Dr. Vandana C
Nath, N05284, Dr. Shail, Dr. Vasavada
Abhaykumar Raghukant
Dr. Vandana Nath, Dr. Shail Vasavada, Dr. Abhay Vasavada
Iladevi Cataract & IOL Research Center, Raghudeep Eye Clinic, Gurukul Road, Memnagar, Ahmedabad, India.
Address :
Raghudeep Eye Hospital,
Gurukul Road, Memnagar,
Ahmedabad – 380052. India.
E-mail: info@raghudeepeyeclinic.com
Post operative visual outcomes with combined PhacoDSAEK surgery in eyes with Fuch’s dystrophy
Introduction:
Fuch,s Corneal Endothelial Dystrophy (FCED) is a degenerative disease of the corneal endothelium with accumulation of focal outgrowths called guttae (drops) and thickening of descemets membrane, leading to corneal edema and loss of vision.
As corneal edema progresses ,definitive treatment is surgical in the form of corneal transplantation. Until a few years back full thickness penetrating keratoplasty was the treatment of choice. Since 1998, new surgical modalities have been developed by G.Melles et al, called posterior lamellar keratoplasty or endothelial keratoplasty, evolving to Descemets Stripping Endothelial Keratoplasty (DSEK)/ Descemets Stripping Automated Endothelial Keratoplasty(DSAEK)1 , and more recently Descemets Membrane Endothelial Keratoplasty (DMEK)2
Cataract is often present in patients with fuchs dystrophy. Cataract surgery alone can exacerbate corneal swelling due to further endothelial cell loss. Combining cataract surgery with Descemets stripping automated endothelial keratoplasty is the treatment of choice in cases with visually significant cataract with advanced fuchs dystrophy.4
AIM:The aim of this study was to report visual outcomes of 15 eyes which underwent combined phacoemulsification with DSEK surgery in eyes with fuchs dystrophy
STUDY DESIGN: Interventional case series
MATERIALS AND METHOD: 15 eyes of 14 patients identified as advanced fuchsdystrophy , diagnosed on slit lamp biomicroscopy , specular microscopy, and pachymetry, with significant cataract were advised combined phaco with DSEK surgery. Eyes with other comobidities were not included. Age of patients ranged from 59 to 80 years and male : female ratio was 1:3. Grading of cataract was done by LOCS Classification, wherein 4 eyes had grade 2 to3 cataract, and 11 eyes had advanced grade 4 ,brunescent to black cataracts. Fuchs dystrophy was seen as confluent guttae in the central cornea in all eyes with beaten metal appearance of endothelial surface on slit lamp examination. Specular microscopy showed pleomorphism and polymegathism of endothelial cells with cell densitiy of less than 1000/mm2 and 0 hexagonality in 8 eyes. Specular microscopy could not be captured in 7 eyes with advanced corneal edema and epithelial bullae. 11 eyes had pachymetry greater than 600 microns. 3 eyes had pachymetry of 550 to 600 microns, measured on anterior segment OCT.(VISANTE OCT).
Pre operative investigations included: manual keratometry, Itrace aberrometry, Pentacam, Optical biometry with IOL master, immersion biometry ,posterior segment OCT, in addition to specular microscopy and AS OCT Scans. Pre and post operative slit lamp photo documentation was done in all eyes.
IOL power calculation was done using SRK-T formula with a target refraction of -1 to -1.5 diopter .
DONOR TISSUE: Donor cornea was pre cut at the Ramayamma International Eye bank , LV Prasad eye institute , Hyderabad, using a Moria microkeratome . Graft thickness varied according to the donor graft pachymetry. The corneas were air transported maintaining the cold chain .
A pre cut donor tissue was trephined to 8 mm graft size , using the indo German corneal punch .
Range of donor graft thickness was 83 microns(thinnest) to 150 microns(thickest).
A conjunctival peritomy was done and cauterization was done.
A temporal scleral tunnel was made using a 15 gauge BP knife and dissected with a crescent knife, 0.5 to 1mm away from the limbus. Internal entry was done using a 2.2 mm knife and phacoemulsificatin was done with a standardized closed chamber technique with a cohesive viscoelastic. Bimanual irrigation aspiration was used for the cortical clean up, through 2 side port incisions of 1mm each. A single piece hydrophobic acrylic IOL (Acrysof SA60AT), Alcon labs, was implanted in the bag. Viscoelastic was removed from behind the IOL .
