Dr. Santosh Kumar, K10815Dr. Brig (Mrs ) Sagarika
Patyal, Dr. Sanjay Kumar Mishra, Dr. Vijay Kumar
Sharma
TYPE OF ARTICLE: Original
AUTHOR :
K10815 Dr Santosh Kumar
CO- AUTHORS :,
P05829 Brig(Mrs) SagarikaPatyal
M08300 Col(Dr) Sanjay Kumar Mishra
S15007 Lt Col Vijay Kumar Sharma
PURPOSE :
Aim – To ascertain the efficacy of UBM in secondary sulcus IOL implantation in aphakes.
KEYWORDS: Aphakia, IOL implantation, ultrasound biomicroscopy (UBM)
INTRODUCTION
Ultrasound biomicroscopy (UBM) is a high resolution ultrasound technique used for imaging of structural details of anterior segment at near microscopic resolution. It provides for detailed 2-D gray scale images of conjunctiva, cornea and anterior sclera, anterior chamber and angle structures, ciliarybody, crystalline lens, zonules, capsular remnants and anterior vitreous. The frequency of UBM used is 50MHz whereas conventional ultrasound is 7.5-10 MHz. providing cross sectional images of anterior segment structures. The detailed images give a lateral resolution of 59 µ , axial resolution of 25µ and depth of penetration of 4-5mm(upto pars plana).
MATERIALS AND METHODS :
A prospective case analysis of 20 cases of surgically induced or post traumatic aphakia who were taken up for secondary sulcus IOL implantation from Jun2013 to Mar 2016. All the patients were in the age group of 48-72yrs. 14 cases were post-surgical aphakia whereas 06 cases were post-traumatic. All the patients were subjected to a detailed pre-operative examination which consisted of :
a) Logmar visual acuity (unaided and aided)
b) Cornea
c) Anterior chamber depth and any evidence of inflammation
d) Iris tissue details and pupillary size and configuration
e) Dilated eye examination for anterior/posterior capsular support.
Inclusion criteria
All cases where the capsular remnants could not be seen either due to inadequate pupillary dilatation or only the most peripheral capsular remnants were present which could not be visualized on slit lamp examination.
Thus before implantation of intraocular lens on the remnants of the capsule in patients with inadequate pupillary dilatation, a confirmation as regards the status of lens capsule was imperative. We resorted to a preoperative ultrasound biomicroscopy in all patients to assess the capsular integrity. On ultrasound biomicroscopy with a 50Hz probe, the extent of capsule present could easily be quantified and was meticulously documented. Only those patients were included for study who had at least 03 clock hours of capsular integrity and similar one 180° opposite as confirmed on ultrasound biomicroscopy. All surgeries were performed by a single surgeon.
A large 7mm limbal incision, 90° away from the intact capsular remnants was made. A good anterior vitrectomy was performed and a single piece all PMMA IOL with 6.5mm optic and 13mm overall length was used. Hydroxypropylmethyl cellulose was injected behind the iris to increase the space in the sulcus for assisting in easy IOL implantation. The haptics were placed over the capsular remnants which had been identified preoperatively by UBM. Anterior chamber was washed off the viscoelastic and anterior chamber was formed with air. The limbal wound was sutured with 5 sutures of 10’0 polyamide.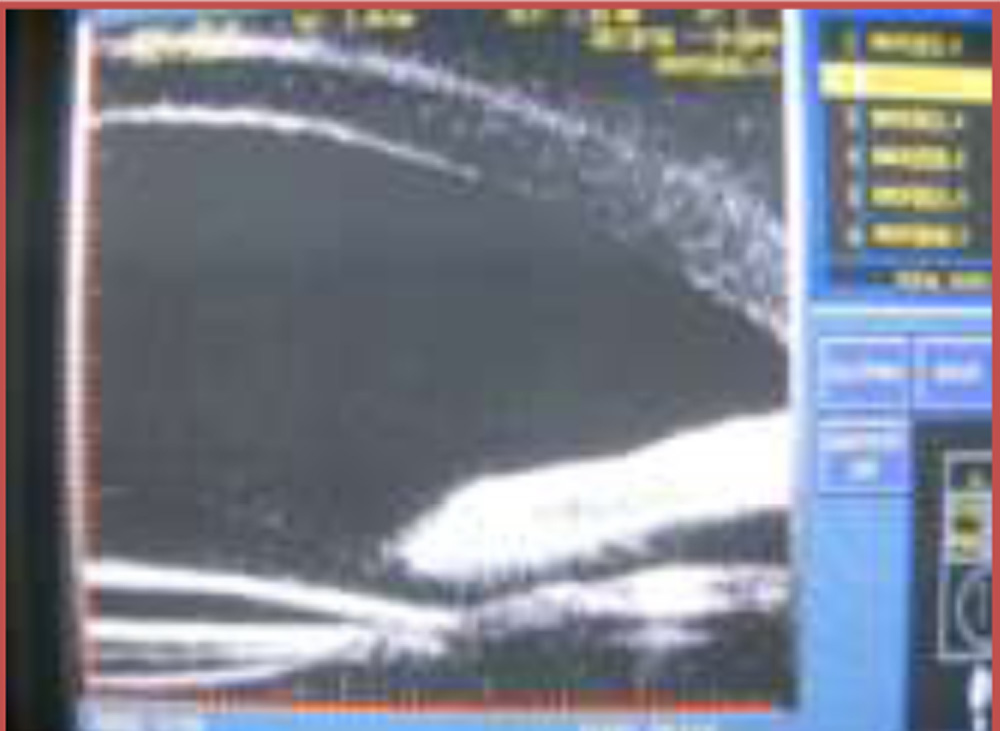
The exclusion criteria was –
a) Dislocated IOL
b) Traumatic cataract
c) Pseudoexfoliation
d) Uveitis
e) Glaucoma
f) Corneal opacity
g) High myopia
h) Small pupils
Postoperatively the patients were examined on day 1,2,7,14 and 30 and detailed slit lamp evaluation was done.
