Dr. Rushad Shroff, S14772
Dr. Luci Kaweri, K16966, Dr. Mathew Kurian, Dr.
Rohit Shetty, Dr. Tejal S. J.
Luci Kaweri, Mathew Kurian, Rohit Shetty
Abstract:
Purpose:To assess the repeatability and agreement of a new swept source optical coherence tomography biometer an optical low coherence reflectometer, a dual scheimpflug ray tracing biometer and a Partial Coherence Interferometer AL scan to measure the keratometry (K), Astigmatism (AST), Axial length (AL), Anterior chamber depth (ACD), central corneal thickness (CCT) and white-to-white (WTW) in cataractous eyes in a prospective study.
Methods:Fifty eyes of fifty consecutive patients scheduled for cataract surgery were included. Three consecutive scans was performed using the four biometers (IOL Master® 700, Carl Zeiss Meditec, Lenstar 900, Haag-Streit AG, Koeniz, Switzerland, Galilei G6, Ziemer, Switzerland, Nidek Co. Ltd., Japan) by a single operator. Within-subject standard deviation (Sw), test–retest repeatability (TRT) and coefficient of variation (COV) for assessing repeatability were assessed. Bland-Altman plots for the agreement between the mean measurements of each machine were examined.
Results:The Mean age of patients was 60.2 + 10.6 years. Dropouts for AL measurement were significantly higher in AL scan and Galilei G6 compared to IOL Master 700. There was good agreement between IOL Master 700 and Lenstar LS 900 for axial length and keratometry (p<0.5). High variability was seen between the 4 machines for Astigmatism and WTW.
Conclusion:The new SS-OCT biometer showed valid measurements, good repeatability and good agreement with the OLCR biometer. The new long range SS-OCT biometer was better than the other 3 devices in acquiring axial length measurements in denser cataracts due to better penetration.
INTRODUCTION
Accurate pre-operative measurement of ocular structures is mandatory for precise postoperative results. Ultrasound biometers were the first biometers to be introduced. Later, the IOL Master® 500 (Carl Zeiss Meditec) optical biometer was introduced and soon became the standard for AL measurements1, 2. It is based on the principle of Partial coherence interferometry (PCI).
An optical low-coherence reflectometry (OLCR), the Lenstar 900 (Haag-Streit AG, Koeniz, Switzerland),3, 4 measures all parameters in a single step. In 2012, a new biometry device combining optical interference principle (AL-Scan, Nidek Co., Ltd.) was introduced for performing ocular measurements including central corneal thickness (CCT), anterior chamber depth (ACD), axial length (AL), keratometry (K) values, corneal dioptric power in the flattest meridian (flat K), corneal dioptric power in the steepest meridian (steep K), and the white-to-white (WTW) distance.Ziemer Ophthalmic systems (Switzerland) introduced Galilei G6 with dual schiempflug combined with placido technology along with ray tracing biometry for more accurate measurement of anterior segment parameters.The latest biometer available commercially (IOL Master®700, Carl Zeiss Meditec) uses swept source optical coherence tomography (SS-OCT) to acquire measurements from various ocular structures. It provides OCT images of the lens that can help in detecting pathologies like lens tilt whereas OCT images of fovea help to confirm central fixation by observing foveal alignment.
The aim of this study was to assess the repeatability and agreement in measuring anterior segment parameters using the Lenstar 900, IOL Master®700, Nidek AL scan and Galillie G6 biometers and to decide which is the best biometer to buy.
METHODS:
This prospective study was carried out at a tertiary eye care center in Bangalore, India, with the approval of the institute’s ethics committee. The study was carried out in accordance with the guidelines laid down in the Declaration of Helsinki. Written informed consent was obtained from all patients before the commencement of the study. Fifty eyes of 50 patients underwent scans in random order using the four instruments. For statistical analysis, data from only one eye of patient was included.
All subjects underwent routine preoperative eye examinations including visual acuity, intraocular pressure (IOP), slit-lamp examination, and fundoscopy along with biometry measurements. A single operator obtained three measurements per eye for all the machines.
Scans with a quality specification of ‘‘OK’’ were taken for analysis. Measurements of the axial length (AL), central corneal thickness (CCT), mean keratometry (Km), astigmatism (AST), lens thickness (LT), and aqueous depth (AD)/anterior chamber depth (ACD) taken from each of the devices were used to evaluate for agreement between devices
Statistical analyses were performed using Stata version 12.1(StataCorp, College Station, TX, USA) statistical software. A P value < 0.05 was considered statistically significant. Repeatability was assessed by within-subject standard deviation (Sw), test–retest variability (TRT), and within-subject coefficient of variation (COV ¼ 100 3 Sw/overall mean).
RESULTS:
Fifty eyes of 22 female patients and 28 male patients were analyzed. There were 30 right eyes and 20 left eyes. Mean age of the patients was 60.2 + 10.05 years. The mean biometry parameters from different machines were as in table 1.