Trypan Blue stain was injected to stain the descemets membrane. A cohesive viscoelastic was injected in the anterior chamber (Provisc), and descemets membrane was stripped using Thomas John,s descemets membrane stripper. A 1.5 mm clear corneal incision was made opposite the scleral tunnel to facilitate insertion of a Tan endoglide forceps for pulling the donor cornea.
Scleral incision was enlarged to 5mm and donor graft was pulled into a Tan endoglide cartridge. The anterior chamber was irrigated to clear the viscoelastic and an anterior chamber maintainer was inserted(Bluementhal). Tan endoglide was introduced through the scleral tunnel and donor graft pulled using a Tan forceps for ultra thin grafts in the anterior chamber. Air was injected to allow the donor cornea to stick to the host cornea. The Golden Double – Ring sign was the indicator of graft adherence to the host cornea7.The scleral tunnel was sutured with 10-0 nylon suture. Conjunctiva was sutured with the same suture. Topical moxifloxacin drops were put and the eye was patched . The patient was asked to be in supine position for 2 hours post operatively.Topical regimen followed was prednisolone eye drops, antibiotic eye drops, atropine eye drops, timolol eye drops, oral paracetamol .Patients were asked to follow up the next day .Post operative AS OCT was done for graft adherence in all quadrants, pachymetry, IOL position. Photo documentation was done. Patients were followed up at 3 days, 1 week, 1 month ,3 months and 6 months.
RESULTS: All patients were counselled pre operatively regarding the nature of the condition of the eye requiring a combined phaco and DSEK procedure. Possibility of graft detachment was explained.Possibility of graft failure and graft rejection was explained. Lifelong medication and follow up was advised.
Intraopertively all had uneventful phaco and donor graft insertion with minimal manipulation of the graft in the anterior chamber.
Post operatively , all had adhered grafts , and no patient needed a repeat air injection.5 All eyes had an increase of pachymetry on day 1, which reduced by 1 week. All grafts were clear at the end of 1 month. Visual acuity was taken at 3 months and final refraction done at the end of 6 months
VISUAL OUTCOME:
At the end of 6 months 5 eyes achieved best corrected vision of 6/9 (snellens vision), 4 eyes had 6/12, 3 eyes had 6/18, 1 eye had 6/24, 2 eyes had 6/60 .
60 percent achieved >6/12 vision, 20 percent achieved 6/18 vision, 20 percent had 6/24 or less.
DISCUSSION:
Cataract with fuchs dystrophy poses a dilemma to many surgeons. Many surgeons advocate a staged procedure , where the cataract surgery is performed first ,followed by DSEK after 1 to 2 months or later.6 This allows the IOL to stick firmly in the bag by capsule fibrosis, before performingDSEK.
Improved surgical instrumentation forDSEK, such as donor graft injectors and technical improvements in the surgical technique have facilitated reduced complications and better outcomes ofDSEK . These key technical improvements are primarily aimed at allowing graft insertion with the least possible damage to donor endothelial cells, thereby deliveringthe greatest load of fully functional endothelial cells to the patients eye.
In our series of 15 eyes it was noted that visual outcomes were better in thinner donor grafts. This is comparable to other studies comparing DMEK to DSEK, where DMEK visual outomes were better than dsek.3 However the learning curve for DMEK is steeper , and chances of graft dislocation and failure were comparable.
More speculative future directions in treatment of FCED include in vitro expansion of human corneal endothelial ceels for transplantation, artificial corneas (keratoprosthesis), and genetic modification.
No graft surgery where the central diseased endothelium is stripped off ,but not replaced with donor tissue has also shown some promise in selected patients. Visual recovery is thought to occer due to peripheral endothelial cell migration to denuded area of cells.
What is very promising is the effect of Rho kinase (ROCK) inhibition on endothelial cell division and proliferation. ROCK inhibition may offer a viable medical treatment or cell therapy for fuchs endothelial dystrophy within the next decade.
CONCLUSION:
Combined Phaco and DSEK gave good visual outcomes in patients with fuchs dystrophy. The advantage was a single surgical procedure with faster visual recovery.
In the title DSAEK is mentioned , rest of the places it is mentioned as DSEK
Please clarify .