On day 30 an UBM was done to see the location of IOL and the haptics and all cases had the haptics resting on capsular remnants.
RESULTS:
Secondary IOL implantation in sulcus over the capsular remnants could be achieved in 18 out of 20 patients (90%). In 02 patients there was intraoperative difficulty in implantation of IOL which was managed with glued IOL implantation at the same sitting.
DISCUSSION:
In this case series we were able to implant an PMMA intraocular lens in sulcus in 90% patients which would have otherwise required a more complex surgery like glued IOL or iris fixated IOL. Thus ultrasound biomicroscopy is an excellent modality for assessing anterior capsular integrity prior to secondary IOL implantation. Preoperatively an ultrasound biomicroscopy exactly delineates the available capsular support for placing the haptics especially in non dilating pupils.Without the ultrasound biomicroscopyin all such patients with aphakia, one would be in a dilemma whether to attempt secondary IOL without quantification of the remnants of the anterior capsule based only on slit lamp examination.The procedure can easily be performed and easily adopted by majority of surgeons.
CONCLUSION :
A pre-operativeultrasound biomicroscopywould obviate the need for a more challenging procedure like scleral/iris fixation of IOL and aid in a more physiological sulcus placement which could be easily performed by majority of anterior segment surgeons. In the absence of ultrasound biomicroscopy revealing the extent of capsular support,all these cases would be subjected to scleral/iris fixation of IOL.The sulcus IOL implantation is thus a simple proposition as compared to more challenging surgeries as glued IOL, scleral fixated IOL or iris fixated IOL implantation for management of aphakia. Thus the importance of doing ultrasound biomicroscopy in cases of aphakia where the capsular remnants could not be identified fully on slit-lamp examination but still could be taken up for intraocular lens implantation.
Postoperatively the patients were examined on day 1,2,7,14 and 30 and detailed slit lamp evaluation was done.
On day 30 an UBM was done to see the location of IOL and the haptics and all cases had the haptics resting on capsular remnants.
RESULTS:
Secondary IOL implantation in sulcus over the capsular remnants could be achieved in 18 out of 20 patients (90%). In 02 patients there was intraoperative difficulty in implantation of IOL which was managed with glued IOL implantation at the same sitting.
DISCUSSION:
In this case series we were able to implant an PMMA intraocular lens in sulcus in 90% patients which would have otherwise required a more complex surgery like glued IOL or iris fixated IOL. Thus ultrasound biomicroscopy is an excellent modality for assessing anterior capsular integrity prior to secondary IOL implantation. Preoperatively an ultrasound biomicroscopy exactly delineates the available capsular support for placing the haptics especially in non dilating pupils.Without the ultrasound biomicroscopyin all such patients with aphakia, one would be in a dilemma whether to attempt secondary IOL without quantification of the remnants of the anterior capsule based only on slit lamp examination.The procedure can easily be performed and easily adopted by majority of surgeons.
CONCLUSION :
A pre-operativeultrasound biomicroscopywould obviate the need for a more challenging procedure like scleral/iris fixation of IOL and aid in a more physiological sulcus placement which could be easily performed by majority of anterior segment surgeons. In the absence of ultrasound biomicroscopy revealing the extent of capsular support,all these cases would be subjected to scleral/iris fixation of IOL.The sulcus IOL implantation is thus a simple proposition as compared to more challenging surgeries as glued IOL, scleral fixated IOL or iris fixated IOL implantation for management of aphakia. Thus the importance of doing ultrasound biomicroscopy in cases of aphakia where the capsular remnants could not be identified fully on slit-lamp examination but still could be taken up for intraocular lens implantation.