Table 1: Mean biometric measurements with the biometers.
| Nidek AL scan | Galilei G6 | Lenstar LS 900 | IOL Master 700 | |
| Axial length (mm) | 23.4 (22.7, 24.0) | 23.6 (23.1, 24.2) | 23.4 (23.0, 24.0) | 23.5 (22.9, 24.0) |
| CCT (microns) | 519 ± 33 | 534 ± 31 | 530 ± 33 | 534 ± 34 |
| ACD (mm) | 3.45 ± 0.30 | 3.50 ± 0.28 | 3.42 ± 0.32 | |
| Lens thickness (mm) | 3.99 (3.70, 4.37) | 3.88 (3.58, 4.16) | 3.78 (3.58, 4.26) | |
| K1 (diopters) | 43.3 ± 1.5 | 43.1 ± 1.7 | 43.2 ± 1.6 | 43.4 ± 1.6 |
| K2 (diopters) | 44.0 ± 1.5 | 43.9 ± 1.7 | 44.0 ± 1.6 | 44.1 ± 1.6 |
| Km (diopters) | 43.6 ± 1.5 | 43.5 ± 1.6 | 43.6 ± 1.6 | 43.7 ± 1.6 |
| Astigmatism | 0.59 (0.35, 0.95) | 0.76 (0.48, 1.14) | 0.59 (0.33, 0.98) | 0.55 (0.29, 0.87) |
| Astigmatism angle | 97 (81, 126) | 95 (75, 119) | 94 (81, 116) | 97 (78, 115) |
| AD | 2.98 ± 0.29 | 2.90 ± 0.31 | 2.88 ± 0.32 | |
| WTW (mm) | 12.0 ± 0.48 | 12.1 ± 0.39 | 12.1 ± 0.41 | 12.0 ± 0.48 |
In our study, Within subject standard deviation for axial length, K mean, White to White (WTW), Lens thickness, ACD was best with Lenstar LS 900 while that for central corneal thickness (CCT) was best with Nidek OPD3 scan as seen in figures 1 A-D.
Figure 1: Within subject standard deviation for Axial Length (1A), CCT (1B), Kmean (1C) and WTW (1D).
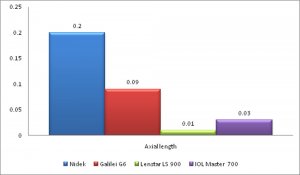
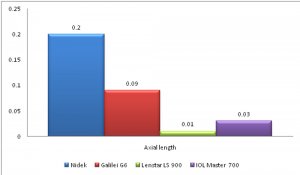 FIGURE 1A
FIGURE 1A
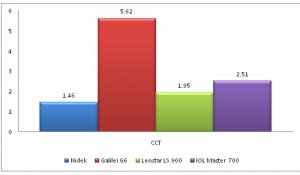
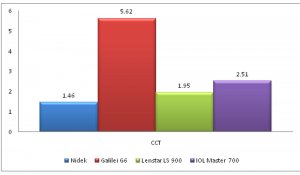
FIGURE 1B
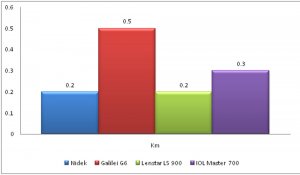
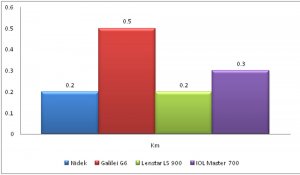
FIGURE 1C
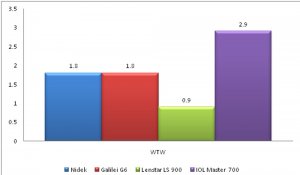
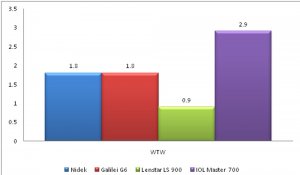
FIGURE 1D
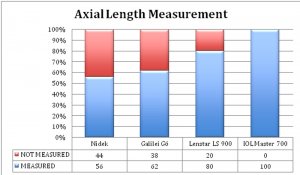
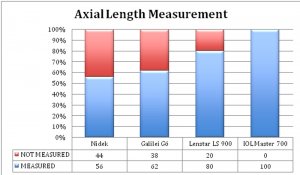
FIGURE 2: Percentage of eyes in which axial length was measured.
As seen in figures 3 (A-C), best agreement for axial length and WTW was found between Lenstar LS 900 and IOL Master 700 and for K mean was between Nidek and Lenstar LS 900.
Figure 3: Bland Altman plots showing best agreement for Axial Length (3A), WTW (3B), K mean (3C)
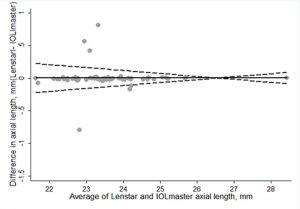
FIGURE 3A
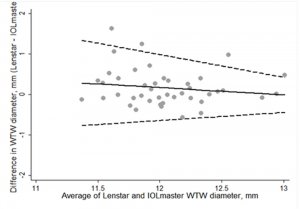
FIGURE 3B
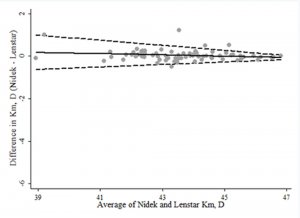
FIGURE 3C
DISCUSSION:
Accurate keratometry and axial length are the most important parameters for IOL power calculation before cataract surgery. Some of the newer generation formulae require ACD and WTW as well for more accurate IOL power calculation. The four machines we have compared work on different principles.
