, Neuhann T, Burrow M, Tetz M. In the bag capsular tension ring and intraocular lens subluxation or dislocation. A series of 23 cases.Ophthalmology 2012; 119: 266–271.
8.G. Jakobsson, M. Zetterberg, M. Lundstr¨om, U. Stenevi, R. Grenmark, and K. Sundelin,“Late dislocation of in-the-bag and out-of-the bag intraocular lenses: ocular and surgical characteristics and time to lens repositioning,” Journal of Cataract & Refractive Surgery, vol. 36, no. 10, pp. 1637–1644, 2010.
9.L. Kr˙epˇst˙e, L. Kuzmien˙e, A. Miliauskas, and I. Januleviˇcien˙e, “Possible predisposing factors for late intraocular lens dislocation after routine cataract surgery,” Medicina, vol. 49, no. 5, pp. 229–234, 2013.
10.Fernández-Buenaga R, Alio JL, Pérez-Ardoy AL, Larrosa-Quesada A, Pinilla- Cortés L, Barraquer R, Alio JL 2nd, Muñoz-Negrete FJ. Late in-the-bag intraocular lens dislocation requiring explantation: risk factors and outcomes. Eye (Lond). 2013 Jul;27(7):795-801; quiz 802.
11.Jehan FS, Mamalis N, Crandall AS. Spontaneous late dislocation of intraocular lens within the capsular in pseudoexfoliation patients. Ophthalmology 2001;108:1727-31.
12.Schlotzer-Schrehardt U, Naumann GO. A histopathologicstudy of zonularinstability in pseudoexfoliation syndrome.Am J Ophthalmol 1994;118:730-43.
13Drolsum L, Ringvold A, Nicolaissen B. Cataract and glaucoma surgery in pseudoexfoliation syndrome: a review. ActaOphthalmol Scand 2007;85:810-21.
14.J. J. Kanski, Clinical Ophthalmology. A Systematic Approach, Elsevier, Madrid,Spain, 6th edition, 2009.
15.H.-M. Cheng, O. S. Singh, K. K. Kwong, J. Xiong, B. T.Woods, and T. J. Brady,“Shape of the myopic eye as seen with highresolutionmagnetic resonanceimaging,” Optometry and VisionScience, vol. 69, no. 9, pp. 698–701, 1992.
16.H. R. Wilbrandt and T. H. Wilbrandt, “Pathogenesis and management of the lens-iris diaphragm retropulsion syndrome during phacoemulsification,”Journal of Cataract and RefractiveSurgery, vol. 20, no. 1, pp. 48–53, 1994.
17.Lorente R, de Rojas V. Luxacióntardía del complejosaco capsular y lente intraocular. In: Lorente R, Mendicute J eds. Cirugía del cristalino. LXXXIV PonenciaOficial de la Sociedad Española de Oftalmología, 2008; vol. II: 1751-1767
18.R Lorente, MV de Rojas, P Vazquez de Parga, et al. Management of late spontaneous in-the-bag intraocular lens dislocation: a etrospective analysis of 45 cases. J Cataract Refract Surg. 2010; 36: 1270- 1282.
19.Gul A, Duran M, Can E1, Yucel OE, Sullu Y; Surgical management of intraocular lens dislocations. Arq Bras Oftalmol, 2015 Sep-Oct;78(5):313-7. 20.ZHENG Dan-ying, CHEN Li-na, SUN Yi, SHAO Ying-feng, LIANG Jing-li and LIU Yi-zhi Out-of-the-bag intraocular lens dislocation: outcomes of posterior chamber intraocular lens exchange, risk factors, and prevention Chin Med J 2010;123(18):2562-2567