REFERENCES:
- YakovGoldich, Mahmood Showail, NOA Avni – Zaberman, Maurico Perez, Randall Ulate, Uri Elaz and David Rootman.Contralateral Eye Comparison of Descemet MembraneEndothelial Keratoplasty and Descemet StrippingAutomated Endothelial Keratoplasty.Am J Ophthalmol. 2015 Jan;159(1):155-9
2.Theofilos Tourtas, Kathrin Laaser, Bjoern Bachmann, Claus Cursiefen and Friedrich E. Kruse.Descemet Membrane Endothelial Keratoplasty Versus Descemet Stripping Automated Endothelial Keratoplasty Am J Ophthalmol. 2012 Jun;153(6):1082-90
3.Mark A. Terry, Michael D. Straiko, Jeffrey M. Goshe, Jennifer Y. Li, David Davis-Boozer,Descemet’s Stripping Automated EndothelialKeratoplasty: The Tenuous Relationshipbetween Donor Thickness and PostoperativeVision.Ophthalmology. 2012 Oct;119(10):1988-96
4.Terry MA. Endothelial Keratoplasty for Fuch’s Dystrophy with cataract : Complications and clinical results with the new triple procedure. Ophthalmology 2009 ; April : 116 (4) : 631 – 9.
5.Vaddavalli PK, Diakonis VF, Canto AP. et al. Factors affecting DSAEK graft lenticle adhesion : an in vitro experimental study. Cornea 2014 ; June ; 33 (6) : 551 – 4.
6.Sykakis E, Lam FC, Georgoudis P et al. Patients with Fuchs Endothelial Dystrophy and cataract undergoing Descemet stripping automated endothelial keratoplasty and phacoemulsificatin with Intraouclar lens Implant : Staged versus Combined procedure outcomes. J Ophthalmol 2015 ; 2015 : 172075.
7.Delfazayaebaher S, Feizi S, Javadi MA et al. Double – Ring Sign to confirm correct orientation ofDonor Lenticules during Descemet Stripping Automated Endothelial Keratoplasty. Cornea 2015 ; Aug : 34 (8) : 980 – 4.
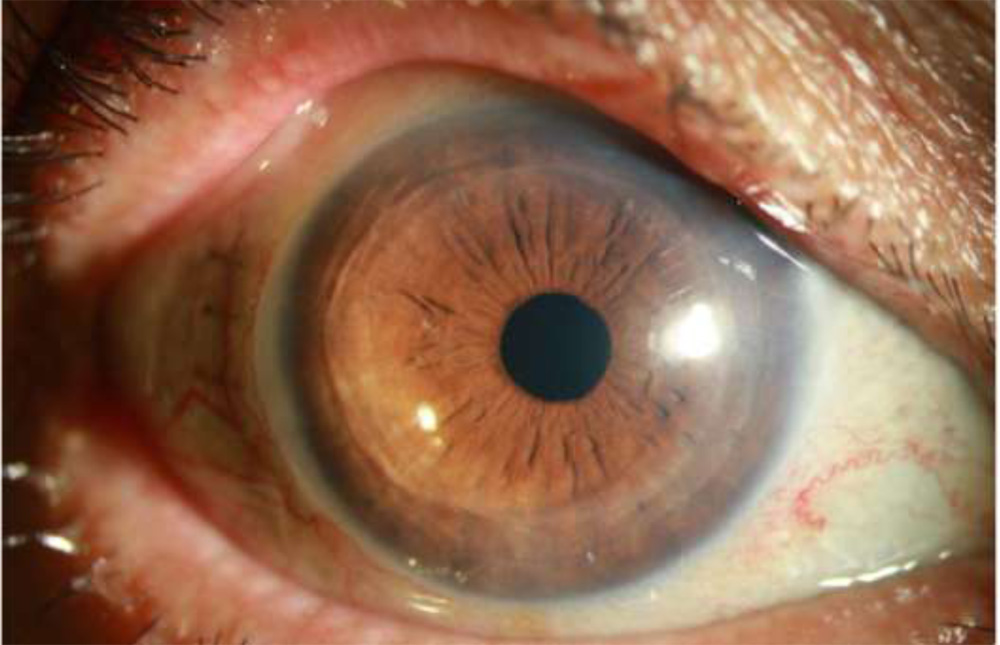
6 Months Post op. Phaco + DSAEK combined Surgery.