Individual instruments should be evaluated for their repeatability before they become widely applied in clinical practice. It is also necessary to compare the instruments with each other to check whether there is sufficient agreement for the devices to be used interchangeably in practice. Different methodologies cannot be considered equivalent if the degree of error has significant clinical implications.5, 6
In a study of 50 eyes comparing AL scan and IOL Master 500, Kaswin et al.7 reported comparable mean AL measurements (P = 0.70), and the correlation between the results was almost perfect (r = 0.999). The keratometry measurements were similar (P = 0.59, r= 0.701). In another study of 137 eyes conducted by Srivannaboon et al. 8, agreement between biometric measurements obtained with AL-Scan and IOL Master 500 was quite high, apart from WTW
values.
Several studies have compared IOL Master 500 and Lenstar 900. Holzer et al. 9 reported high correlations for AL and keratometry measurements (r = 0.9957 and r = 0.9859, respectively) but moderate correlation for ACD (r= 0.4456). Rohrer et al. 10 described high correlations for AL (r = 0.999), ACD (r = 0.875), and for corneal radius and the axis of the flattest radius (flattest radius, r = 0.927; steep radius, r = 0.929; axis of the flattest radius, r = 0.938). In another study, Hoffer et al.11 also found good correlations between AL, ACD, and K measurements in 50 eyes with cataract (r= 0.9995, r=0.8211, and r = 9959, respectively). The MAE in IOL power prediction was 0.455 + 0.32 D with the OLCR unit and 0.461 + 0.31 D with the PCI unit. 11
In our study axial length, WTW and ACD measurements were most repeatable with Lenstar LS 900; whereas CCT was most repeatable with AL scan. Among the 50 eyes included, AL scan could not measure axial length in 22 eyes, galilei could not measure in 19 and Lenstar LS 900 could not measure in 10 eyes (figure 2). Only those eyes where axial length was measurable by IOL Master 700 were included in study. None of the other biometers could measure axial length in eyes that IOL Master 700 could not, due to better penetration of IOL Master 700. Pachymetry measurements by AL scan were around 15 microns (p<0.001) lower compared to IOL master and Galilei. Axial length measurements by Galilei were 0.2mm (p<0.001) more than that by lenstar and AL scan. For most parameters IOL Master 700 measurements had good agreement with the measurements obtained by Lenstar LS 900.
In conclusion, IOL Master 700 showed valid measurements, good repeatability and good agreement with Lenstar LS 900, except axial length measurement. IOL Master 700 was better than other three devices in acquiring axial length measurements in denser cataracts due to better penetration. Overall, Lenstar LS 900 had the best repeatability in our study.
References:
1. Haigis W. Optical biometry using partial coherence interferometry. In: Shammas HJ, ed, Intraocular Lens Power Calculations. Thorofare, NJ, Slack, 2004; 141–157
2.Packer M, Fine IH, Hoffman RS, Coffman PG, Brown LK. Immersion A-scan compared with partial coherence interferometry; outcomes analysis. J Cataract Refract Surg 2002; 28:239–242
3.Holzer MP, Mamusa M, Auffarth GU. Accuracy of a new partial coherence interferometry analyzer for biometric measurements. Br J Ophthalmol 2009; 93:807–810
4.Buckhurst PJ, Wolffsohn JS, Shah S, Naroo SA, Davies LN, Berrow EJ. A new optical low coherence reflectometry device for ocular biometry in cataract patients. Br J Ophthalmol 2009; 93:943–953
5.Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986;1(8476):307–310.
6.Bland JM, Altman DG. Measuring agreement in method comparison studies. Stat Methods Med Res 1999;8(2):135–160.
7.Kaswin G, Rousseau A, Mgarrech M, Barreau E, Labetoulle M. Biometry and intraocular lens power calculation results with a new optical biometry device: Comparison with the gold standard. J Cataract Refract Surg 2014; 40:593–600.
8.S. Srivannaboon, C. Chirapapaisan, P. Chonpimai, and S. Koodkaew, “Comparison of ocular biometry and intraocular lens power using a new biometer and a standard biometer,” J Cataract Refract Surg, vol. 40, no. 5, pp. 709– 715, 2014.
9.Holzer MP, Mamusa M, Auffarth GU. Accuracy of a new partial coherence interferometry analyser for biometric measurements. Br J Ophthalmol 2009; 93:807–810
10.Rohrer K, Frueh BE, W€alti R, Clemetson IA, Tappeiner C, Goldblum D. Comparison and evaluation of ocular biometry using a new noncontact optical low-coherence reflectometer. Ophthalmology 2009; 116:2087–2092
11.Hoffer KJ, Shammas HJ, Savini G. Comparison of 2 laser instruments for measuring axial length. J Cataract Refract Surg 2010; 36:644–648